

- Department of Life, Health and Environmental Sciences (MESVA), University of L'Aquila, L'Aquila, Italy
- Department of Neurosurgery, San Salvatore City Hospital, L'Aquila, Italy
Correspondence Address:
Danilo De Paulis
Department of Life, Health and Environmental Sciences (MESVA), University of L'Aquila, L'Aquila, Italy
DOI:10.4103/2152-7806.163318
Copyright: © 2015 Di Vitantonio H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Vitantonio HD, Paulis DD, Ricci A, Marzi S, Dehcordi SR, Galzio RJ. Cavernous hemangioma of the dura mater mimicking meningioma. Surg Neurol Int 20-Aug-2015;6:
How to cite this URL: Vitantonio HD, Paulis DD, Ricci A, Marzi S, Dehcordi SR, Galzio RJ. Cavernous hemangioma of the dura mater mimicking meningioma. Surg Neurol Int 20-Aug-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/cavernous-hemangioma-of-the-dura-mater-mimicking-meningioma/
Abstract
Background:Cavernomas are benign lesions that most commonly occur intra-parenchymally, but occasionally they have been described as arising from the dura mater. Extra-axial cavernous angiomas (or hemangiomas) account for 0.4–2% of all intracranial vascular malformations, and they usually occur in the middle cranial fossa, associated with the cavernous sinus. Other possible localizations (e.g. tentorium, convexity, anterior cranial fossa, cerebellopontine angle, Meckel's cave, sella turcica and internal auditory meatus) are rare, and they account only for 0.2–0.5%.
Case Description:We report a case of a 30-year-old female presenting with a 2 years history of headache unresponsive to drug therapy. The magnetic resonance imaging showed a dural-based lesion in the left frontal region; the lesion size was: 1.5 cm × 3.5 cm. The appearance suggested a convexity meningioma. A left frontal craniotomy was performed, and the histopathological diagnosis deposed for a cavernous hemangioma of the dura mater. The follow-up at 1-year was good without any neurologic deficit.
Conclusions:Dural-based cavernous hemangiomas of the convexity are uncommon lesions. Up to now, only 13 cases have been described in the literature. The authors have discussed clinical aspects, radiological features, surgical treatment, and operative findings.
Keywords: Convexity, dural cavernous hemangioma, meningioma
INTRODUCTION
Cavernomas are benign lesions[
Extra-axial cavernous angiomas (or hemangiomas) account for 0.4–2% of all intracranial vascular malformations,[
The authors report the case of a convexity dural-based hemangioma in a young woman. Clinical aspects, radiological features, surgical treatment, and operative findings are discussed reviewing the literature.
CASE REPORT
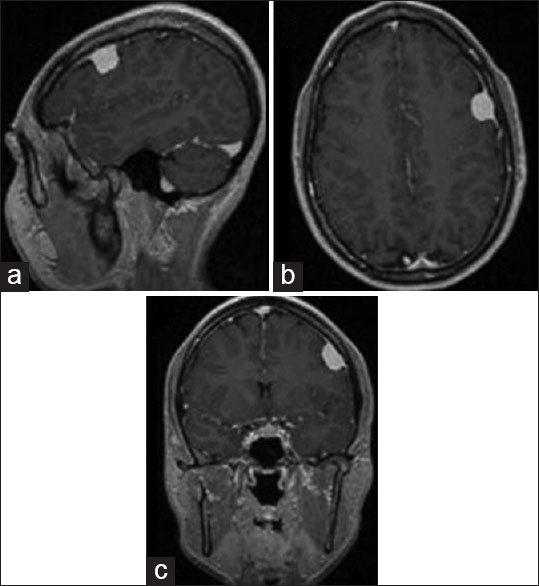
A 30-year-old female had a 2 years history of left frontal headache unresponsive to drug therapy with common analgesics. The intensity of this symptom increased over time. Her neurological examination was normal. The magnetic resonance imaging (MRI) showed a dural-based lesion in the left frontal region; the lesion size was 1.5 cm × 3.5 cm. It was hyperintense on T2-weighted images and isointense on T1-weighted images showing intense contrast enhancement. This small mass appeared to be adherent to the dura mater with a dural tail sign [
Initially, the patient refused surgery.
After 1-year, brain control MRI showed no changes of the lesion.
Finally, the patient decided to undergo surgery because the episodes of headaches had become more and more frequent and intense.
A left frontal craniotomy was performed. After opening the dura, an encapsulated, red-colored tumor was exposed. The base of the implant was coagulated and the lesion was removed en-bloc without significant intraoperative bleeding.
The histopathological diagnosis deposed for a cavernous hemangioma of the dura mater [
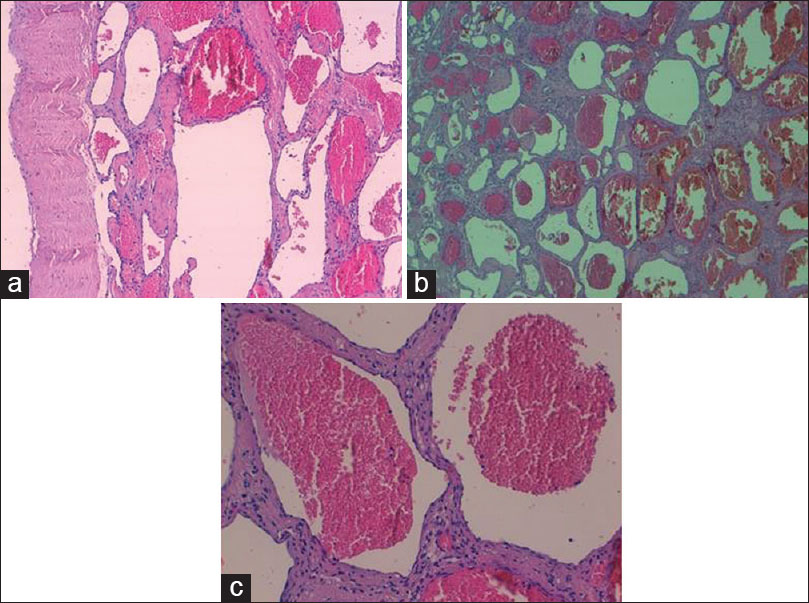
Figure 2
Histological examination showed a multilobulated lesion (b) composed of sinusoidal vascular spaces of various sizes lined with a single layer of endothelial cells (a and c). These vascular spaces are separated by fibrous connective tissue (a). H and E, ×4 (a); H and E, ×10 (b); H and E, ×40 (c)
The postoperative MRI showed no residual hemangioma [
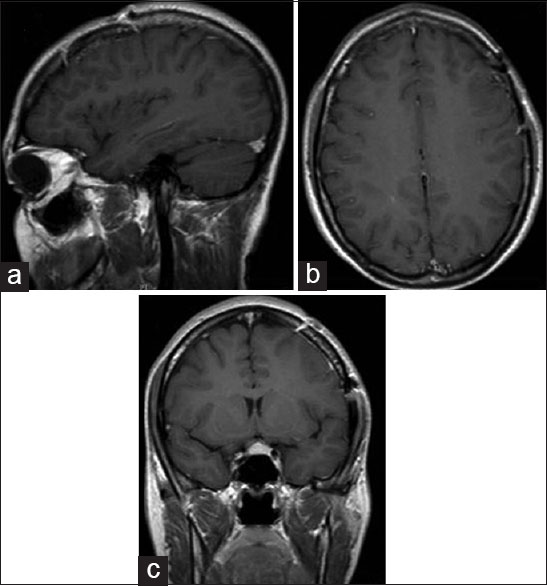
At 1-year follow-up, the patient was asymptomatic without any neurologic deficit.
DISCUSSION
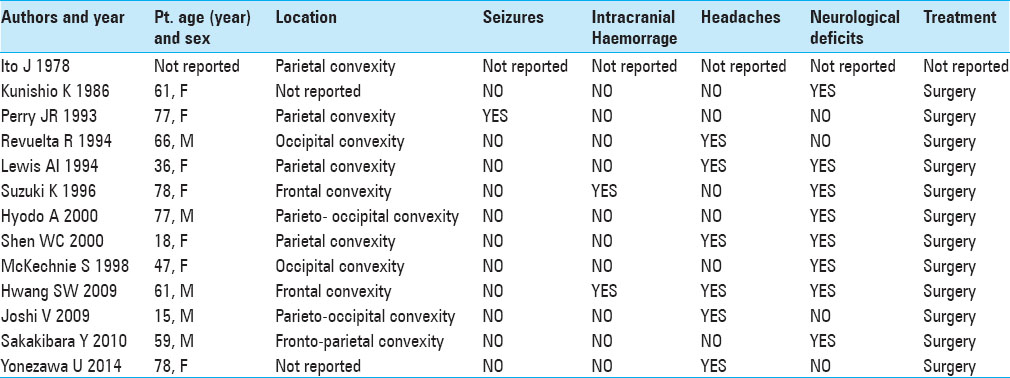
Dural-based cavernous hemangiomas of the convexity are uncommon lesions. Up to now, only 13 cases have been described in the literature.[
Reviewing the literature, we note that the average age is 52 years, and only in 2 cases the patients are 18 and 15 years old. There is a slight female prevalence (7:6) and the most frequent localization is the parietal convexity. Some cases are associated with a nonspecific focal neurological deficit, and headache is the most common symptom. In only 1 case, there is association with seizures. There is not enough evidence to show that lesions are predisposed to bleeding because in only 2 cases they are associated with hemorrhage. In all these cases, the treatment of choice is surgery without the need for radiation or embolization [
The cavernous hemangiomas are vascular malformations made up of sinusoidal vascular spaces of various sizes lined with a single layer of endothelial cells. These vascular spaces are separated by fibrous connective tissue.[
Although dural cavernous hemangiomas are benign entities, sometimes they can grow very quickly to reach a considerable size over 2 years.[
On the contrary, in our case, after 12 months the cavernous hemangioma showed no signs of growth.
Cavernous dural hemangiomas of the convexity can closely resemble meningiomas on computed tomography (CT) and MRI in terms of signal characteristics, enhancement pattern, and localization.[
In MRI, both lesions are usually isointense or hypointense on T1-weighted images, and isointense or mildly hyperintense on T2-weighted images with intense contrast enhancement.[
The CT appearance of dural cavernous hemangiomas, like meningiomas, shows a well-defined extra-axial mass lesion on a broad dural base with regular contrast.[
The cerebral angiography may not be performed when CT or MRI findings are felt to be diagnostic, and the lesion is surgically accessible.[
In 1994 Lewis et al. published a review of the literature where they subdivided dural cavernous malformations into two groups: The cavernous hemangiomas located in the middle fossa and those located outside of it.[
On the contrary, in the cases of the second group, neither radiation nor embolization is necessary to successfully remove cavernous hemangiomas outside the middle fossa,[
In our era, in which stereotactic radiosurgery represents a therapeutic option, a histopathological confirmation is needed. This seems to be influential because dural cavernous hemangiomas are different from meningiomas in their clinical features such as surgical difficulty and sensitivity to radiosurgery.[
CONCLUSIONS
We believe that the occurrence of dural hemangiomas should always be suspected in the presence of extra-axial lesions of the convexity, especially if neuroradiological data suggest a meningioma. Therefore, according to our opinion, the treatment of choice should always be surgery since it is necessary to have the histopathological confirmation. In addition, dural hemangiomas of the convexity are surgically more accessible than cavernomas of the middle cranial fossa, and, for this reason, their remotion provides a better prognosis.
ACKNOWLEDGMENT
The authors thank Maria Silvia Marottoli for her assistance to the translation.
References
1. Buonaguidi R, Canapicci R, Mimassi N, Ferdeghini M. Intrasellar cavernous hemangioma. Neurosurgery. 1984. 14: 732-4
2. Gutiérrez-González R, Casanova-Peño I, Porta-Etessam J, Martínez A, Boto GR. Dural cavernous haemangioma of the anterior cranial fossa. J Clin Neurosci. 2010. 17: 936-8
3. Hwang SW, Pfannl RM, Wu JK. Convexity dural cavernous malformation with intradural and extradural extension mimicking a meningioma: A case report. Acta Neurochir (Wien). 2009. 151: 79-83
4. Hyodo A, Yanaka K, Higuchi O, Tomono Y, Nose T. Giant interdural cavernous hemangioma at the convexity. Case illustration. J Neurosurg. 2000. 92: 503-
5. Ito J, Konno K, Sato I, Kameyama S, Takeda S. Convexity cavernous hemangioma, its angiographic and CT findings. Report of a case. No To Shinkei. 1978. 30: 737-47
6. Joshi V, Muzumdar D, Dange N, Goel A. Supratentorial convexity dural-based cavernous hemangioma mimicking a meningioma in a child. Pediatr Neurosurg. 2009. 45: 141-5
7. Kunishio K, Sunami N, Yamamoto Y, Satoh T, Asari S, Ohtsuki Y. A case of convexity cavernous hemangioma associated with meningioma. No Shinkei Geka. 1986. 14: 1487-91
8. Lewis AI, Tew JM, Payner TD, Yeh HS. Dural cavernous angiomas outside the middle cranial fossa: A report of two cases. Neurosurgery. 1994. 35: 498-504
9. McKechnie S, Harper C, Besser M. Durally-based occipital cavernous haemangioma indistinguishable from meningioma. J Clin Neurosci. 1998. 5: 105-8
10. Melone AG, Delfinis CP, Passacantilli E, Lenzi J, Santoro A. Intracranial extra-axial cavernous angioma of the cerebellar falx. World Neurosurg. 2010. 74: 501-4
11. Perry JR, Tucker WS, Chui M, Bilbao JM. Dural cavernous hemangioma: an under-recognized lesion mimicking meningioma. Can J Neurol Sci. 1993. 20: 230-3
12. Revuelta R, Teixeira F, Rojas R, Juambelz P, Romero V, Valdes J. Cavernous hemangiomas of the dura mater at the convexity. Report of a case and therapeutical considerations. Neurosurg Rev. 1994. 17: 309-11
13. Sakakibara Y, Matsumori T, Taguchi Y, Koizumi H. Supratentorial high convexity intradural extramedullary cavernous angioma: case report. Neurol Med Chir (Tokyo). 2010. 50: 328-9
14. Shen WC, Chenn CA, Hsue CT, Lin TY. Dural cavernous angioma mimicking a meningioma and causing facial pain. J Neuroimaging. 2000. 10: 183-5
15. Suzuki K, Kamezaki T, Tsuboi K, Kobayashi E. Dural cavernous angioma causing acute subdural hemorrhage-case report. Neurol Med Chir (Tokyo). 1996. 36: 580-2
16. Yonezawa U, Ikawa F, Hamasaki O, Hidaka T, Kurokawa Y, Onuma H. A case of cavernous angioma at the convexity in the dura mater: Characteristics of images in the literature. No Shinkei Geka. 2014. 42: 731-5

