

- Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, Illinois, USA,
- Ghaly Neurosurgical Associates, Aurora, Illinois, USA,
- Department of Anesthesiology, University of Illinois, Chicago, Illinois, USA.
Correspondence Address:
Ramsis F. Ghaly
Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, Illinois, USA,
Department of Anesthesiology, University of Illinois, Chicago, Illinois, USA.
DOI:10.25259/SNI_505_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ramsis F. Ghaly, Zinaida Perciuleac, Kenneth D. Candido, Nebojsa Nick Knezevic. Athletic pubalgia misdiagnosed as lumbar radiculopathy – A case report. 22-Nov-2019;10:224
How to cite this URL: Ramsis F. Ghaly, Zinaida Perciuleac, Kenneth D. Candido, Nebojsa Nick Knezevic. Athletic pubalgia misdiagnosed as lumbar radiculopathy – A case report. 22-Nov-2019;10:224. Available from: http://surgicalneurologyint.com/surgicalint-articles/9767/
Date of Submission
26-Oct-2019
Date of Acceptance
31-Oct-2019
Date of Web Publication
22-Nov-2019
Abstract
Background: Athletic pubalgia is a painful complex syndrome encountered by many athletes involved in sports. Multiple pathologies often coexist, and many systems can refer pain to the groin. The current case reflects the failure to distinguish pubalgia from lumbar radiculopathy.
Case Description: Originally, a 47-year-old male with left-sided inner thigh pain was diagnosed as having a L3-4-disc herniation and spinal stenosis; he underwent a L3-4 and L4-5 laminectomy/discectomy. For 2 years postoperatively, the pain persisted. Ultimately, he underwent surgical reinsertion of the adductor muscle and experienced immediate and sustained pain relief.
Conclusion: This case report highlights how pubalgia may be misdiagnosed as a lumbar disc herniation and may inadvertently lead to unnecessary lumbar surgery.
Keywords: Adductor muscle, Athletic pubalgia, Groin pain, Lumbar, Radiculopathy
INTRODUCTION
Athletic pubalgia (AP) is a tendinopathy characterized by a breakdown of the pelvic stabilizers at the confluence of the rectus abdominis insertion, adductor origin, and pelvic floor at the pubic ramus. It is a common sports-related injury (e.g., ice hockey and soccer). Acute injury is associated with extension of the trunk, and concomitant abduction of the hip. There is a significant correlation of AP with hip disease, especially femoroacetabular impingement.[
The current case reflects the failure to distinguish pubalgia from lumbar radiculopathy which led to an unnecessary lumbar laminectomy L3-4 and L4-5 and discectomy.
CASE DESCRIPTION
A 47-year-old male presented with low back, left groin pain, and lateral hip pain exacerbated by sitting and getting up from a sitting position. He was originally diagnosed with a lumbar disc herniation at the L3-4 and L4-5 levels plus spinal stenosis and underwent a L3-4 and L4-5 laminectomy/discectomy. The postoperative course was complicated by headaches secondary to intracranial hypotension from a cerebrospinal fluid leak that required repair on three separate occasions (reoperations).
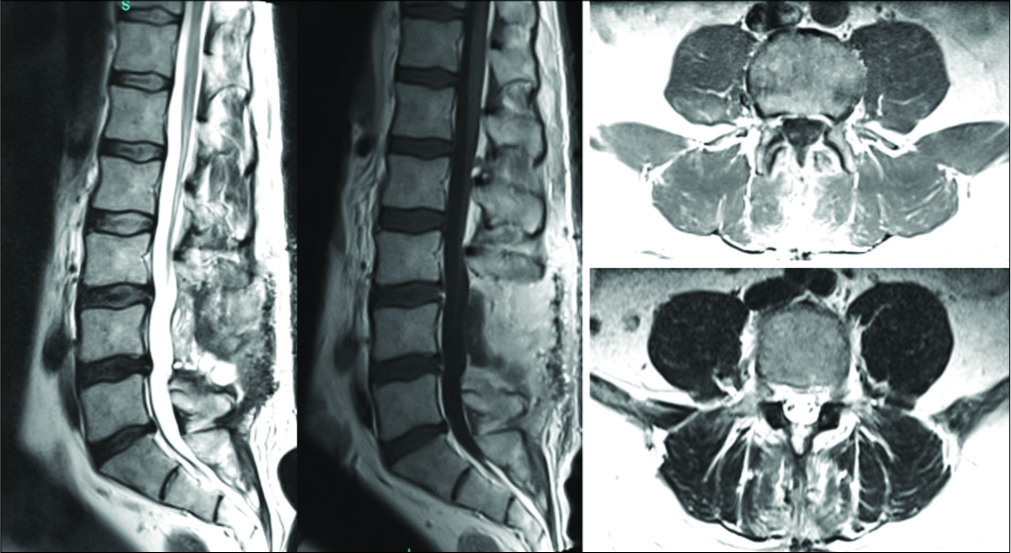
Two years of persistent groin pain and postoperative lumbar magnetic resonance (MR) positive for arachnoiditis
For 2 years following these procedures, he continued to complain of the intense left-sided inner thigh pain. The postoperative lumbar MR imaging (MRI) showed postsurgical changes without significant spinal stenosis, but adhesive arachnoiditis (e.g., clumping of the lumbar nerve roots) and a residual pseudomeningocele [
Second opinion surgeon diagnosed on MR of the hip- adductor muscle tear
A second opinion surgeon requested an MRI of the hip (e.g., first author) that revealed edema, a partial thickness tear, severe sprain of the adductor muscle of the hip, and partial thickness tear of the origin of the left common hamstring tendons – the true cause of the left thigh pain
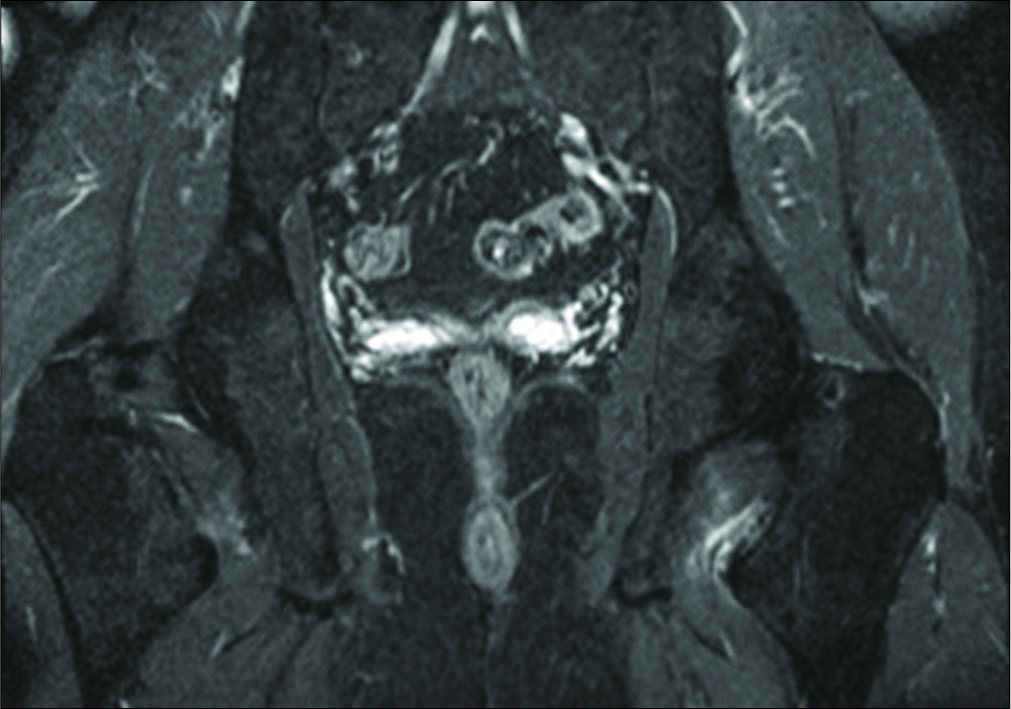
There was also some evidence of a hip labral tear, secondary to underlying femoroacetabular impingement. The physical examination was also notable for tenderness along the inner aspect of the thigh, pain on straight leg raising on the left, tenderness with hip abduction, and flexibility limited to 50–70%. Subsequently, he underwent surgical reinsertion of the adductor muscle and experienced immediate and sustained relief of his symptoms.
DISCUSSION
Definition and clinical presentation of pubalgia: a sports- related injury
AP, sometimes called “sports hernia,” occurs due to a strain or tear of the adductor muscle group. It typically presents as pain, sometimes severe and disabling along the inner aspect of the thigh and groin, and typically follows an acute injury or a repetitive eccentrically load the trunk flexors and hip adductors. Tenderness to palpation of the adductors reproduces pain in 36% of athletes around the pubic ramus; pain is variously elicited with resisted adduction and resisted sit-ups. With acute injuries, there is also associated swelling. Note, this all occurs without an inguinal hernia being present.[
Pathophysiology
The pathophysiology of pubalgia is attributed to an injury to where the rectus and adductors attach to the Pubic ramus and pelvic floor. Here, functional overuse, and microtrauma (e.g., caused by traction induced on the muscle attachments during sudden sharp changes in direction, repetitive kicking and lateral motions), result in this injury. The literature shows improvement with return to physical activities after surgery in >80% cases.
MR findings of pubalgia
MRI with gadolinium may confirm the diagnosis or differentiate between adductor strain, osteitis pubis, and a sports hernia.[
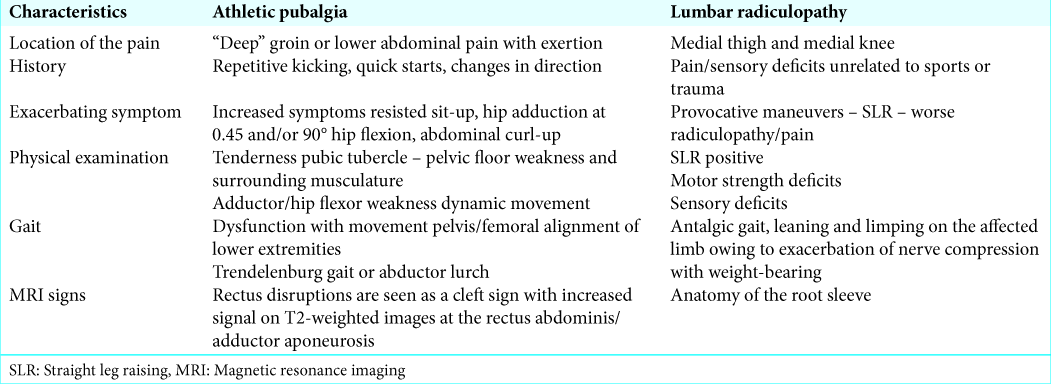
Misdiagnosis with lumbar disc disease
Patients with pubalgia may be misdiagnosed as having lumbar disc herniation, particularly as then present with groin pain and thigh pain.
CONCLUSION
AP is very common among people participating in sports. Spine surgeons should familiarize themselves with AP when evaluating patients complaining of inner thigh pain. They should learn to differentiate these patients from those with lumbar disc herniation warranting lumbar surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. DeFroda SF, Daniels AH, Deren ME. Differentiating radiculopathy from lower extremity arthropathy. Am J Med. 2016. 129: 1124.e1-7
2. Diduch DR, Brunt ML.editors. Sports Hernia and Athletic Pubalgia: Diagnosis and Treatment. United States: Springer US; 2014. p.
3. Ellsworth AA, Zoland MP, Tyler TF. Athletic pubalgia and associated rehabilitation. Int J Sports Phys Ther. 2014. 9: 774-84
4. Omar IM, Zoga AC, Kavanagh EC, Koulouris G, Bergin D, Gopez AG. Athletic pubalgia and “sports hernia”: Optimal MR imaging technique and findings. Radiographics. 2008. 28: 1415-38
5. Tibor LM, Sekiya JK. Differential diagnosis of pain around the hip joint. Arthroscopy. 2008. 24: 1407-21

