

- Department of Neurosurgery, Centro Hospitalar Universitário do Algarve, Faro, Portugal.
Correspondence Address:
Pedro Gonçalo Abreu, Department of Neurosurgery, Centro Hospitalar Universitário do Algarve, Faro, Portugal.
DOI:10.25259/SNI_10_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Pedro Gonçalo Abreu, Clara Romero, Jose Artur Bastos Lourenço, Lia Pappamikail, Miguel Brito, Pedro Teles, Joaquim Correia. Case report: Challenging post-traumatic pseudoarthrosis of C2 odontoid fracture and extreme C1-C2 subluxation. 08-Apr-2022;13:137
How to cite this URL: Pedro Gonçalo Abreu, Clara Romero, Jose Artur Bastos Lourenço, Lia Pappamikail, Miguel Brito, Pedro Teles, Joaquim Correia. Case report: Challenging post-traumatic pseudoarthrosis of C2 odontoid fracture and extreme C1-C2 subluxation. 08-Apr-2022;13:137. Available from: https://surgicalneurologyint.com/surgicalint-articles/11512/
Date of Submission
02-Jan-2022
Date of Acceptance
24-Mar-2022
Date of Web Publication
08-Apr-2022
Abstract
Background: Type II C2 odontoid fractures are common traumatic cervical spine lesions and have the highest risk of non-union without fusion. Pseudoarthrosis may lead to extreme anatomic deformation, and poor clinical outcomes. A 50-year-old male, following a traumatic C2 dens fracture treated when the patient was 44 years of age, newly presented at age 50 with pseudoarthrosis and severe C1-C2 subluxation that required a secondary fusion using a three-dimensional (3D) printed model for appropriate surgical planning.
Case Description: A 44-year-old male underwent a C1 posterior arch osteotomy to treat cervical myelopathy after a type 2 odontoid fracture. Now at age 50, he newly presented with recurrent myelopathy, and marked cord compression due to a C2 odontoid-dens pseudoarthrosis, and extreme C1 subluxation over C2. A 3D model of the patients’ cervical-spine anatomy was created for surgical planning and led to an anterior C1-C2 freeing of the pseudoarthrosis, followed by a posterior C0-C1 decompression, deformity reduction, C0, C2 laminar, and C3/4 trans-articular arthrodesis. Six months postoperatively, the patient improved from a pre-operative mJOA score of 5 to a postoperative mJOA score of 14.
Conclusion: A 3D model was successfully utilized to plan a secondary 360° fusion for a pseudoarthrosis diagnosed 6 years after an original C-C2type II odontoid fusion in a now 50-year-old male.
Keywords: Arthrodesis, Odontoid process, Printing three-dimensional, Pseudoarthrosis
INTRODUCTION
C2 odontoid fractures account for 9–20% of all cervical spine fractures.[
CASE DESCRIPTION
At age 44, the patient originally presented with myelopathy attributed to a traumatic type II odontoid fracture. Following a C1 posterior arch osteotomy, the fracture appeared fused. However, 6 years later, at age 50, he newly presented with a markedly progressive quadriparesis, and a mJOA score of 5 due to a rotatory C1-C2 pseudoarthrosis.
MR/CT studies
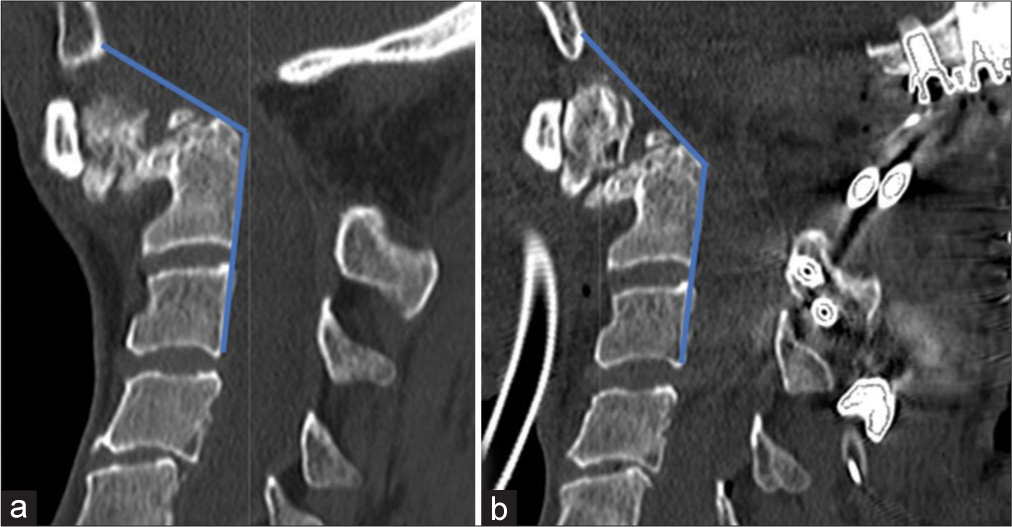
Both MR and CT studies confirmed the continued presence of a type II odontoid fracture with extreme anterior-inferior/rotatory subluxation, and pseudoarthrosis of C0/C1 over the C2 vertebral body, with the residual C1 posterior arch contributing to spinal cord compression. Myelomalacia was also seen on the MR, while the CT documented partial bony bridging between the C1-C2 levels (i.e., especially between the articular facets of the C1 and C2 bodies) [

Figure 1:
(a-f) Preoperative C-Spine CT scan, bone window. (a) Medial sagittal view, (b) Left paramedian sagittal view, (c) Right paramedian sagittal view, (d) axial odontoid base view, (e) coronal odontoid view, (f) coronal C1-C2 facets view, (g) preoperative cervical MRI T2WI sagittal view, (h) pre-operative cervical MRI T1WI sagittal view.
Surgery
A 3D CT model of the patients’ occipito-cervical junction pathology was obtained to facilitate surgical planning [
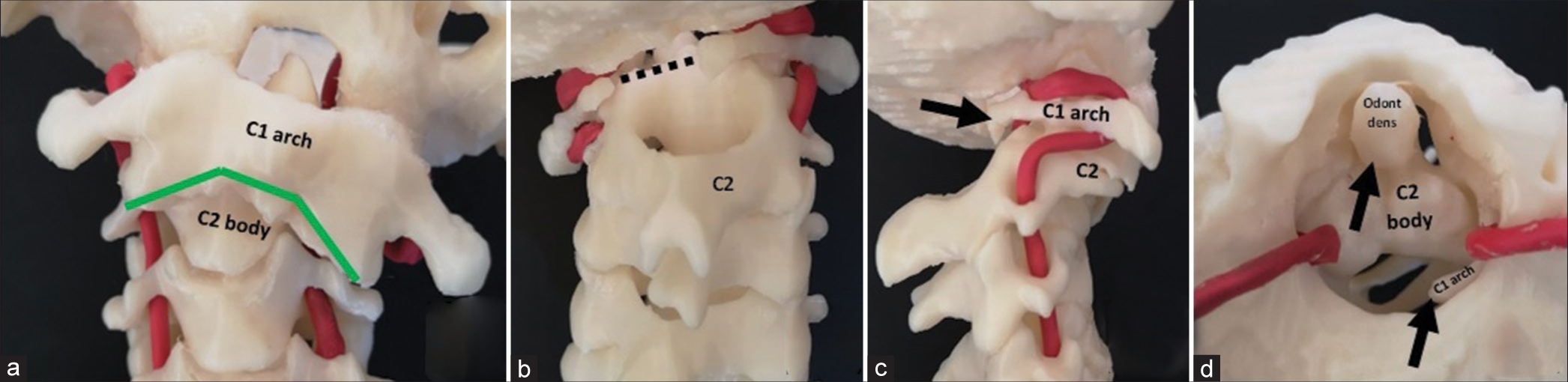
Figure 2:
Patient’s C-Spine 3D model. (a) Anterior view, the green line highlights the area to perform surgical bone disarticulation. (b) Posterior view, black dotted line represents the previously surgically removed C1 posterior arch. (c) Right lateral view, black arrow represents the subluxation vector of C1 over C2. Bird’s eye view, black arrows represent the C1 and odontoid tip subluxation over the C2 body.
DISCUSSION
Nonsurgical treatment of type II fractures has a high rate of non-union. Standard surgical options include an anterior approach (i.e., using an odontoid compression screw) or a posterior approach (i.e., using different techniques to achieve C1-C2 arthrodesis).[
CONCLUSION
Emerging 3D CT reconstructive technologies can now facilitate complex operative planning. Here, it was utilized to plan a secondary 360° fusion procedure where prior operative management of a traumatic type II odontoid fracture had resulted in a rotatory C1-C2 pseudoarthrosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Elgafy H, Dvorak MF, Vaccaro AR, Ebraheim N. Treatment of displaced Type II odontoid fractures in elderly patients. Am J Orthop (Belle Mead NJ). 2009. 38: 410-6
2. Hoarau R, Zweifel D, Simon C, Broome M. The use of 3D planning in facial surgery: Preliminary observations. Rev Stomatol Chir Maxillofac Chir Orale. 2014. 115: 353-60
3. Joaquim AF, Patel AA. Surgical treatment of Type II odontoid fractures: Anterior odontoid screw fixation or posterior cervical instrumented fusion?. Neurosurg Focus. 2015. 38: E11
4. Maak TG, Grauer JN. The contemporary treatment of odontoid injuries. Spine (Phila Pa 1976). 2006. 31: S53-60
5. Sembrano JN, Santos ERG, Polly DW. New generation intraoperative three-dimensional imaging (O-arm) in 100 spine surgeries: Does it change the surgical procedure?. J Clin Neurosci. 2014. 21: 225-31
6. Yang Z, Yuan ZZ, Ma JX, Ma XL. Conservative versus surgical treatment for Type II odontoid fractures in the elderly: Grading the evidence through a meta-analysis. Orthop Traumatol Surg Res. 2015. 101: 839-44

