

- Department of Neurosurgery, Sapporo Medical University, Sapporo, Japan
- Department of Neurosurgery, Hokkaido University, Graduate School of Medicine, Sapporo, Japan
Correspondence Address:
Takeshi Mikami
Department of Neurosurgery, Sapporo Medical University, Sapporo, Japan
DOI:10.4103/2152-7806.159372
Copyright: © 2015 Horita Y. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Horita Y, Mikami T, Houkin K, Mikuni N. Cerebral aneurysms associated with segmental dilative arteriopathy of the circle of Willis. Surg Neurol Int 25-Jun-2015;6:
How to cite this URL: Horita Y, Mikami T, Houkin K, Mikuni N. Cerebral aneurysms associated with segmental dilative arteriopathy of the circle of Willis. Surg Neurol Int 25-Jun-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/cerebral-aneurysms-associated-with-segmental-dilative-arteriopathy-of-the-circle-of-willis/
Abstract
Background:Dilative arteriopathy is a form of dolichoectasia. It is sometimes observed in the posterior circulation, and it may be associated with various type of stroke. Herein, we report two unusual cases of saccular aneurysms associated with a segmental dilative arteriopathy located in the anterior circulation.
Case Descriptions:The first case is a 39-year-old woman with irregular tortuosity and coiling of the left internal cerebral artery along with saccular aneurysms in this artery. The second case is a 45-year-old woman presenting with a ruptured saccular aneurysm in the coiling of the anterior cerebral artery. In both cases, the aneurysm was clipped successfully, and the patients recovered uneventfully with no neurological deficits.
Conclusion:Dilative arteriopathy of the circle of Willis is an unusual anomaly and is characterized by tortuous and elongated arteries, which are sometimes observed in patients with a congenital anomaly. This report describes two cases of saccular aneurysm associated with dilative arteriopathy of the circle of Willis with no medical history, which to the best of our knowledge has not previously been described.
Keywords: Anterior cerebral artery, arteriopathy, dolichoectasia, subarachnoid hemorrhage
INTRODUCTION
Dolichoectasia is a broad concept that may include many diseases. Intracranial dolichoectasia is characterized by enlargement, tortuosity, and elongation of the major arteries of the brain and is typically observed in the posterior circulation.[
CASE REPORTS
Case 1
A 39-year-old woman with no remarkable medical or familial history underwent magnetic resonance (MR) imaging for headache. MR angiography and three-dimensional (3D) computed tomographic (CT) angiography revealed irregular tortuosity of the ICA from the ophthalmic artery to the terminal portion (C1, C2) on the left side and saccular aneurysms in the left C1. Cerebral angiography revealed that the ICA coiled twice between the ophthalmic artery and the anterior choroidal artery and contained four saccular aneurysms distal to the posterior communicating artery [
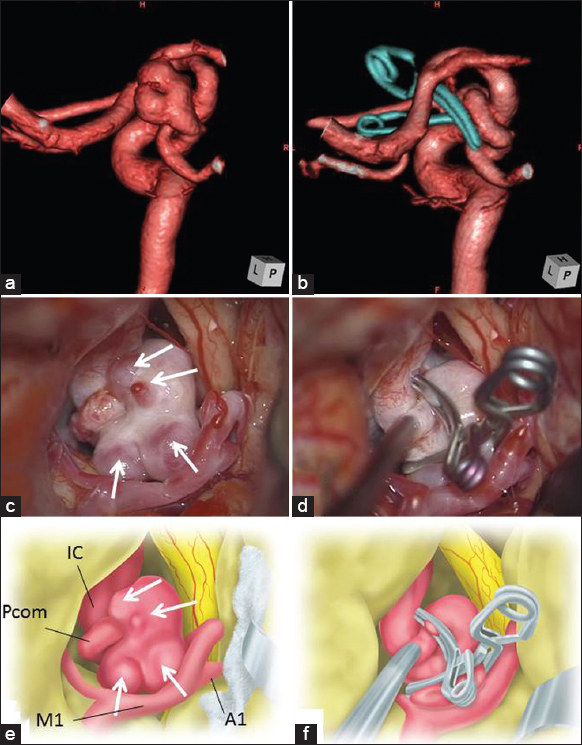
Figure 1
(a) Three-dimensional digital subtraction angiography (DSA) showing the elongated and tortuous left internal cerebral artery (ICA) with saccular aneurysms (white arrow). (b) Postoperative DSA showing successful clipping of these aneurysms. Intraoperative photographs (c and d) and illustrations. (e and f) Enlarged and tortuous left ICA with saccular aneurysms (arrow), and successful clipping of these aneurysms
The patient was taken for microsurgical exploration. The left ICA was dilated and coiled. During temporary occlusion of the ICA, the artery collapsed completely; no arterial dissection or atherosclerotic changes were observed [Figure
Case 2
A 45-year-old woman with no remarkable medical or familial history suddenly developed a severe headache and nausea and was immediately transported to our hospital by ambulance. At the time of admission, she experienced mild consciousness disturbance but no other neurological deficits. She had no history of head trauma or connective tissue disorder. CT revealed diffuse subarachnoid hemorrhage, and 3D CT angiography and cerebral angiography revealed irregular tortuosity of the horizontal portion of the ACA (A1) on the left side and a saccular aneurysm in the left A1 segment [Figure
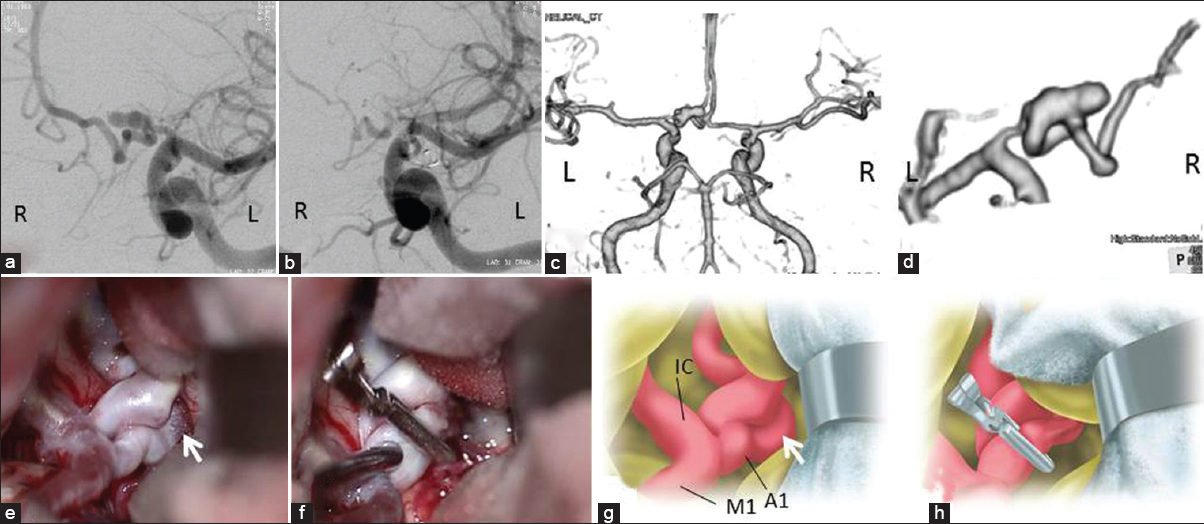
Figure 2
(a) Digital subtraction angiography (DSA) showing the elongated and tortuous left anterior cerebral artery (ACA) with saccular aneurysm (white arrow). (b) Postoperative DSA showing successful clipping of the aneurysm. Preoperative three-dimensional computed tomographic angiography (c and d), intraoperative photographs (e and f) and illustrations. (g and h) Enlarged and tortuous left ACA with saccular aneurysm (arrow), and successful clipping of the aneurysm
On day 1, the patient was taken to the operating room for microsurgical exploration, and a left frontotemporal craniotomy was performed. The dome of the aneurysm, including the rupture point, was buried in the frontal lobe. The left A1 was dilated, elongated, and tortuous [Figure
DISCUSSION
Several diseases have been implicated as potential causes of dilative arteriopathy, including both congenital and acquired conditions.[
Although associated saccular aneurysms are typically induced by hemodynamic stress due to dilative arteriopathy, most aneurysms associated with dolichoectasia are dissecting aneurysms or fusiform aneurysms.[
References
1. Anson JA, Lawton MT, Spetzler RF. Characteristics and surgical treatment of dolichoectatic and fusiform aneurysms. J Neurosurg. 1996. 84: 185-93
2. Baccin CE, Krings T, Alvarez H, Ozanne A, Lasjaunias PL. A report of two cases with dolichosegmental intracranial arteries as a new feature of PHACES syndrome. Childs Nerv Syst. 2007. 23: 559-67
3. Beringer W, Alenghat J. Pericallosal artery ectasia with associated stenosis. AJNR Am J Neuroradiol. 2004. 25: 1197-8
4. Dhouib A, Beghetti M, Didier D. Imaging findings in a child with Loeys-Dietz syndrome. Circulation. 2012. 126: 507-8
5. Doran SE, Deveikis JP, Chandler WF. Dolichoectasia of the anterior cerebral arteries in an adolescent. AJNR Am J Neuroradiol. 1995. 16: 1548-50
6. Gutierrez J, Sacco RL, Wright CB. Dolichoectasia-an evolving arterial disease. Nat Rev Neurol. 2011. 7: 41-50
7. Heyer GL, Dowling MM, Licht DJ, Tay SK, Morel K, Garzon MC. The cerebral vasculopathy of PHACES syndrome. Stroke. 2008. 39: 308-16
8. Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: Angiographic aspects with embryological discussion. Anat Clin. 1984. 6: 133-41
9. Makos MM, McComb RD, Hart MN, Bennett DR. Alpha-glucosidase deficiency and basilar artery aneurysm: Report of a sibship. Ann Neurol. 1987. 22: 629-33
10. Mercurius KO, Morla AO. Inhibition of vascular smooth muscle cell growth by inhibition of fibronectin matrix assembly. Circ Res. 1998. 82: 548-56
11. Mitsias P, Levine SR. Cerebrovascular complications of Fabry's disease. Ann Neurol. 1996. 40: 8-17
12. Mizutani T, Kojima H. Clinicopathological features of non-atherosclerotic cerebral arterial trunk aneurysms. Neuropathology. 2000. 20: 91-7
13. Nakatomi H, Segawa H, Kurata A, Shiokawa Y, Nagata K, Kamiyama H. Clinicopathological study of intracranial fusiform and dolichoectatic aneurysms: Insight on the mechanism of growth. Stroke. 2000. 31: 896-900
14. Pessin MS, Chimowitz MI, Levine SR, Kwan ES, Adelman LS, Earnest MP. Stroke in patients with fusiform vertebrobasilar aneurysms. Neurology. 1989. 39: 16-21
15. Smoker WR, Corbett JJ, Gentry LR, Keyes WD, Price MJ, McKusker S. High-resolution computed tomography of the basilar artery: 2. Vertebrobasilar dolichoectasia: Clinical-pathologic correlation and review. AJNR Am J Neuroradiol. 1986. 7: 61-72
16. Tronc F, Mallat Z, Lehoux S, Wassef M, Esposito B, Tedgui A. Role of matrix metalloproteinases in blood flow-induced arterial enlargement: Interaction with NO. Arterioscler Thromb Vasc Biol. 2000. 20: E120-6
17. Yamada K, Hayakawa T, Ushio Y, Mitomo M. Cerebral arterial dolichoectasia associated with moyamoya vessels. Surg Neurol. 1985. 23: 19-24
18. Yu YL, Moseley IF, Pullicino P, McDonald WI. The clinical picture of ectasia of the intracerebral arteries. J Neurol Neurosurg Psychiatry. 1982. 45: 29-36

