

- Department of Neurosurgery, Oregon Health and Science University, Portland, Oregon, United States.
- Department of Neurosurgery, University of California at San Francisco, San Francisco, California, United States.
Correspondence Address:
Brannan E. O’Neill
Department of Neurosurgery, Oregon Health and Science University, Portland, Oregon, United States.
DOI:10.25259/SNI_50_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Brannan E. O’Neill1, Thomas Wozny2, Kutluay Uluc1, Jesse J. Liu1. Acute nontraumatic subdural hematoma from ruptured accessory meningeal artery pseudoaneurysm. 26-Apr-2021;12:186
How to cite this URL: Brannan E. O’Neill1, Thomas Wozny2, Kutluay Uluc1, Jesse J. Liu1. Acute nontraumatic subdural hematoma from ruptured accessory meningeal artery pseudoaneurysm. 26-Apr-2021;12:186. Available from: https://surgicalneurologyint.com/surgicalint-articles/10757/
Date of Submission
19-Jan-2021
Date of Acceptance
01-Apr-2021
Date of Web Publication
26-Apr-2021
Abstract
Background: Cerebral angiography including internal and external carotid artery injections is crucial in young patients with a spontaneous subdural hematoma.
Case Description: We present the first reported case of an accessory meningeal artery aneurysm in a 46-year-old male with a history of hypertension that led to a spontaneous nontraumatic acute subdural hematoma. A PubMed review of the literature was performed using a keyword search to identify cases examining nontraumatic spontaneous intracranial hematomas related to meningeal artery aneurysms. The literature review summarizes all published reports of middle meningeal artery aneurysms resulting in nontraumatic acute intracranial bleeds. The patient underwent successful coiling of the accessory meningeal artery.
Conclusion: We propose endovascular treatment for accessory meningeal artery aneurysms and emphasize the utility of angiography of internal and external carotid arteries in a patient with an unexplained intracranial hematoma.
Keywords: Angiography, Meningeal artery aneurysm, Spontaneous subdural hematoma
INTRODUCTION
A nontraumatic acute subdural hematoma can be caused by rupture of a vascular malformation or of an intracranial aneurysm into the subdural space. There are several reports of nontraumatic subdural hematomas secondary to aneurysms that have an internal carotid artery (ICA) distribution.[
Aneurysms of external carotid artery distribution that is intracranial are rare. When present, they are diagnosed commonly in symptomatic patients. Few cases of middle meningeal artery (MMA) aneurysms leading to acute nontraumatic subdural hematoma have been described.[
The case described here is the first report, to our knowledge, to detail a nontraumatic acute subdural hematoma secondary to rupture of a pseudoaneurysm of the accessory MMA. Subsequently, the case was managed with endovascular coiling. Cerebral angiography including internal and external carotid artery injections is crucial, especially in young patients with a spontaneous subdural hematoma. A literature review is also presented.
CASE REPORT
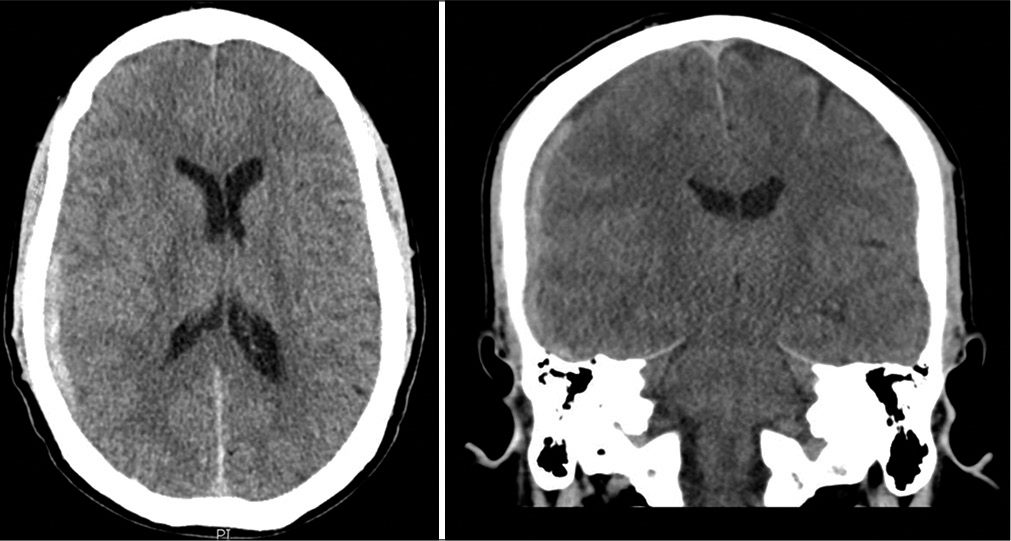
A 46-year-old male with a history of hypertension was transferred to our facility after presenting with an 11-day history of nausea and vomiting after waking up with a right-sided sharp headache. The patient reported taking ibuprofen for the headache without significant relief. As a result of the ongoing headache, head computed tomography (CT) was obtained. The head CT revealed a right-sided acute subdural hematoma [
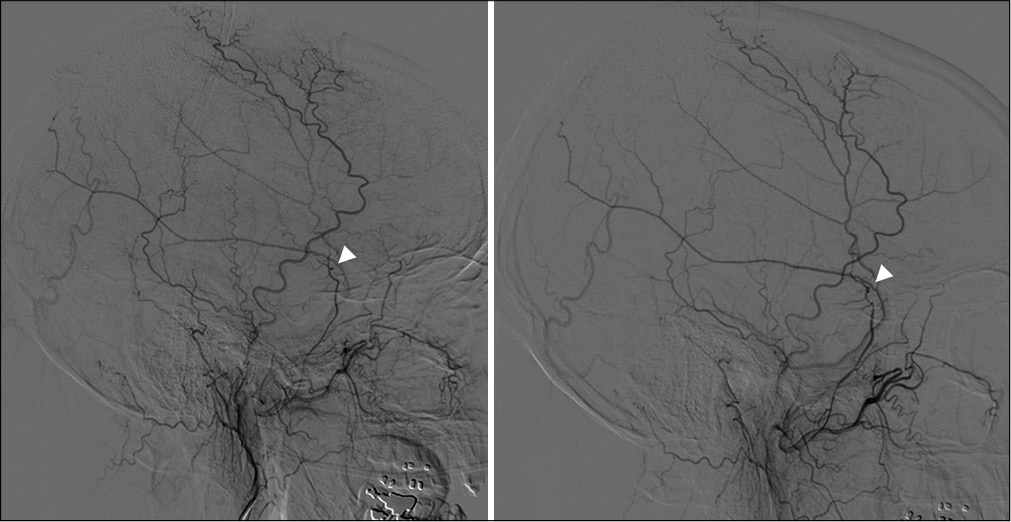
A diagnostic cerebral angiogram including careful evaluation of the external and ICA circulations was undertaken. This revealed a small pseudoaneurysm of the right accessory MMA [
Literature analysis
A literature search of the PubMed/Medline databases was performed using the algorithm (“meningeal artery aneurysm” OR “spontaneous subdural hematoma” AND “nontraumatic”). Article titles and abstracts were then individually screened to populate articles of interest, and selected manuscripts were recorded digitally and tracked. To mitigate publication bias, referenced articles were utilized to identify other case reports and case series.
DISCUSSION
The first reported case of a MMA aneurysm was published by Berk in 1961; they described a 73-year-old female with Paget’s disease who presented without trauma and endorsement of a 6-month headache.[
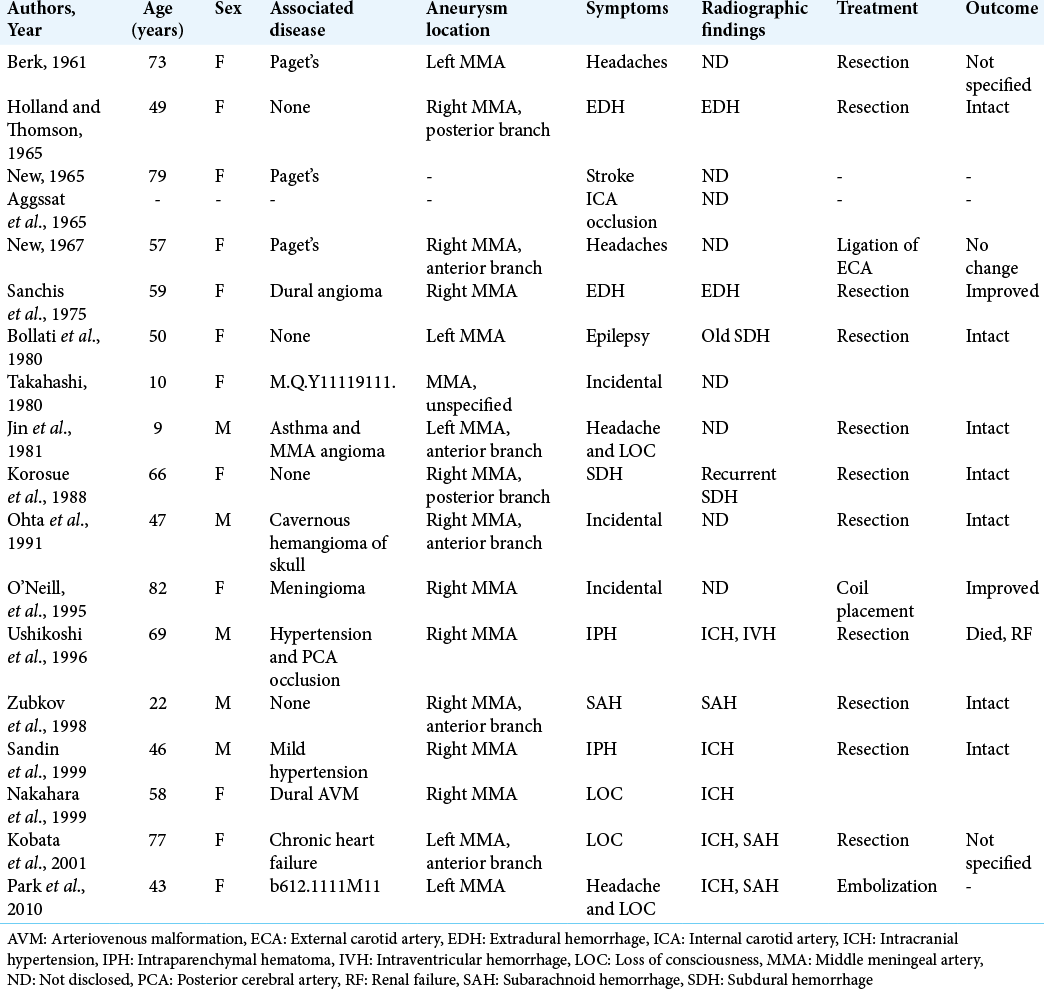
To the best of our knowledge, there are no cases of an accessory meningeal artery aneurysm described in the literature. Given the rarity and unclear natural history of the aneurysms of the external carotid artery circulation, clinical decision-making can be challenging. Several studies recommend endovascular treatment of these aneurysms due to bleeding risk.[
CONCLUSION
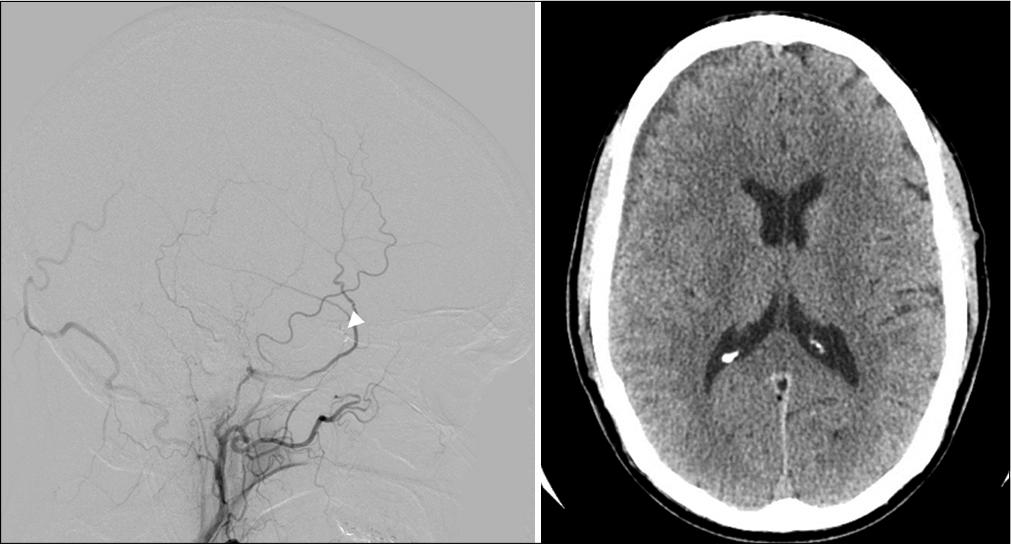
To the best of our knowledge, this is the first reported case of an accessory meningeal artery aneurysm causing a nontraumatic acute subdural hematoma. Angiography of the external carotid arteries allowed for the detection of a small accessory meningeal artery pseudoaneurysm in this patient, and after successful embolization of the lesion, the vessel was obliterated and the hematoma improved significantly on follow-up imaging.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Awaji K, Inokuchi R, Ikeda R, Haisa T. Nontraumatic pure acute subdural hematoma caused by a ruptured cortical middle cerebral artery aneurysm: Case report and literature review. NMC Case Rep J. 2016. 3: 63-6
2. BERK ME. Aneurysm of the middle meningeal artery. Br J Radiol. 1961. 34: 667-8
3. Bollati A, Galli G, Gandolfini M, Orlandini A, Gualandi GF. True aneurysm of the middle meningeal artery. Case report. J Neurosurg Sci. 1980. 24: 89-92
4. Gong J, Sun H, Shi XY, Liu WX, Shen Z. Pure subdural haematoma caused by rupture of middle cerebral artery aneurysm: Case report and literature review. J Int Med Res. 2014. 42: 870-8
5. Holland HW, Thomson JL. Aneurysm of the middle meningeal artery. Clin Radiol. 1965. 16: 334-8
6. Jin KH, Toyoda S, Kumagai K, Hashimoto T, Abe Y, Suzuki K. Non-traumatic middle meningeal aneurysm and angioma in a child. Brain Dev. 1981. 3: 323-8
7. Kähärä VJ. Middle meningeal artery aneurysm. Case illustration. J Neurosurg. 1999. 91: 518
8. Kobata H, Tanaka H, Tada Y, Nishihara K, Fujiwara A, Kuroiwa T. Intracerebral hematoma due to ruptured nontraumatic middle meningeal artery aneurysm--case report. Neurol Med Chir (Tokyo). 2001. 41: 611-4
9. Korosue K, Kondoh T, Ishikawa Y, Nagao T, Tamaki N, Matsumoto S. Acute subdural hematoma associated with nontraumatic middle meningeal artery aneurysm: Case report. Neurosurgery. 1988. 22: 411-3
10. Nakahara I, Taki W, Kikuchi H, Sakai N, Isaka F, Oowaki H. Endovascular treatment of aneurysms on the feeding arteries of intracranial arteriovenous malformations. Neuroradiology. 1999. 41: 60-6
11. New PF. True aneurysm of the middle meningeal artery, cranial Paget’s disease and hypertension: A triad. Clin Radiol. 1967. 18: 154-7
12. New PF. True aneurysm of the middle meningeal artery. Clin Radiol. 1965. 16: 236-40
13. Ohta H, Tanazawa T, Osuka K, Ito Y, Fukatsu T. True aneurysms of the middle meningeal artery associated with cavernous hemangioma of the skull--case report. Neurol Med Chir (Tokyo). 1991. 31: 203-5
14. O’Neill OR, Barnwell SL, Silver DJ. Middle meningeal artery aneurysm associated with meningioma: Case report. Neurosurgery. 1995. 36: 396-8
15. Park YS, Suk JS, Kwon JT. Repeated rupture of a middle meningeal artery aneurysm in moyamoya disease. Case report. J Neurosurg. 2010. 113: 749-52
16. Sanchis JF, Orozco M, Cabanes J. Spontaneous extradural haematomas. J Neurol Neurosurg Psychiatry. 1975. 38: 577-80
17. Sandin JA, Salamat MS, Baskaya M, Dempsey RJ. Intracerebral hemorrhage caused by the rupture of a nontraumatic middle meningeal artery aneurysm. Case report and review of the literature. J Neurosurg. 1999. 90: 951-4
18. Takada T, Yamamoto T, Ishikawa E, Zaboronok A, Kujiraoka Y, Akutsu H. Acute subdural hematoma without subarachnoid hemorrhage caused by ruptured A1-A2 junction aneurysm. Case report. Neurol Med Chir (Tokyo). 2012. 52: 430-4
19. Takahashi M, Saito Y, Konno K. Intraventricular hemorrhage in childhood moyamoya disease. J Comput Assist Tomogr. 1980. 4: 117-20
20. Ushikoshi S, Houkin K, Itoh F, Saitoh H, Nozaki M, Kuroda S. Ruptured aneurysm of the middle meningeal artery associated with occlusion of the posterior cerebral artery. Case report. J Neurosurg. 1996. 84: 269-71
21. Zingesser LH, Schechter MM, Rayport M. Truths and untruths concerning the angiographic findings in extracerebal haematomas. Br J Radiol. 1965. 38: 835-47
22. Zubkov YN, Matsko DE, Pak VA. Saccular aneurysms of meningeal artery: Case report. Neurosurgery. 1998. 42: 664-6

