

- Department of Neurosurgery, Umberto I General Hospital, Università Politecnica delle Marche, Ancona, Italy
DOI:10.25259/SNI-22-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: M. Dobran, Davide Nasi, R. Paracino, M. Gladi, M. Della Costanza, A. Marini, S. Lattanzi, M. Iacoangeli. Analysis of risk factors and postoperative predictors for recurrent lumbar disc herniation. 26-Mar-2019;10:36
How to cite this URL: M. Dobran, Davide Nasi, R. Paracino, M. Gladi, M. Della Costanza, A. Marini, S. Lattanzi, M. Iacoangeli. Analysis of risk factors and postoperative predictors for recurrent lumbar disc herniation. 26-Mar-2019;10:36. Available from: http://surgicalneurologyint.com/surgicalint-articles/9248/
Date of Submission
13-Jan-2019
Date of Acceptance
18-Jan-2019
Date of Web Publication
26-Mar-2019
Abstract
Background: This study identified risk factors and postoperative indicators for recurrent lumbar disc herniations (rLDH) following microdiscectomy.
Methods: We retrospectively reviewed the 1-year recurrence rate for LDH in 209 consecutive patients undergoing microdiscectomy (2013–2018).
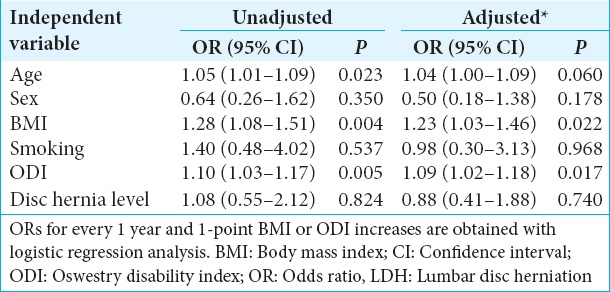
Results: Utilizing a multivariate analysis, higher body mass index (BMI) and postsurgery Oswestry disability index (ODI) were significantly associated with an increased risk of rLDH.
Conclusion: Elevated postsurgery ODI and higher BMI were significantly associated with increased risk of rLDH.
Keywords: Discectomy, lumbar disc herniation, lumbar microdiscectomy, recurrent disc herniation
INTRODUCTION
Lumbar disc herniation (LDH) is the most common reason for performing lumbar spine surgery. Today, many are managed utilizing a microdiscectomy approach. Nevertheless, these procedures correlate with a recurrence rate at 1 year that ranges from 1% to 21%.[
MATERIALS AND METHODS
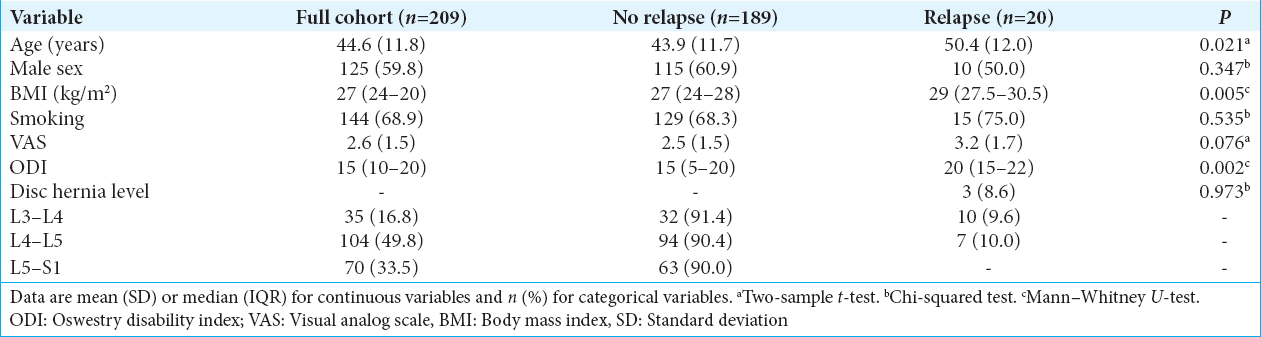
We retrospectively reviewed consecutive patients who underwent standard lumbar spinal microdiscectomy for disc herniation (LDH) (2013–2018). The follow-up evaluations were performed at 1, 6, and 12 months postoperatively. Recurrence of disc herniation was defined as disc herniation at the same level and side of the previous microdiscectomy after a 3-month postoperative pain-free period. Variables contributing to rLDH included age, sex, weight/body mass index (BMI), smoking status, postoperative (6 months) Oswestry disability index (ODI), and the level of the disc herniation. Radiological examination included magnetic resonance imaging before and after surgery.
Statistical analysis
Analyses include Student’s t-test, Mann–Whitney U-test or Chi-squared test, logistic regression, and multivariate analysis. Results were considered significant for P < 0.05 (two-sided). Data analysis was performed using STATA/IC 13.1 statistical package (StataCorp LP, Texas, USA).
RESULTS
There were 209 patients included in this study; 20 of 209 (9.6%) had rLDH at 1 postoperative year. Utilizing a multivariate analysis, older age, higher BMI, and postsurgery ODI were significantly associated with increased risk of rLDH [Tables
DISCUSSION
Microdiscectomy is a relatively straightforward procedure but is associated with a complication rate of up to 15–18%.[
CONCLUSIONS
To summarize, patients with rLDH were older and had higher BMI and postsurgery ODI score after a pain-free 3-month interval.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ambrossi GL, McGirt MJ, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL. Recurrent lumbar disc herniation after single-level lumbar discectomy: Incidence and health care cost analysis. Neurosurgery. 2009. 65: 574-8
2. Dobran M, Brancorsini D, Costanza MD, Liverotti V, Mancini F, Nasi D. Epidural scarring after lumbar disc surgery: Equivalent scarring with/without free autologous fat grafts. Surg Neurol Int. 2017. 8: 169-
3. Dobran M, Marini A, Gladi M, Nasi D, Colasanti R, Benigni R. Deep spinal infection in instrumented spinal surgery: Diagnostic factors and therapy. G Chir. 2017. 38: 124-9
4. Dobran M, Marini A, Nasi D, Gladi M, Liverotti V, Costanza MD. Risk factors of surgical site infections in instrumented spine surgery. Surg Neurol Int. 2017. 8: 212-
5. Huang W, Han Z, Liu J, Yu L, Yu X. Risk factors for recurrent lumbar disc herniation: A systematic review and meta-analysis. Medicine (Baltimore). 2016. 95: e2378-
6. Meredith DS, Huang RC, Nguyen J, Lyman S. Obesity increases the risk of recurrent herniated nucleus pulposus after lumbar microdiscectomy. Spine J. 2010. 10: 575-80

