

- Department of Neurosurgery, Iwate Prefectural Chubu Hospital, Kitakami, Iwate, Japan
Correspondence Address:
Hiroshi Kashimura
Department of Neurosurgery, Iwate Prefectural Chubu Hospital, Kitakami, Iwate, Japan
DOI:10.4103/2152-7806.166178
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Aso K, Kashimura H, Takeda M, Chida K. An unusual variant of the common trunk of the fronto-orbital and frontopolar arteries associated with a ruptured aneurysm of the A1 segment of the anterior cerebral artery. Surg Neurol Int 28-Sep-2015;6:
How to cite this URL: Aso K, Kashimura H, Takeda M, Chida K. An unusual variant of the common trunk of the fronto-orbital and frontopolar arteries associated with a ruptured aneurysm of the A1 segment of the anterior cerebral artery. Surg Neurol Int 28-Sep-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/an-unusual-variant-of-the-common-trunk-of-the-fronto%e2%80%91orbital-and/
Abstract
Background:The common trunk of the fronto-orbital artery (FOA) and frontopolar artery (FPA) arising from the A1 segment of the anterior cerebral artery (ACA) associated with a ruptured aneurysm (AN), is rare.
Case Description:The patient was a 52-year-old man who suffered from subarachnoid hemorrhage. Three-dimensional computed tomography angiography revealed an elongated and tortuous left A1 segment of the ACA and a saccular AN arising from the left A1 segment of the ACA at the origin of the cortical branch, defining its location just on the midline and behind the anterior communicating artery. This vessel had two branches. One branch ran along the inferior surface of the ipsilateral frontal lobe, and the other branch ran anteriorly and medially along the surface of the left hemisphere toward the frontal pole. The anomalous artery was interpreted as a common trunk of the FOA and FPA. Bifrontal craniotomy was performed. The anomalous artery arose from the A1 segment of the ACA at the origin of the AN, and the recurrent artery of Heubner branched off the anomalous artery. The AN was successfully obliterated, clipping with a bayonet-shaped Yasargil titanium clip. Complete AN occlusion and patency of both the A1 and the common trunk of the FOA and FPA, were confirmed intraoperatively by indocyanine green angiography.
Conclusions:Recognizing this variant preoperatively, could be helpful in preventing the complications of surgery.
Keywords: Aneurysm, anterior cerebral artery, common trunk, fronto-orbital artery, frontopolar artery
INTRODUCTION
Aneurysms (ANs) arising from the A1 segment of the anterior cerebral artery (ACA) are quite rare and are considered to be unique because they are usually connected with other vascular anomalies such as a fenestration of the A1 segment, an infra-optic course of the A1 segment, or an anomalous cortical branch arising from the A1 segment such as an accessory middle cerebral artery, a persistent primitive olfactory artery, or a callosomarginal artery.[
CASE REPORT
A 52-year-old man presented with a severe headache and subsequent loss of consciousness was admitted to our hospital. No focal neurological abnormality was noted. Initial computed tomography (CT) showed the typical findings of subarachnoid hemorrhage in the basal cistern. Three-dimensional CT angiography revealed an elongated and tortuous left A1 segment of the ACA and a saccular AN arising from the left A1 segment of the ACA at the origin of the cortical branch, defining its location just on the midline and behind the anterior communicating artery (ACoA) [
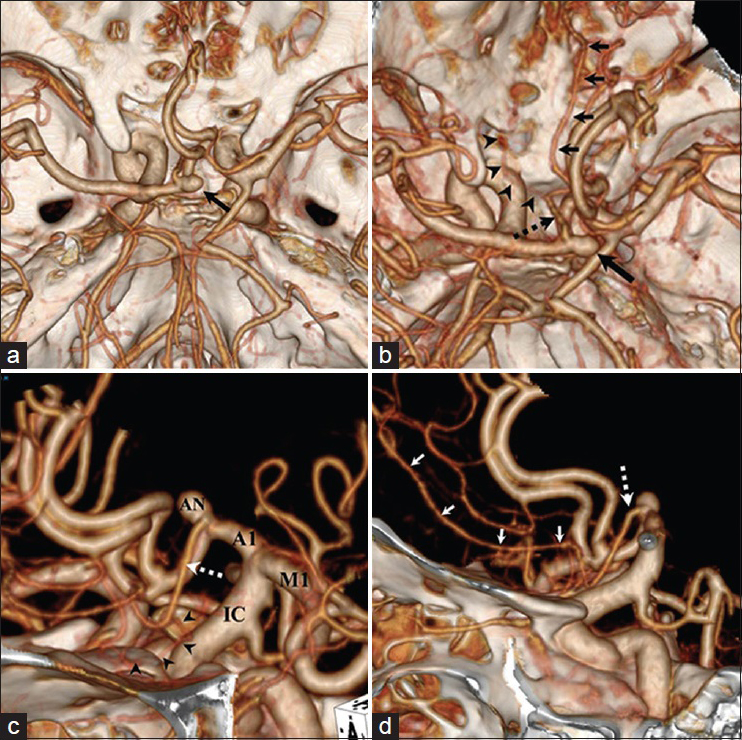
Figure 1
Three-dimensional computed tomography angiogram, superoinferior view (a and b) showing a saccular aneurysm (black arrow) arising from the left A1 segment of the anterior cerebral artery at the origin of the common trunk (black dotted arrow) of the fronto-orbital artery (black arrowheads) and frontopolar artery (black arrows). An aneurysm is located just on the midline and behind the anterior communicating artery. Three-dimensional computed tomography angiogram, oblique view (c), showing an elongated and tortuous left A1 segment of the anterior cerebral artery. The common trunk (white dotted arrow) shares a fronto-orbital artery and runs along the inferior surface of the ipsilateral frontal lobe (black arrowheads). Three-dimensional computed tomography angiogram, lateral view (d), showing an aneurysm located in the highest place on the vessel. The common trunk (white dotted arrow) shares a frontopolar artery, which runs anteriorly and medially along the surface of the left hemisphere toward the frontal pole (white arrows). ACA: Anterior cerebral artery, AN: Aneurysm, A1: A1 segment of the anterior cerebral artery, CT: Computed tomography, IC: Internal cerebral artery, M1: M1 segment of the middle cerebral artery, FOA: Fronto-orbital artery, FPA: Frontopolor artery
Bifrontal craniotomy was performed, and the interhemispheric fissure was opened widely to expose the ACoA, the bilateral distal A2, and the A3 segment of the ACA [
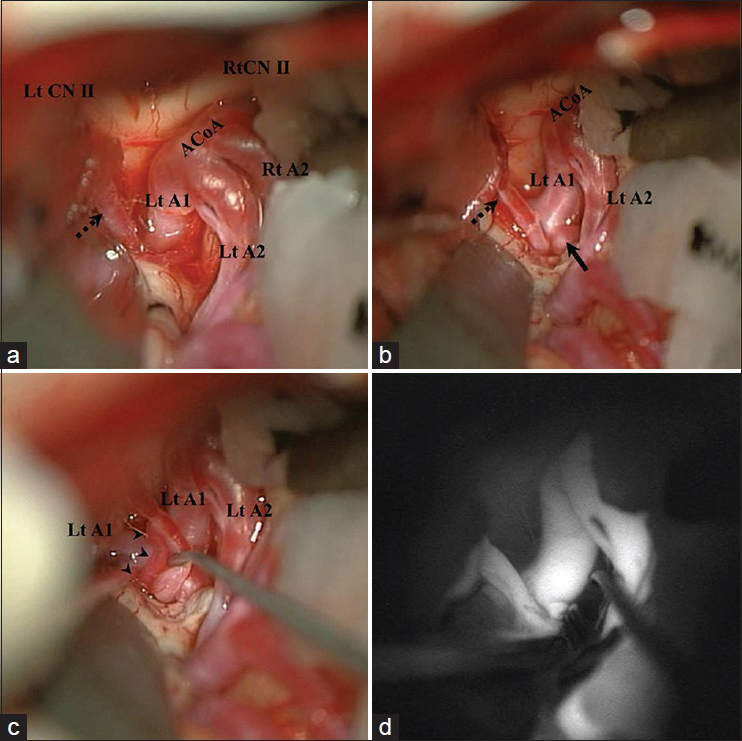
Figure 2
Intraoperative photographs showing the aneurysm (black arrow) and its relationship to the left distal A1 segment, left A2 segment of the anterior cerebral artery, anterior communicating artery, and the common trunk of the frontopolor artery and fronto-orbital artery (black dotted arrow) (a and b). A small cortical incision is made in the gyrus rectus allowing visualization of the proximal aneurysmal neck (b). The common trunk of the fronto-orbital artery and the frontopolor artery from the A1 segment of the anterior cerebral artery shares Heubner's artery (black arrowheads) (c). Intraoperative indocyanine green angiogram showing the patency of both the A1 (proximal A1 segment) (white arrow) and the common trunk of the frontopolor artery and frontopolor artery (white arrowheads) (d). ACA: Anterior cerebral artery, ACoA: Anterior communicating artery, CN: Cranial nerve, FOA: Fronto-orbital artery, FPA: Frontopolor artery, Lt: Left, Rt: Right
DISCUSSION
The FOA is the first cortical branch of the ACA and normally arises from the ipsilateral pericallosal artery.[
The featured case has some interesting characteristics. First, a common trunk of the FOA and FPA arose from the A1 segment of the ACA associated with ruptured AN. Anomalous arteries originating from the A1 segment of the ACA are often associated with cerebral AN. The pathogenesis of associated ANs has not been fully clarified, and both genetic and hemodynamic factors are considered. Therefore, a careful follow-up study is necessary to monitor AN formation in cases with an arterial abnormality of the A1 segment of the ACA.
Second, the ruptured AN was located just on the midline and behind the ACA due to an elongated and tortuous left A1 segment of the ACA. In treating A1 ANs, most of the ANs are easily visualized by using a standard pterional approach. In the present case, the patient underwent microsurgical clipping via the interhemispheric approach because of its deep and high location. It is critical to preserve the patency of the A1 segment of the ACA as well as the common trunk of the FOA, FPA, and Heubner's artery. Recognizing and reporting this variant could be helpful in preventing the complications of surgery. Although injury to the common trunk itself is unlikely to result in clinical deficits, precise knowledge of the vascular anatomy, including such variants, is essential to help minimize complications. When an A1 AN is found, one should carefully scrutinize the angiograms to identify anomalies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Handa J, Nakasu Y, Matsuda M, Kyoshima K. Aneurysms of the proximal anterior cerebral artery. Surg Neurol. 1984. 22: 486-90
2. Hino A, Fujimoto M, Iwamoto Y, Oka H, Echigo T. Surgery of proximal anterior cerebral artery aneurysms. Acta Neurochir (Wien). 2002. 144: 1291-6
3. Hong SK. Ruptured proximal anterior cerebral artery (A1) aneurysm located at an anomalous branching of the fronto-orbital artery – A case report. J Korean Med Sci. 1997. 12: 576-80
4. Horie N, Morikawa M, Fukuda S, Hayashi K, Suyama K, Nagata I. New variant of persistent primitive olfactory artery associated with a ruptured aneurysm. J Neurosurg. 2012. 117: 26-8
5. Huber P, Bosse G.editors. Cerebral Angiography. New York: Thieme-Stratton; 1982. p. 85-8
6. Krishnamoorthy T, Gupta AK, Bhattacharya RN, Rajesh BJ, Purkayastha S. Anomalous origin of the callosomarginal artery from the A1 segment with an associated saccular aneurysm. AJNR Am J Neuroradiol. 2006. 27: 2075-7
7. Lee ER, Eastwood JD. An unusual variant of the fronto-orbital artery. AJNR Am J Neuroradiol. 2000. 21: 939-40
8. Lee JM, Joo SP, Kim TS, Go EJ, Choi HY, Seo BR. Surgical management of anterior cerebral artery aneurysms of the proximal (A1) segment. World Neurosurg. 2010. 74: 478-82
9. Marinkovic S, Milisavljevic M, Kovacevic M. Anatomical bases for surgical approach to the initial segment of the anterior cerebral artery. Microanatomy of Heubner's artery and perforating branches of the anterior cerebral artery. Surg Radiol Anat. 1986. 8: 7-18
10. Mäurer J, Mäurer E, Perneczky A. Surgically verified variations in the A1 segment of the anterior cerebral artery. Report of two cases. J Neurosurg. 1991. 75: 950-3
11. Newton TH, Potts DG.editors. Radiology of the Skull and Brain Angiography. St. Louis, MO: Mosby; 1974. p. 1414-
12. Suzuki M, Onuma T, Sakurai Y, Mizoi K, Ogawa A, Yoshimoto T. Aneurysms arising from the proximal (A1) segment of the anterior cerebral artery. A study of 38 cases. J Neurosurg. 1992. 76: 455-8
13. Wakabayashi T, Tamaki N, Yamashita H, Saya H, Suyama T, Matsumoto S. Angiographic classification of aneurysms of the horizontal segment of the anterior cerebral artery. Surg Neurol. 1985. 24: 31-4
14. Wanibuchi M, Kurokawa Y, Ishiguro M, Fujishige M, Inaba K. Characteristics of aneurysms arising from the horizontal portion of the anterior cerebral artery. Surg Neurol. 2001. 55: 148-54
15. Yasargil MG. Anterior communicating artery aneurysm. Microneurosurgery. Stuttgart: Georg Thieme Verlag; 1984. I: 113-6

