

- Stroke Center, Yamagata City Hospital Saiseikan, Yamagata, Japan.
- Department of Neurosurgery, Yamagata University, Yamagata, Japan.
Correspondence Address:
Tetsu Yamaki
Department of Neurosurgery, Yamagata University, Yamagata, Japan.
DOI:10.25259/SNI_202_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Tetsu Yamaki1, Rei Kondo1, Kenshi Sano1, Hiroshi Honma1, Atsushi Kuge1, Shinjiro Saito1, Yukihiko Sonoda2. Coil embolization of subarachnoid hemorrhage with ruptured persistent primitive olfactory artery aneurysm. 08-Apr-2021;12:147
How to cite this URL: Tetsu Yamaki1, Rei Kondo1, Kenshi Sano1, Hiroshi Honma1, Atsushi Kuge1, Shinjiro Saito1, Yukihiko Sonoda2. Coil embolization of subarachnoid hemorrhage with ruptured persistent primitive olfactory artery aneurysm. 08-Apr-2021;12:147. Available from: https://surgicalneurologyint.com/surgicalint-articles/10696/
Date of Submission
27-Feb-2021
Date of Acceptance
13-Mar-2021
Date of Web Publication
08-Apr-2021
Abstract
Background: Persistent primitive olfactory artery (PPOA) is a rare anomaly of the anterior cerebral artery. We experienced a rare case of subarachnoid hemorrhage caused by a ruptured saccular aneurysm of PPOA.
Case Description: A 72-year-old man was transported to our hospital with sudden headache. On examination, World Federation of Neurological Surgeons scale was Grade I, and computed tomography of the head showed subarachnoid hemorrhage in Fisher Group 3. Cerebral angiography showed left PPOA and a 4-mm saccular aneurysm at the hairpin turn. No other abnormalities causing bleeding were observed. Based on these findings, subarachnoid hemorrhage due to a ruptured PPOA aneurysm was diagnosed. As the patient had a ventilatory defect due to emphysema, direct approach to the lesion would have been difficult and an endovascular surgery was performed. Three coils were inserted into the aneurysm, and complete occlusion was achieved. Cerebral vasospasm was not observed, and the patient was discharged 1 month after surgery without any neurologic deficit.
Conclusion: Most aneurysms of the PPOA are formed at the hairpin turn, as observed in our patient; therefore, a hemodynamic mechanism may be involved in the etiology. To the best of our knowledge, there is no report on treatment using intra-aneurysmal coil embolization, indicating that ours was the first case. As the long-term outcome of intra-aneurysmal coil embolization for PPOA aneurysm is unknown, careful follow-up will be necessary in the future.
Keywords: Intra-aneurysmal coil embolization, Persistent primitive olfactory artery, Subarachnoid hemorrhage
INTRODUCTION
Persistent primitive olfactory artery (PPOA) is a rare anomaly of the anterior cerebral arteries.[
CASE DESCRIPTION
A 72-year-old man presented to our department with a sudden headache. Neurological examination on admission revealed a Glasgow coma scale score of 15 (E4V4M6). No neurological deficit was observed, and the World Federation of Neurological Surgeons score was Grade I. Computed tomography of the head revealed subarachnoid hemorrhage, classified as Fisher Group 3. Emergency cerebral angiography of the left internal carotid artery revealed that the left anterior cerebral artery coursed anteromedially and downward after division from the internal carotid artery, turned in an extreme acute angle, headed upwards, and ran posteriorly over the corpus callosum as a pericallosal artery. The anterior communicating artery was not visualized, and the Heubner artery branched from the A1 segment. Based on this characteristic course, we suspected it to be a PPOA [
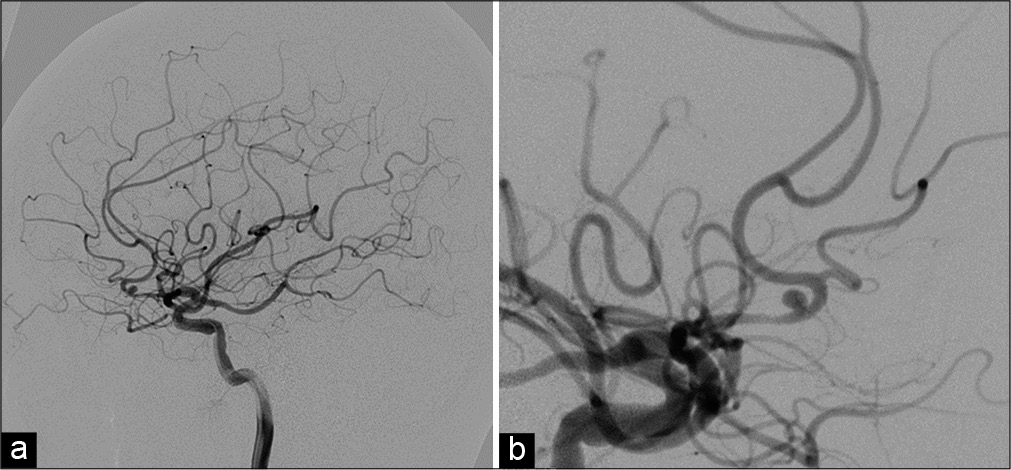
Figure 1:
Preoperative left internal carotid angiograms showing anomalous arteries arising from the internal carotid arteries, which and run anteromedially along the frontal base and making a hairpin-pin bend, and a saccular aneurysm is seen on the hairpin-pin bend, lateral view (a) and oblique view (b).
Based on the findings, we diagnosed the condition as subarachnoid hemorrhage due to a ruptured aneurysm of PPOA. The patient had emphysema before admission, and ventilatory defect developed after administration of general anesthesia. Therefore, a direct open approach by craniotomy was considered difficult, and endovascular surgery was performed.
A 7 Fr Launcher (Medtronic, Minneapolis, MN, USA) was placed in the left internal carotid artery from the right femoral artery, while maintaining the activated clotting time >200 s under administration of systemic heparin, and 4.2 Fr ASAHI FUBUKI (ASAHI INTEC, Aichi) was guided to a C2 portion of the internal carotid artery as an intermediate catheter. From there, the Excelsior SL-10 reshaped J microcatheter (Stryker, Kalamazoo, MI, USA) was guided into the aneurysm with Transend EX platinum (Stryker, Kalamazoo, MI, USA). A cage was formed with Axium PRIME 3D (Medtronic, Minneapolis, MN, USA). Three coils were inserted into the aneurysm, and nearly complete occlusion was achieved [
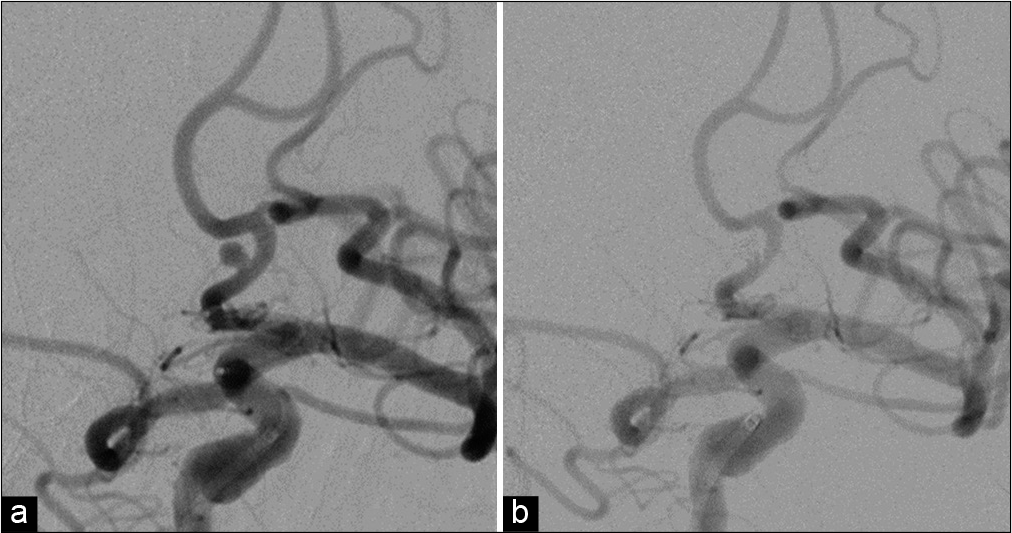
Postoperatively, the patient showed no symptomatic cerebral vasospasm and was discharged from the hospital 1 month after surgery without neurologic deficit. Cerebral angiography before discharge showed favorable embolization of the aneurysm.
DISCUSSION
Intracranial carotid arteries are embryologically classified into cranial and caudal divisions.[
PPOA Type 1 branches from the internal carotid artery terminal, runs toward the olfactory bulb, runs anteriorly along the olfactory tract, sharply turns in the rear upper direction (hairpin turn), and is connected to the distal part of the anterior cerebral artery. PPOA Type 2 branches from the anterior cerebral artery as the orbitofrontal artery, runs into the nasal cavity through the cribriform plate, and becomes the ethmoidal artery.[
Although residual PPOA itself does not cause symptoms, some patients have been reported to present with anosmia or an aneurysm as a complication.[
This patient underwent radical endovascular surgery. Due to the presence of a PPOA aneurysm at the hairpin turn without a branch, difficulty in the stable placement of the microcatheter in the aneurysm was considered. Therefore, an intermediate catheter was used to improve the stability of the microcatheter. Further, an aneurysm of the PPOA has a wide neck.[
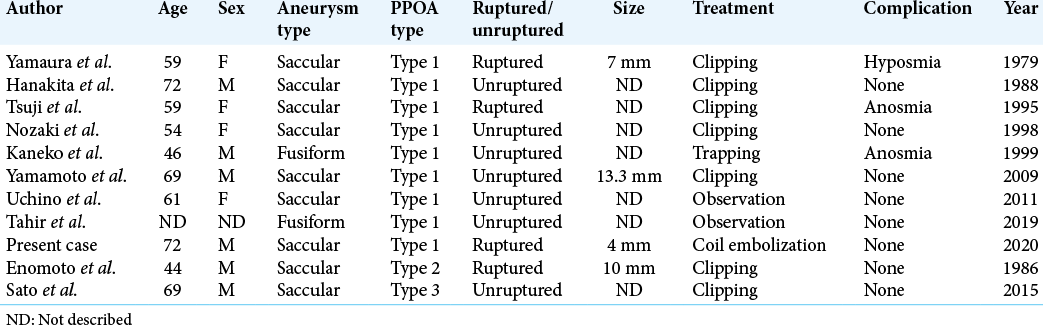
To the best of our knowledge, 11 patients with PPOA aneurysms have been reported, including our patient:[
CONCLUSION
This is the first report of coil embolization for persistent primitive olfactory astery aneurysm.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Enomoto H, Goto H, Murase M. A ruptured cerebral aneurysm of the fronto-oribital artery and the existing anastomosis with the anterior ethmoidal artery. No Shinkei Geka. 1986. 14: 203-6
2. Hanakita J, Nagayasu S, Nishi S, Suzuki T. An aneurysm of the distal anterior cerebral artery with a remarkably anomalous configuration. No Shinkei Geka. 1988. 16: 781-4
3. Horie N, Morikawa M, Fukuda S, Hayashi K, Suyama K, Nagata I. New variant of persistent primitive olfactory artery associated with a ruptured aneurysm. J Neurosurg. 2012. 117: 26-8
4. Kaneko T, Suetake K, Shinya T, Takeda M. Persistent primitive olfactory artery: report of 5 cases. No Shinkei Geka. 1999. 27: 933-9
5. Kuwabara S, Ishikawa S, Andoh S, Matsumoto S, Sekimoto H, Uemura Y. Aneurysms of the distal anterior cerebral artery. Report of 18 cases and review of 191 reported cases. Neurol Med Chir (Tokyo). 1984. 24: 580-90
6. Moffat DB. A case of persistence of the primitive olfactory artery. Anat Anz. 1967. 121: 477-9
7. Nozaki K, Taki W, Kawanami O, Hashimoto N. Cerebral aneurysm associated with persistent primitive olfactory artery aneurysm. Acta Neurochir (Wien). 1998. 140: 397-402
8. Paget DH.editors. The Development of the Cranial Arteries in the Human Embryo. Contributions to Embryology. Washington, DC: Carnegie Institution; 1948. p. 205-61
9. Sato Y, Kashimura H, Takeda M, Chida K, Kubo Y, Ogasawara K. Aneurysm of the A1 segment of the anterior cerebral artery associated with the persistent primitive olfactory artery. World Neurosurg. 2015. 84: 2079.e7-9
10. Tahir RA, Haider S, Kole M, Griffith B, Marin H. Anterior cerebral artery: Variant anatomy and pathology. J Vasc Interv Neurol. 2019. 10: 16-22
11. Tsuji T, Abe M, Tabuchi K. Aneurysm of a persistent primitive olfactory artery. Case report. J Neurosurg. 1995. 83: 138-40
12. Uchino A, Saito N, Kozawa E, Mizokoshi W, Inoue K. Persistent primitive olfactory artery: MR angiographic diagnosis. Surg Radiol Anat. 2011. 33: 197-201
13. Yamamoto T, Suzuki K, Yamazaki T, Tsuruta W, Tsurubuchi T, Matsumura A. Persistent primitive olfactory artery aneurysm. Neurol Med Chir (Tokyo). 2009. 49: 303-5
14. Yamaura A, Takase M, Makino H. An aneurysm of the proximal anterior cerebral artery at the olfactory bulb. Surg Neurol. 1979. 12: 425-7

