

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran.
DOI:10.25259/SNI_941_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Sam Hajialiloo Sami, Shahrzad Rahimizadeh, Walter L. Williamson, Mahan Amirzadeh. Acute traumatic sequestrated thoracic disc herniation: A case report and review. 17-Mar-2021;12:108
How to cite this URL: Abolfazl Rahimizadeh, Sam Hajialiloo Sami, Shahrzad Rahimizadeh, Walter L. Williamson, Mahan Amirzadeh. Acute traumatic sequestrated thoracic disc herniation: A case report and review. 17-Mar-2021;12:108. Available from: https://surgicalneurologyint.com/surgicalint-articles/10644/
Date of Submission
24-Dec-2020
Date of Acceptance
05-Feb-2021
Date of Web Publication
17-Mar-2021
Abstract
Background: Pure sequestrated thoracic disc herniations secondary to a traumatic event are rare.
Case Description: Elderly male presented with the sudden onset of severe paraparesis following a fall. The MR showed a left-sided extruded disc at the T10-T11. The patient underwent a thoracic interlaminar laminectomy, removal of one large, and several smaller sequestrated disc fragments utilizing a transfacet corridor requiring placement of an interbody Peek cage, and bilateral T10 and T11 pedicle screw instrumentation. At 6 postoperative months, he sustained a good recovery.
Conclusion: Acute thoracic disc herniations without attendant fracture/dislocation are rare. When they result in major neurological deficits, timely surgical excision is warranted.
Keywords: Outcome, Thoracic disc, Thoracic spine, Transfacet pedicle sparing route, Transthoracic approach, Traumatic thoracic disc herniation
INTRODUCTION
Acute traumatic thoracic disc herniations without serious fracture/dislocation are rare.
Here, we present a 75-year-old male whose acute paraparesis was attributed to a traumatic MR/ CT documented sequestrated disc at the T10-T11 level. Following surgical excision, the patient sustained a remarkable recovery.
CASE REPORT
A 75-year-old male presented with severe paraparesis after a fall. He exhibited bilateral lower extremity weakness (strength score of 2/5) with diffuse hyperreflexia, bilateral Babinski signs, and a questionable T12 sensory level.
Imaging
The T2-weighted axial MR images showed an isointense left-sided large anterolateral thoracic disc herniation at the T10-T11 level with superior migration resulting in an image equivalent to a “complete block” herniation [
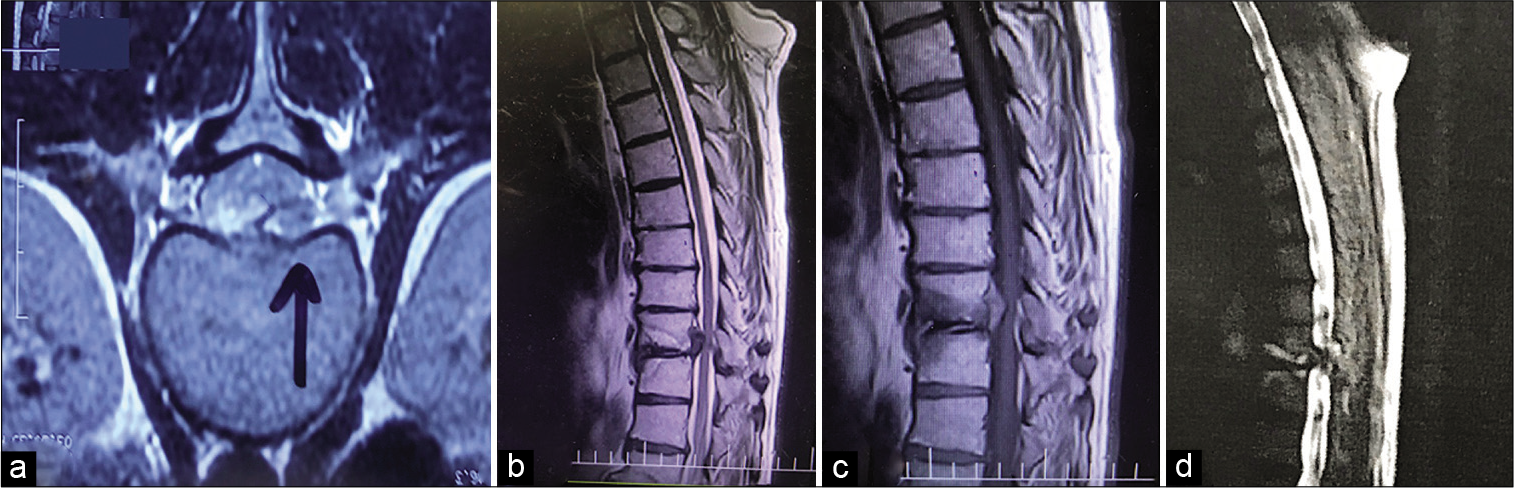
Figure 1:
Thoracic spine MRI, (a) axial T2-weighted image show left-sided isointense mass compatible with a sequestrated disc (black arrow), (b and c) sagittal T1- and T2-weighted MRI demonstrated the disc fragment migrated up, note the edema of the corresponding end plated. (d) MR myelogram showing complete block at the affected level and hyperintense endplates edema.
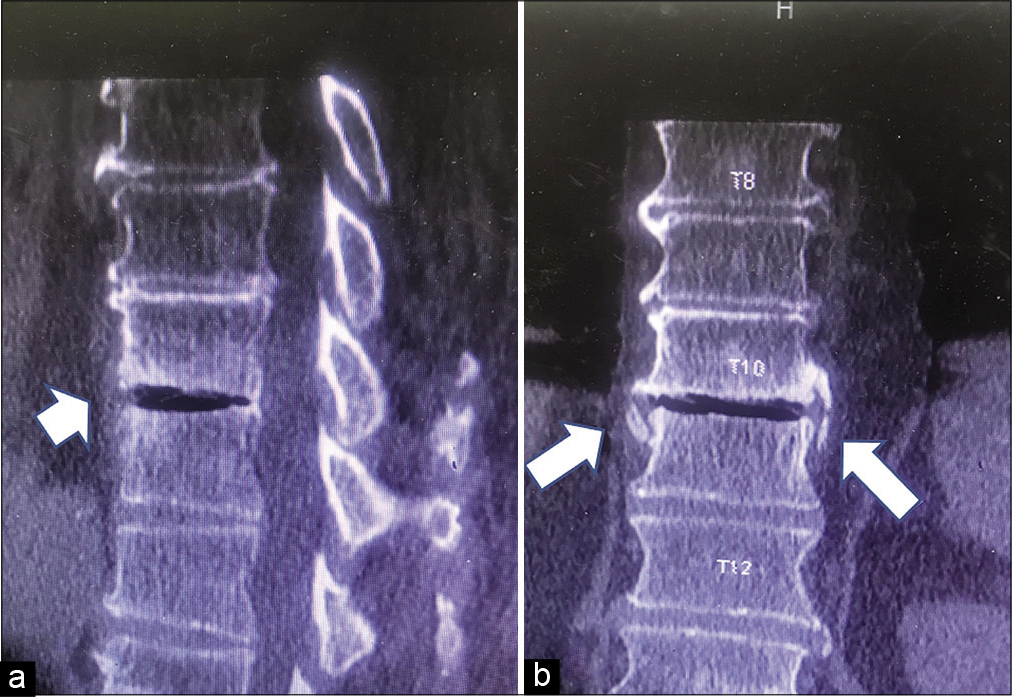
Figure 2:
Thoracic spine reconstructed C.T. scan, (a) in sagittal view, the intervertebral disc space is hypodense indicating release of nitrogen gas through the porous holes of the corresponding end plates into the disc space subsequent to expulsion of the nucleus and occurrence of negative pressure, designated as vacuum phenomenon (white arrow head) (b). Coronal images show breakage of the lateral syndesmophytes in the absence of vertebral body fracture which is indicative of acute traumatic event.
Surgery
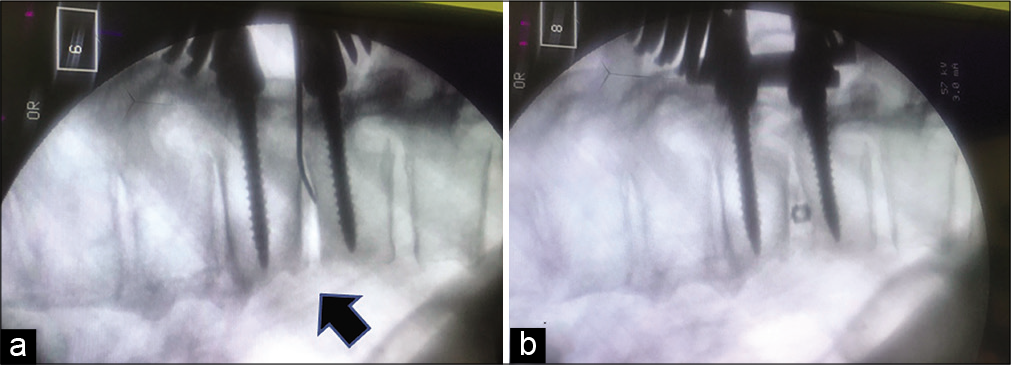
The surgery included; a thoracic interlaminar laminectomy, removal of one large and several smaller sequestrated disc fragments (i.e., removed through a transfacet corridor), and placement of an interbody banana-shaped Peek cage (i.e., bilaterally at the T10 and T11 level) with T10 and T11 bilateral pedicle screws [
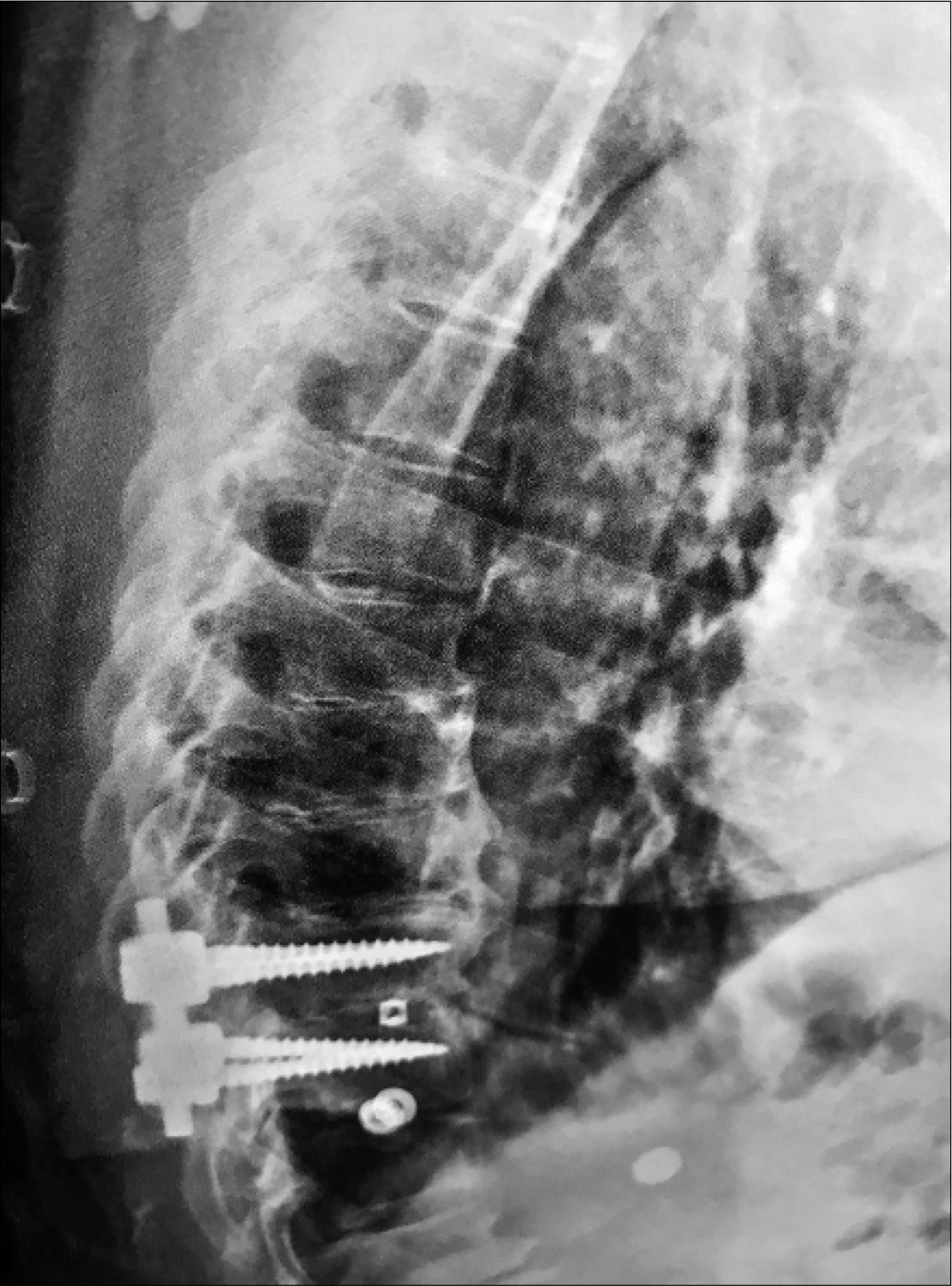
Six weeks postoperatively, could the patient could barely ambulate with a walker. However, the thoracic plain radiographs showed that the fusion construct was intact [

DISCUSSION
Thoracic disc herniations account for roughly 0.25–0.75% of all spinal disc ruptures.[
Rarely, a traumatic sequestrated soft disc herniations can occur in the absence of a vertebral fracture or dislocation.[
CONCLUSION
MR imaging is the study of choice to identify traumatic thoracic disc herniations. Notably, patients with severe preoperative deficits may not exhibit substantial postoperative recovery despite timely surgical intervention utilizing a transfacet pedicle-sparing approach.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Basile L, Brunasso L, Gerardi RM, Maugeri R, Iacopino DG, Gulì C. Traumatic lumbar disc extrusion mimicking spinal epidural hematoma: Case report and literature review. Surg Neurol Int. 2020. 11: 348
2. Carr DA, Volkov AA, Rhoiney DL, Setty P, Barrett RJ, Claybrooks R. Management of thoracic disc herniations via posterior unilateral modified transfacet pedicle-sparing decompression with segmental instrumentation and interbody fusion. Global Spine J. 2017. 7: 506-13
3. Fuentes S, Metellus P, Dufour H, Grisoli F. Traumatic thoracic disc herniation. Case illustration. J Neurosurg. 2001. 95: 276
4. Kil JS, Park JT. Posterior epidural herniation of a lumbar disk fragment at L2-3 that mimicked an epidural hematoma. Korean J Spine. 2017. 14: 115-7
5. Ogrenci A, Koban O, Yilmaz M, Yaman O, Dalbayrak S. Traumatic sequestrated thoracic disc herniation; a case report. Turk Neurosurg. 2019. 29: 954-6
6. Pringle RG, Hayes KC, Askes HK, Kakulas BA. Retropulsion of intervertebral discs associated with traumatic hyperextension of the cervical spine and absence of vertebral fracture: An uncommon mechanism of spinal cord injury. Spinal Cord. 2003. 41: 254-5
7. Rahimizadeh A, Rahimizadeh A, Saghri M, Hajimirzabeigi A, Yazdi T. Spontaneous resolution of a big thoracic disc herniation. Report of a case and review of the literature. World Spinal Column J. 2015. 6: 133-8
8. Rahimizadeh A, Zohrevand A, Kabir N. T1-T2 disc herniation: Report of four cases and review of the literature. Surg Neurol Int. 2019. 10: 56
9. Rahimizadeh A. Thoracic disc herniation: 20 years experience in 82 cases. Glob Spine J. 2016. 6: 36-7
10. Song KJ, Lee KB, Kim DY, Lee SY. A traumatic disc herniation mimicking an epidural hematoma in a young adult; a case report. Neurosurgy Q. 2012. 22: 81-3

