

- Tecnologico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Monterrey, Nuevo Leon, Mexico.
DOI:10.25259/SNI_53_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ana S. Ferrigno, Jose A. Figueroa-Sanchez. Coexisting arachnoid cyst and tentorial sinus: A therapeutic dilemma. 12-Sep-2020;11:280
How to cite this URL: Ana S. Ferrigno, Jose A. Figueroa-Sanchez. Coexisting arachnoid cyst and tentorial sinus: A therapeutic dilemma. 12-Sep-2020;11:280. Available from: https://surgicalneurologyint.com/surgicalint-articles/10260/
Date of Submission
10-Feb-2020
Date of Acceptance
04-May-2020
Date of Web Publication
12-Sep-2020
Abstract
A 4-year-old male presented with a large arachnoid cyst over the left temporal region causing displacement of adjacent structures. Cerebral angiography showed dilatation of the tentorial sinus without other apparent vascular alterations. The association of these two anomalies raises a therapeutic dilemma as no information is available about how the variants of the venous system can modify cerebrospinal fluid hydrodynamics and thus affect arachnoid cyst’s prognosis. In this case, the patient was treated conservatively and has remained stable for 2 years.
Keywords: Arachnoid cyst, Tentorial sinus, Vein of Galen
CASE DESCRIPTION
A 4-year-old male presented to the emergency department with a mild traumatic brain injury after sustaining a 1 m fall from a staircase. His previous medical history was unremarkable except for occasional episodes of mild holocraneal cephalea during the previous year that could be effectively treated with over-the-counter acetaminophen. Unenhanced head computed tomography (CT) revealed a Galassi type 3 arachnoid cyst over the left temporal region that measured 5.7 × 9.5 × 9.3 cm, causing displacement of adjacent structures. Magnetic resonance imaging (MRI) study showed an abnormal dilatation of probable venous origin [
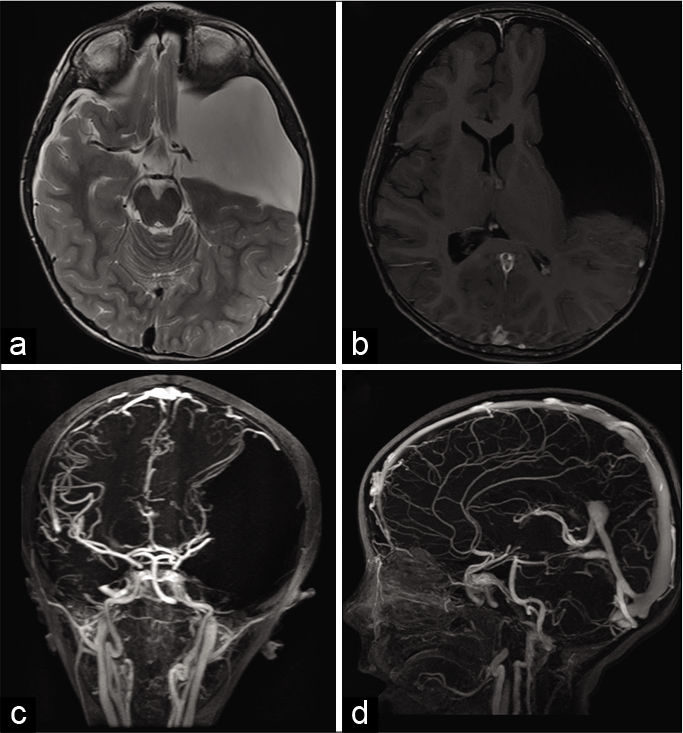
Figure 1:
Magnetic resonance imaging. (a) The T2-weighted image demonstrates a large arachnoid cyst classified as Galassi type 3 in in the left hemisphere. (b) A contrast-enhanced T1-weighted image shows an abnormal vascular dilation in proximity to the site of the vein of Galen. (c) Time-of-flight angiography revealed displacement of vascular structures in proximity to the arachnoid cyst and (d) abnormal dilatation of probable venous origin.
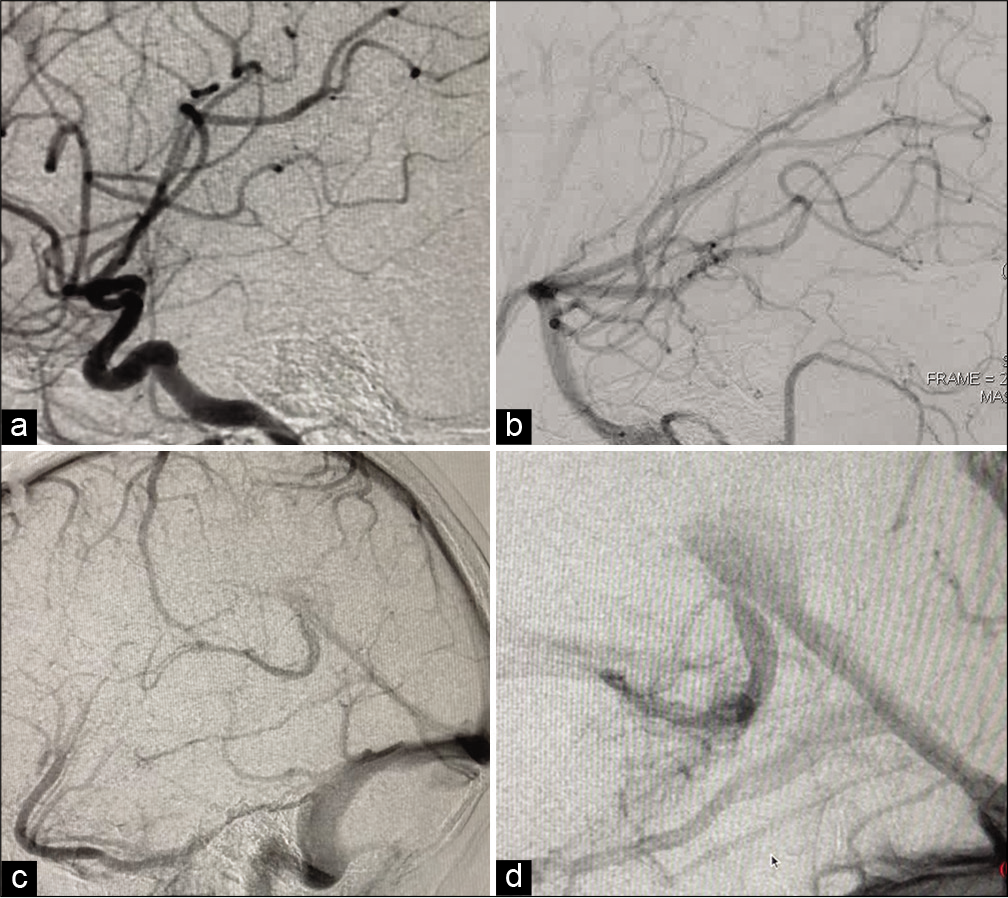
Figure 2:
Digital subtraction angiography. (a) Lateral view of the arterial phase of the right carotid artery and (b) vertebrobasilar artery failed to reveal vascular malformations and excluded early venous filling. (c and d) On venous phase, a vascular dilation suggestive of a tentorial sinus was observed.
DISCUSSION
Arachnoid cysts are a structural anomaly, in which abnormal splitting or duplication of the arachnoid membrane exists, allowing for cerebrospinal fluid (CSF) accumulation.[
On the other hand, the venous dilatation observed in the MRI study was initially classified as a vein of Galen aneurysmal dilatation. The vein of Galen is a midline venous structure that is formed by the embryonic remnant of the caudal median prosencephalic vein when it joins the internal cerebral veins.[
No previous studies have reported an association of tentorial sinus and arachnoid cysts. We speculate that the tentorial sinus is a normal anatomical variant that can be enlarged due to abnormal blood flow secondary to compression of vascular structures by the arachnoid cyst. The association of these two abnormalities is relevant given that the dilatation of venous structures can be an indirect sign of high pressure in the venous system, impeding CSF reabsorption, and favoring arachnoid cyst enlargement. This unique clinical presentation raises a therapeutic dilemma as no information is available about how the variants of the venous system can modify CSF hydrodynamics and thus affect arachnoid cyst’s prognosis. In this case, the patient was treated conservatively with close clinical follow-up and has remained stable for 2 years.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Al-Holou WN, Yew AY, Boomsaad ZE, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in children. J Neurosurg Pediatr. 2010. 5: 578-85
2. Hall S, Smedley A, Sparrow O, Mathad N, Waters R, Chakraborty A. Natural history of intracranial arachnoid cysts. World Neurosurg. 2019. 126: e1315-20
3. Miabi Z, Midia R, Rohrer SE, Hoeffner EG, Vandorpe R, Berk CM. Delineation of lateral tentorial sinus with contrast-enhanced MR imaging and its surgical implications. Am J Neuroradiol. 2004. 25: 1181-8
4. Mizutani K, Miwa T, Akiyama T, Sakamoto Y, Fujiwara H, Yoshida K. Fate of the three embryonic dural sinuses in infants: The primitive tentorial sinus, occipital sinus, and falcine sinus. Neuroradiology. 2018. 60: 325-33
5. Spazzapan P, Milosevic Z, Velnar T. Vein of Galen aneurismal malformations-clinical characteristics, treatment and presentation: Three cases report. World J Clin Cases. 2019. 7: 855-62

