

- Department of Neurosurgery, Maastricht University Medical Center, PO box 5800, 6202AZ Maastricht, The Netherlands
Correspondence Address:
R. Goes
Department of Neurosurgery, Maastricht University Medical Center, PO box 5800, 6202AZ Maastricht, The Netherlands
DOI:10.4103/2152-7806.157948
Copyright: © 2015 Goes R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Goes R, Overbeeke Jv. A vertebral extra dural chordoma at C5, possibly deriving from a clival chordoma. Surg Neurol Int 01-Jun-2015;6:94
How to cite this URL: Goes R, Overbeeke Jv. A vertebral extra dural chordoma at C5, possibly deriving from a clival chordoma. Surg Neurol Int 01-Jun-2015;6:94. Available from: http://surgicalneurologyint.com/surgicalint_articles/vertebral-extra-dural-chordoma-c5-possibly-deriving/
Abstract
Background:Clival chordomas are a rare type of cancer with low metastatic potential and primary metastasize to the lung or bones.
Case Description:This case report describes a possible metastatic, paravertebral chordoma at level C4-C5 in a patient with a past medical history of a clival chordoma.
Conclusion:Chordomas are unpredictable and may metastasise.
Keywords: Clivus, chordoma, metastatic, vertebral
INTRODUCTION
Deriving from the embryonic remnants of the notochord, chordomas are a rare type of cancer. They account for 1–4% of all primary bone tumors.[
CASE REPORT
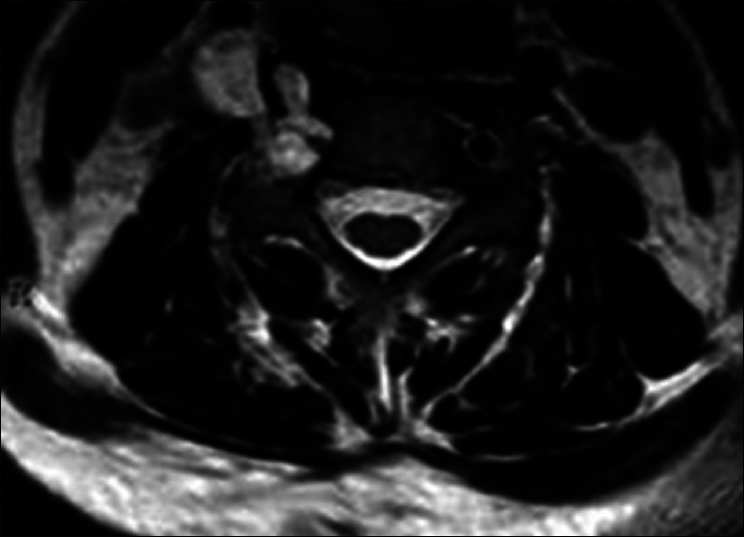
We present a 52-year-old patient with a medical history of clival chordoma. In 2009 the patient underwent a partial resection of a lower clival chordoma expanding until level C2. Six months after surgery, before proton beam could be realized, a second postoperative magnetic resonance imaging (MRI) showed a regrowth of the remnant. A second resection in 2010 and additional proton beam therapy on the postoperative remnant was performed. In 2012, an intracutaneous chordoma in the medial right neck was surgically resected. Routine MRI showed no tumor growth until 2013, when a mass at level C4-C5, suspected for a recurrent chordoma [
Neurologic examination revealed a slight weakness of the right deltoid muscle.
Imaging
The MRI shows an extravertebral 3 cm lobular process extending in the foramen of C4/C5. This foramen is slightly wider than normal. The right carotid artery shows no flow on MRI, suggesting an obstruction of this artery. A computed tomography (CT) scan confirmed a widening of the neural foramen.
Surgery
At surgery, the tumor appeared as a grayish, rather solid, encapsulated mass. The tumor infiltrated the neuroforamen of C4-C5 and infiltrated the C5 nerve root. The vertebral artery had a small caliber and was compressed by the tumor. Considering the medical history, the tumor was macroscopically suspected as a chordoma, however, a schwannoma could not be excluded, intraoperative pathological examination could not confirm the diagnosis of a chordoma. Therefore the tumor was incomplete resected avoiding further damage to the C5 nerve root, thereby leaving a remnant in the C4-C5 neural foramen. This remnant was treated with proton beam therapy.
Pathology
The overall conclusion of the histological examination confirmed the diagnosis chordoma.
DISCUSSION
Chordomas arise from remnants of the notochord. The notochord forms during embryologic development, remnants can occur all along the spinal column. Chordomas are rare and account for 1–4% of all bone tumors, 25–35% of them arise from the clivus. Chordomas are known for their capacity to regrow at the primary site and seeding in the surgical pathway, however, they are considered to have a low metastatic potential.[
Our case is especially rare as the patient previously had a subdermal chordoma, prior to the cervical chordoma. To our knowledge, this is the first paper reporting multiple metastatic chordomas in different tissue types out of the vicinity of the surgical field.
There are a number of possibilities for the occurrence of chordoma in the cervical vertebrae; a new primary tumor or metastatic tumor.
Primary chordomas that originate from the cervical vertebrae account for about 6–7% of all primary chordomas.[
Metastasis are uncommon for clival chordomas, as 73% of the metastatic chordomas originate from the sacrococcygeal region, and most frequently appear in lung, liver, lymph node, or bone.[
The question remains why chordomas recur or metastasise? Can this be explained from a genetic or cellular point of view? Almefty et al. suggest that abnormal karyotypes are associated with a poor prognosis and more importantly tumor progression. They found that abnormalities in chromosome 3, 4, 12–14 are associated with an increased likelihood for recurrence.[
CONCLUSION
This case report underlines the unpredictability of clival chordomas and their possible metastatic potential.
References
1. Almefty KK, Pravdenkova S, Sawyer JR, Al-Mefty O. Impact of cytogenetic abnormalities on the management of skull base chordomas: Clinical article. J Neurosurg. 2009. 110: 715-24
2. Aydemir E, Bayrak OF, Sahin F, Atalay B, Kose GT, Ozen M. Characterization of cancer stem-like cells in chordoma: Laboratory investigation. J Neurosurg. 2012. 116: 810-20
3. Barrenechea IJ, Perin NI, Triana A, Lesser J, Costantino P, Sen C. Surgical management of chordomas of the cervical spine. J Neurosurg Spine. 2007. 6: 398-406
4. Boyette JR, Seibert JW, Fan CY, Stack BC. The etiology of recurrent chordoma presenting as a neck mass: Metastasis vs. surgical pathway seeding. Ear Nose Throat J. 2008. 87: 106-9
5. Chambers KJ, Lin DT, Meier J, Remenschneider A, Herr M, Gray ST. Incidence and survival patterns of cranial chordoma in the United States. Laryngoscope. 2014. 124: 1097-102
6. Chugh R, Tawbi H, Lucas DR, Biermann JS, Schuetze SM, Baker LH. Chordoma: The nonsarcoma primary bone tumor. Oncologist. 2007. 12: 1344-50
7. Jain BB, Datta S, Roy SG, Banerjee U. Skull base chordoma presenting as nasopharyngeal mass with lymph node metastasis. J Cytol. 2013. 30: 145-7
8. Jiang L, Liu ZJ, Liu XG, Ma QJ, Wei F, Lv Y. Upper cervical spine chordoma of C2-C3. Eur Spine J. 2009. 18: 293-300
9. Lim JJ, Kim SH, Cho KH, Yoon DH, Kim SH. Chordomas involving multiple neuraxial bones. J Korean Neurosurg Soc. 2009. 45: 35-8
10. McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM. Chordoma: Incidence and survival patterns in the United States, 1973–1995. Cancer Causes Control. 2001. 12: 1-11
11. Sawyer JR, Husain M, Al-Mefty O. Identification of isochromosome 1q as a recurring chromosome aberration in skull base chordomas: A new marker for aggressive tumors?. Neurosurg Focus. 2001. 10: 1-6
12. Uggowitzer M, Kugler C, Groell R, Lindbichler F, Radner H, Sutter B. Drop metastases in a patient with a chondroid chordoma of the clivus. Neuroradiology. 1999. 41: 504-7
13. van Lierop AC, Fagan JJ, Taylor KL. Recurrent chordoma of the palate occurring in the surgical pathway: A case report. Auris Nasus Larynx. 2008. 35: 447-50
14. Walcott BP, Nahed BV, Mohyeldin A, Coumans JV, Kahle KT, Ferreira MJ. Chordoma: Current concepts, management, and future directions. Lancet Oncol. 2012. 13: e69-76
15. Walter BA, Begnami M, Valera VA, Santi M, Rushing EJ, Quezado M. Gain of chromosome 7 by chromogenic in situ hybridization (CISH) in chordomas is correlated to c-MET expression. J Neurooncol. 2011. 101: 199-206
16. Zemmoura I, Ismail MB, Travers N, Jan M, François P. Maxillary surgical seeding of a clival chordoma. Br J Neurosurg. 2012. 26: 102-3


Mark Soo
Posted July 27, 2015, 10:01 am
Congratulations! Excellent paper on a very rare condition indeed.