

- Department of Spine Service, Indian Spinal Injuries Center, New Delhi, India,
- Department of Orthopaedics, North Eastern Medical University, Rootstown, Ohio, United States,
- Department of Radiology, Indian Spinal Injuries Center, New Delhi, India.
Correspondence Address:
Kalyan Kumar Varma Kalidindi
Department of Spine Service, Indian Spinal Injuries Center, New Delhi, India,
DOI:10.25259/SNI_875_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kuldeep Bansal1, Kalyan Kumar Varma Kalidindi1, Anuj Gupta1, Venkata Nishant Surapaneni2, Rajesh Kapur3, Harvinder Singh Chhabra1. An extremely rare presentation of AV fistula: Massive destruction of multiple vertebral bodies with paraparesis. 30-Mar-2021;12:123
How to cite this URL: Kuldeep Bansal1, Kalyan Kumar Varma Kalidindi1, Anuj Gupta1, Venkata Nishant Surapaneni2, Rajesh Kapur3, Harvinder Singh Chhabra1. An extremely rare presentation of AV fistula: Massive destruction of multiple vertebral bodies with paraparesis. 30-Mar-2021;12:123. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10688
Date of Submission
04-Dec-2020
Date of Acceptance
21-Jan-2021
Date of Web Publication
30-Mar-2021
Abstract
Background: Spinal ventral epidural arteriovenous fistulas (EDAVFs) are rare and underdiagnosed entities and usually present with benign symptoms such as radiculopathy. To the best of our knowledge, EDAVFs presenting with massive vertebral body destruction have not been reported in the literature.
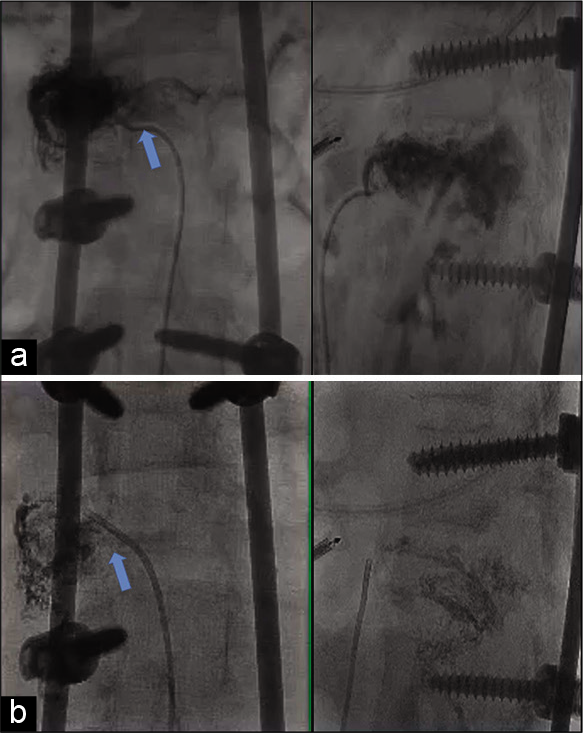
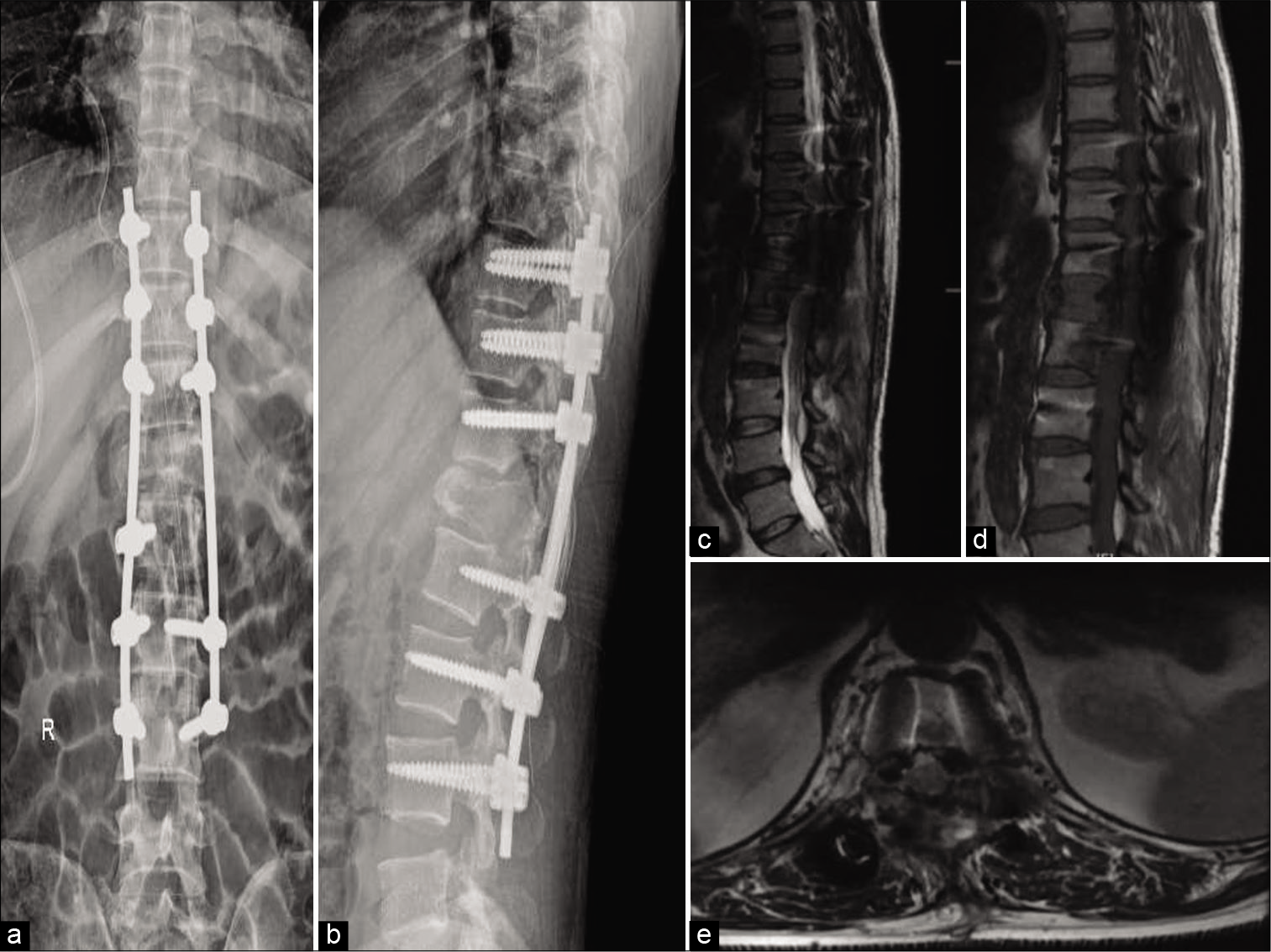
Case Description: A young male presented with mid back pain for 1 year and weakness of both lower limbs for 3 months. He was clinicoradiologically diagnosed with spinal tuberculosis and started on antitubercular treatment elsewhere. Radiological investigations suggested destruction and collapse of T12 and L1 vertebrae. Prominent flow voids were seen in T9-L2 epidural space, likely prominent epidural vessels. The primary differential diagnoses were spinal tuberculosis and neoplastic etiologies. T9 to L3 surgical stabilization and anterior decompression by pediculectomy of left T12 and L was done. The surgeon encountered massive bleeding at the time of anterior decompression and a vascular etiology was suspected. Biopsy revealed negative results for infection or malignancy. DSA revealed ventral EDAVFs, and hence, transcatheter embolization was performed. He had excellent outcome on assessment at 21 months postoperative follow-up.
Conclusion: Spinal epidural AVFs can rarely present with gross vertebral body destruction and paraparesis. Preoperative radiological assessment with suspicion of spinal epidural AVFs can help to avoid intraoperative difficulties and complications. Timely, management of spinal epidural AVFs can result in excellent outcomes
Keywords: AV fistula, Extradural arteriovenous fistula, Paraparesis, Rare, Vertebral body
INTRODUCTION
Spinal ventral epidural arteriovenous fistulas (EDAVFs) are rare and underdiagnosed entities and usually present with benign symptoms such as radiculopathy.[
CASE PRESENTATION
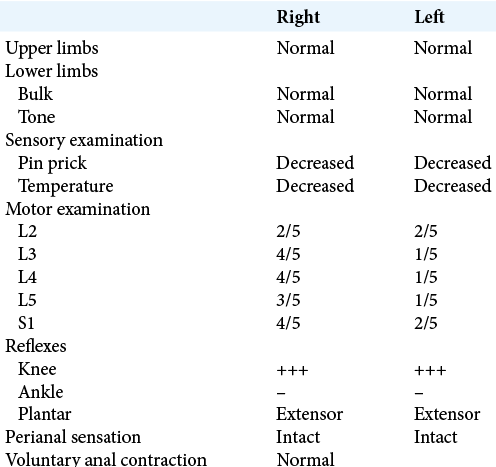
A 38-year-old male patient presented to the outpatient department with a history of mid-back pain for 1 year and progressive weakness in both lower limbs for 3 months. The pain in the mid-back was insidious in onset, progressive in nature, dull-aching in character, initially aggravated by walking and movements of the trunk but had pain even at rest at the time of presentation. Back pain was also associated with a history of difficulty in walking and pain in both lower limbs for the past 3 months. The patient walked with help of walking aid. There was no history of trauma or constitutional symptoms such as fever, weight and loss or loss of appetite. He consulted elsewhere, where he was clinicoradiologically diagnosed with spinal tuberculosis and was started on the anti-tubercular therapy, but there was no relief in his symptoms even after 2 months of taking anti-tubercular therapy. The family and personal history were not significant. On examination, there was deep tenderness over the thoracolumbar junction. There was no local warmth/swelling over the back. The neurological examination suggested paraparesis [
Thoracolumbar radiographs (AP/Lateral) and CT scan suggested huge lytic lesions with complete destruction of T12 and L1 vertebral body as well as pedicles and posterior elements and complete collapse of body of T12 with partial collapse of the body of L1 [
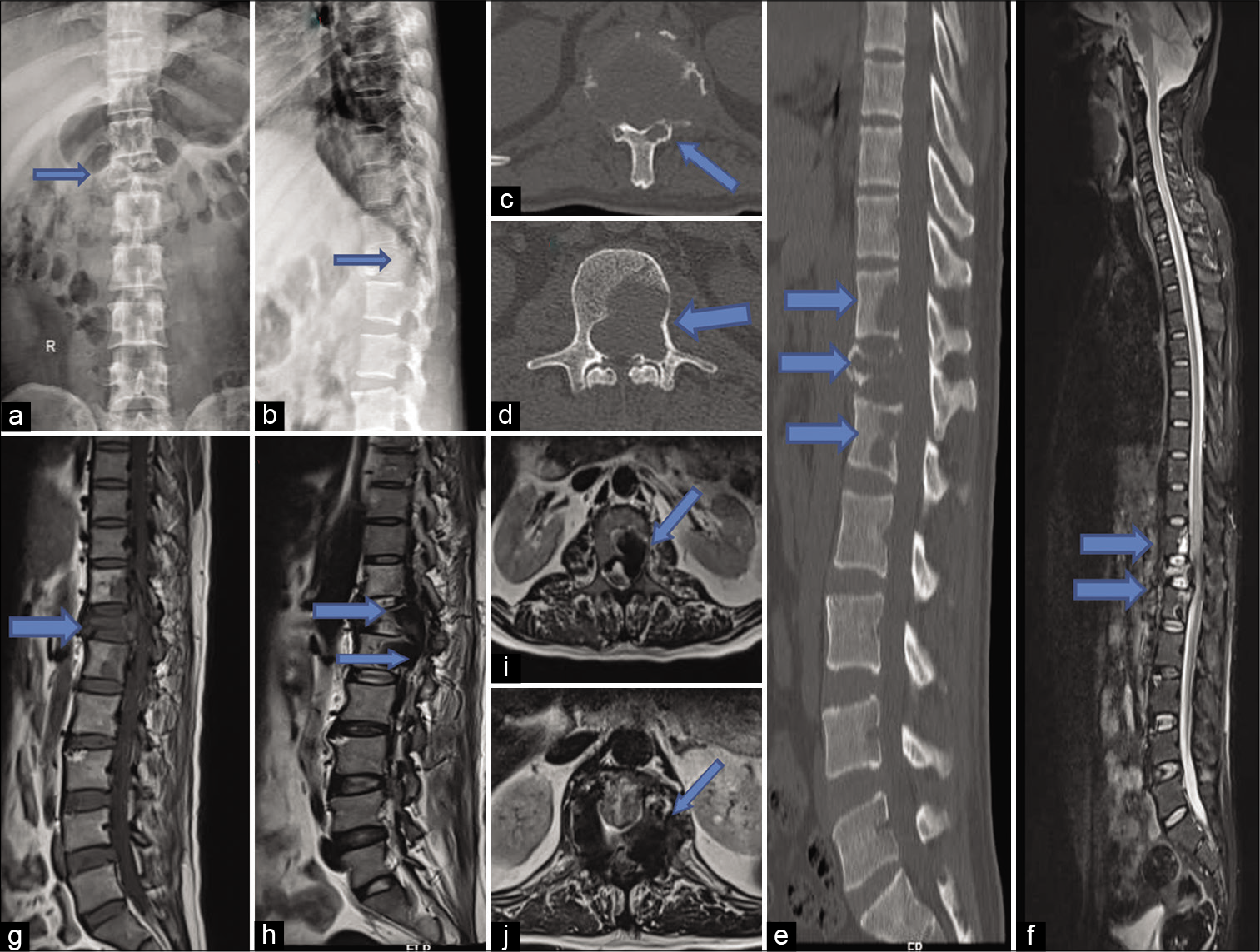
Figure 1:
Preoperative radiographs (a and b) and CT (c-e) scan showing destruction of T12 and L1 vertebral bodies with complete collapse of T12 and partial collapse of L1 body. Preoperative MRI showing signal intensity changes in T11, T12, and L1 vertebrae with hyperintense signal on T2 imaging (f-j) and hypointense signal on T1 imaging (g). Blue arrows depict the pathology.
DISCUSSION
Although there have been reports of vascular abnormalities such as hemangiomas causing vertebral body destruction, spinal ventral EDAVFs causing huge destruction of multiple vertebral bodies are extremely rare.[
CONCLUSION
Spinal epidural AVFs can rarely present with gross vertebral body destruction and paraparesis Preoperative radiological assessment with suspicion of spinal epidural AVFs can help to avoid intraoperative difficulties and complications Timely, management of Spinal Epidural AVFs can result in excellent outcomes.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Asumu TO, Williamson B, Hughes DG. Symptomatic spinal hemangiomas in association with cutaneous hemangiomas. A case report. Spine (Phila Pa 1976). 1996. 21: 1082-4
2. Doppman JL, Wirth FP, di Chiro G, Ommaya AK. Value of cutaneous angiomas in the arteriographic localization of spinal-cord arteriovenous malformations. N Engl J Med. 1969. 281: 1440-4
3. Krings T, Geibprasert S. Spinal dural arteriovenous fistulas. AJNR Am J Neuroradiol. 2009. 30: 639-48
4. Nagata N, Koshino T, Saito T, Ishida T, Sakano H. Multiple gigantic arteriovenous malformations with destruction of lumbar vertebral bodies. A case report. Spine (Phila Pa 1976). 1999. 24: 1377-80

