

- Department of Neurosurgery, Upstate Medical University, Syracuse, New York, United States.
DOI:10.25259/SNI_870_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Clarke I. Cady-McCrea, Michael A. Galgano. C2 quad-screws facilitate 4-rod fixation across the cervico-thoracic junction. 03-Feb-2021;12:40
How to cite this URL: Clarke I. Cady-McCrea, Michael A. Galgano. C2 quad-screws facilitate 4-rod fixation across the cervico-thoracic junction. 03-Feb-2021;12:40. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10560
Date of Submission
03-Dec-2020
Date of Acceptance
04-Jan-2021
Date of Web Publication
03-Feb-2021
Abstract
Background: Cervical spine deformity is a potentially devitalizing problem. Contemporary techniques for repair and reconstruction include fusion using rods of tapered diameter alone, or quadruple-rod constructs in which primary rods are joined to floating accessory rods by connectors. Here, we present how we utilized a quadruple-rod construct to perform five C2 to thoracic spine fusions.
Methods: Our hospital electronic medical record revealed five patients who underwent the four rod C2-thoracic spine fixation. Patients ranged in age from 14-years-old to 78-years-old. The mean operative time was 715.8 min (range 549–987 min), and average estimated blood loss was 878 cc (range 40–1800 cc).
Results: None of the five patients sustained any intraoperative complications, and none demonstrated progressive kyphotic deformity over the average follow-up interval of 8 months.
Conclusion: We successfully treated five patients with degenerative or oncologic cervical pathology requiring fixation across the cervicothoracic junction utilizing a 4-rod C2-cervicothoracic fusion technique.
Keywords: Cervical spine, Cervico-thoracic junction, Posterior instrumentation, Spinal deformity, Spinal tumor
INTRODUCTION
Numerous etiologies contribute to cervical spine deformity.[
Here, we present how we successfully utilized a quadruple-rod construct across the CTJ, from C2 to the thoracic spine, in five patients [
ILLUSTRATIVE CASES
Case 1
A 78-year-old female presented with neck pain and a chin-on-chest deformity following a prior C3–C6 laminoplasty [
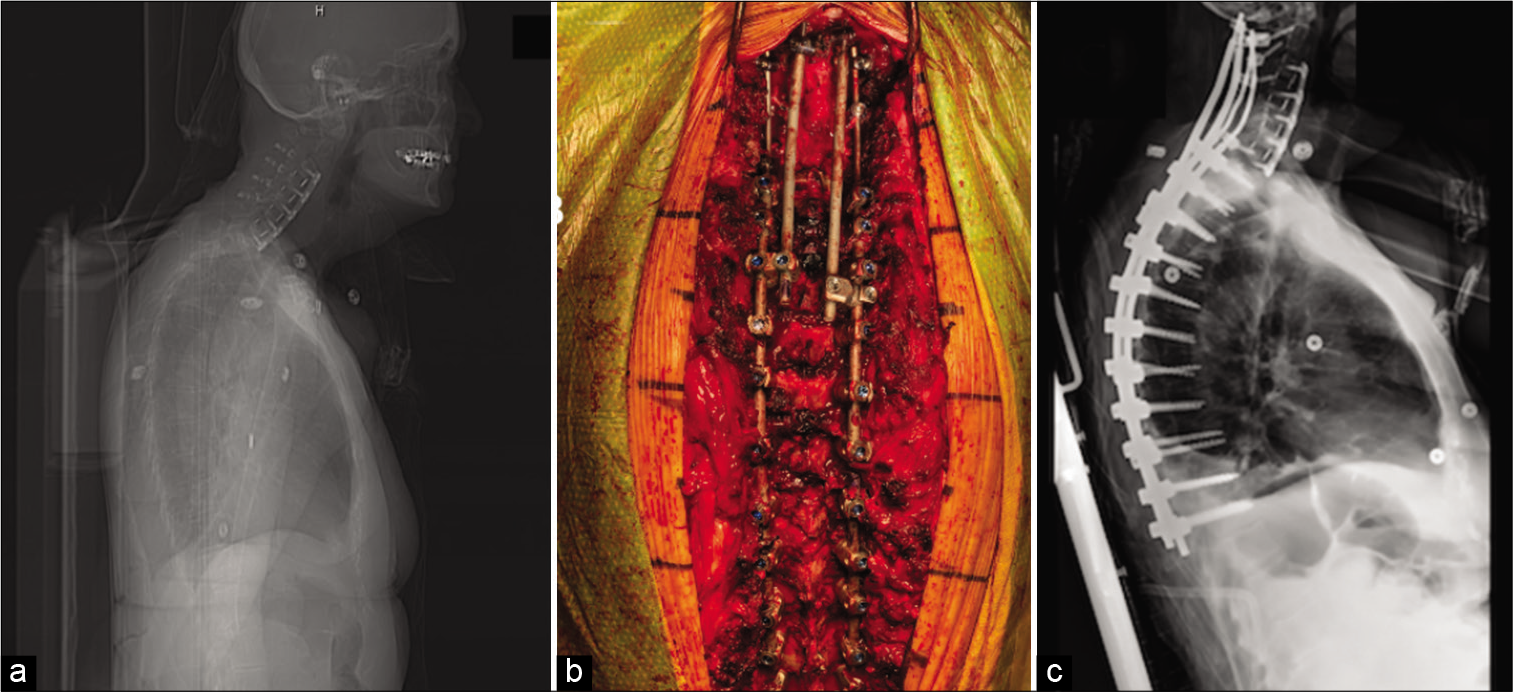
Figure 1:
Illustrative case #1. Preoperative lateral X-ray demonstrating severe cervicothoracic junction deformity (a). Posterior instrumentation demonstrating intralaminar fixation of supplementary rods (b). Postoperative lateral X-ray of instrumentation extending across the cervico-thoracic spine (c).
A C3–C6 laminectomy and Ponte osteotomies were then performed from T6 to T7 and continued rostrally to C7– T1. Rods were cut to span C2–T11 fixed with set caps. A side connector was placed just distal to the right T3 screw. We compressed all levels at which we performed a Ponte osteotomy. A second set of rods were used to connect the C2 laminar screws to the left dual-headed screw, and right lateral connector at T3 [
Case 2
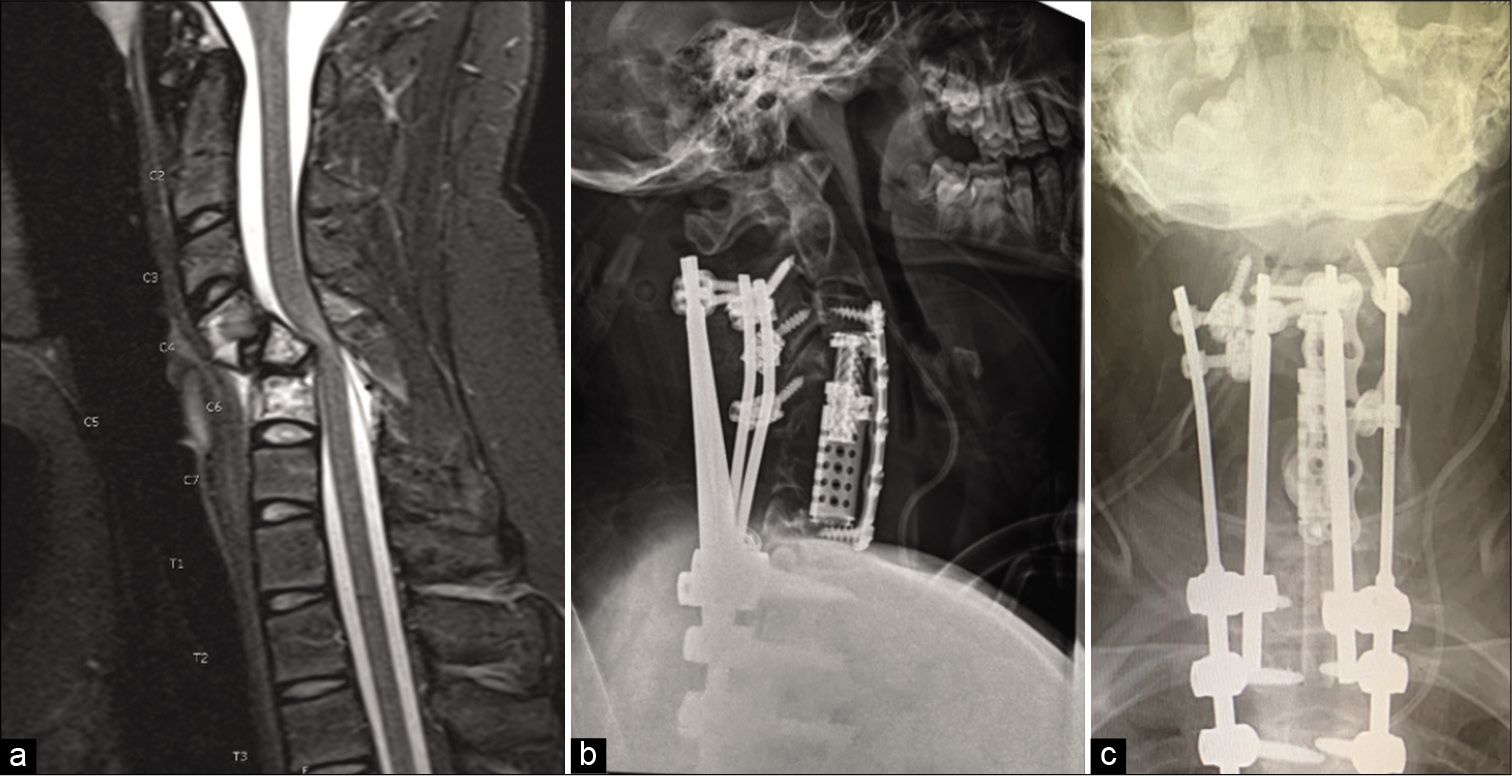
A 14-year-old who presented with quadriparesis underwent a C4–C6 anterior corpectomy using an expandable cage with plate placement from C3 to C7 for tumor.
The patient was then turned prone, bilateral pars and translaminar screws were placed at C2 [
RESULTS
Decompressions
Two patients required cervical corpectomies, one required a pedicle subtraction osteotomy, one required a thoracic Ponte osteotomy, and three required decompressive laminectomies.
Fusions
Five patients were treated with a 4-screw anchoring technique at C2 to facilitate quad-rod posterior fusion across the CTJ. Four patients were treated for postoperative cervicothoracic (CT) kyphosis and impaired horizontal gaze, while the fifth had a pathologic fracture and cervical cord injury at C5 due to an aggressive intraosseous hemangioma.
Outcomes
No patient sustained any significant intraoperative complications, and none demonstrated progressive kyphosis over 8 months postoperative months (range 6–10 months).
DISCUSSION
Numerous etiologies contribute to cervical deformity.[
Here, we presented 5 cases utilizing a 4-rod construct to across the CTJ to address different destabilizing cervico-thoracic pathologies. Proximal intralaminar screws allowed for safer placement of additional screw-rod instrumentation at C2 joined to the thoracic spine. The absence of progressive deformity or hardware failure in these five individuals affirms that this construct compares favorably to rates of distal junctional kyphosis as high as 24% and single-rod posterior cervical hardware failure rates of approximately 4%.[
CONCLUSION
We successfully treated five patients with cervical deformities warranting posterior fusion constructs utilizing a 4-rod technique for procedures crossing the CTJ.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ames CP, Smith JS, Eastlack R, Blaskiewicz DJ, Shaffrey CI, Schwab F. Reliability assessment of a novel cervical spine deformity classification system. J Neurosurg Spine. 2015. 23: 673-83
2. Goyal A, Akhras A, Wahood W, Alvi MA, Nassr A, Bydon M. Should multilevel posterior cervical fusions involving C7 cross the cervicothoracic junction? A systematic review and meta-analysis. World Neurosurg. 2019. 127: 588-95.e5
3. Jager ZS, İnceoğlu S, Palmer D, Akpolat YT, Cheng WK. Preventing instrumentation failure in three-column spinal osteotomy: Biomechanical analysis of rod configuration. Spine Deform. 2016. 4: 3-9
4. Merrill RK, Kim JS, Leven DM, Kim JH, Cho SK. Multi-rod constructs can prevent rod breakage and pseudarthrosis at the lumbosacral junction in adult spinal deformity. Global Spine J. 2017. 7: 514-20
5. Okamoto T, Neo M, Fujibayashi S, Ito H, Takemoto M, Nakamura T. Mechanical implant failure in posterior cervical spine fusion. Eur Spine J. 2012. 21: 328-34
6. Protopsaltis TS, Ramachandran S, Hamilton DK, Sciubba D, Passias PG, Lafage V. Analysis of successful versus failed radiographic outcomes after cervical deformity surgery. Spine (Phila Pa 1976). 2018. 43: E773-81
7. Ramieri A, Domenicucci M, Ciappetta P, Cellocco P, Raco A, Costanzo G. Spine surgery in neurological lesions of the cervicothoracic junction: Multicentric experience on 33 consecutive cases. Eur Spine J. 2011. 20: S13-9
8. Shen FH, Qureshi R, Tyger R, Lehman R, Singla A, Shimer A. Use of the “dual construct” for the management of complex spinal reconstructions. Spine J. 2018. 18: 482-90
9. Zhu ZZ, Chen X, Qiu Q, Chen ZH, Li S, Xu L. Adding satellite rods to standard two-rod construct with the use of duet screws: An effective technique to improve surgical outcomes and preventing proximal junctional kyphosis in posterior-only correction of scheuermann kyphosis. Spine (Phila Pa 1976). 2018. 43: E758-65

