

- Department of Neurological Surgery, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York, United States
- Department of Pediatrics, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York, United States
Correspondence Address:
David A. Chesler
Department of Pediatrics, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York, United States
DOI:10.25259/SNI_536_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Megan E. Cosgrove1, Jordan Saadon1, David A. Chesler2. Colloid cyst curtailed: A case report of spontaneous colloid cyst regression. 29-Dec-2020;11:465
How to cite this URL: Megan E. Cosgrove1, Jordan Saadon1, David A. Chesler2. Colloid cyst curtailed: A case report of spontaneous colloid cyst regression. 29-Dec-2020;11:465. Available from: https://surgicalneurologyint.com/surgicalint-articles/10503/
Date of Submission
15-Aug-2020
Date of Acceptance
28-Oct-2020
Date of Web Publication
29-Dec-2020
Abstract
Background: Colloid cysts arise from the roof of the third ventricle and are at risk for obstructing the flow of cerebrospinal fluid (CSF) and causing increased intracranial pressure. With advancements and increased frequency of imaging, colloid cysts are sometimes discovered incidentally. In these cases, the neurosurgeon is faced with the decision of whether to intervene or manage conservatively.
Case Description: A 67-year-old man was discovered to have a colloid cyst when imaging was performed for transient neurologic deficits. CT and MRI brain revealed a 5mm lesion in the third ventricle with characteristics suggestive of the colloid cyst. Except for his initial presentation, the patient did not exhibit any symptoms and was followed with serial imaging. Four years after discovery, the colloid cyst regressed in size.
Conclusion: The evolution and resolution of colloid cysts remain elusive; however, the discovery of incidental colloid cysts due to more frequent and more advanced neuroimaging emphasize the importance of this topic. The fear of conservative management is acute decompensation due to obstruction of CSF. However, surgical risks may be avoided if these asymptomatic lesions regress and resolve without intervention. Conservative management is a viable option for patients with colloid cysts, who may not only avoid surgery but who might also rarely experience cyst resolution.
Keywords: Colloid cyst, Cyst, Third ventricle
INTRODUCTION
Colloid cysts are benign neoplasms of neuroepithelial origin, thought to be derived from the paraphysis of the roof of the third ventricle where they are typically located.[
Treatment of symptomatic colloid cysts requires neurosurgical intervention. Colloid cysts can be resected using microsurgical or endoscopic techniques, aspirated using stereotaxis, or patients can be shunted as a means to treat their symptoms.[
CASE REPORT
A 67-year-old man presented to the emergency room after the acute onset of neurologic deficits. The patient arose from bed with new-onset dizziness, left leg paresthesia, and gait abnormalities. His gait was described as “left-leaning” and ambulating was associated with the feeling of imminent syncope, although no syncopal episodes were reported. The patient also endorsed a frontal headache, in which he described as similar in intensity and quality to previous headaches. No symptoms were present the previous day or evening before bed, and the patient denied any previous reports of these symptoms, with the exception of chronic headaches. Medical history was significant for hypertension and hepatitis C; he was being treated with ledipasvir/ sofosbuvir at the time of evaluation. Family history revealed a brother who died suddenly from a brain aneurysm.
In the emergency room, there were no significant physical examination findings, including no focal neurologic deficits. CT brain revealed a 5 mm hyperdensity in the third ventricle, concerning for hemorrhage or neoplasm. MRI brain confirmed the presence of a cystic lesion in the third ventricle, which appeared to arise from the roof of the third ventricle posterior to the foramen of Monro. The foramen appeared patent bilaterally, and consistent with this, there was no associated ventriculomegaly. DWI did not reveal areas of restricted diffusion, making a cerebrovascular event unlikely, and MR angiogram was normal with the exception of a fetal posterior cerebral artery. There were no aneurysms, or arteriovenous malformations appreciated on MRA. The patient was determined to be neurologically stable, with likely an incidental finding of a colloid cyst. It was, therefore, recommended that he be expectantly managed with follow-up scans and was advised to seek immediate care if there was an abrupt change in neurologic status.
The patient was seen in the clinic for follow-up at 3 months at which point repeat imaging revealed the same cystic lesion unchanged in size, appearance, and location [
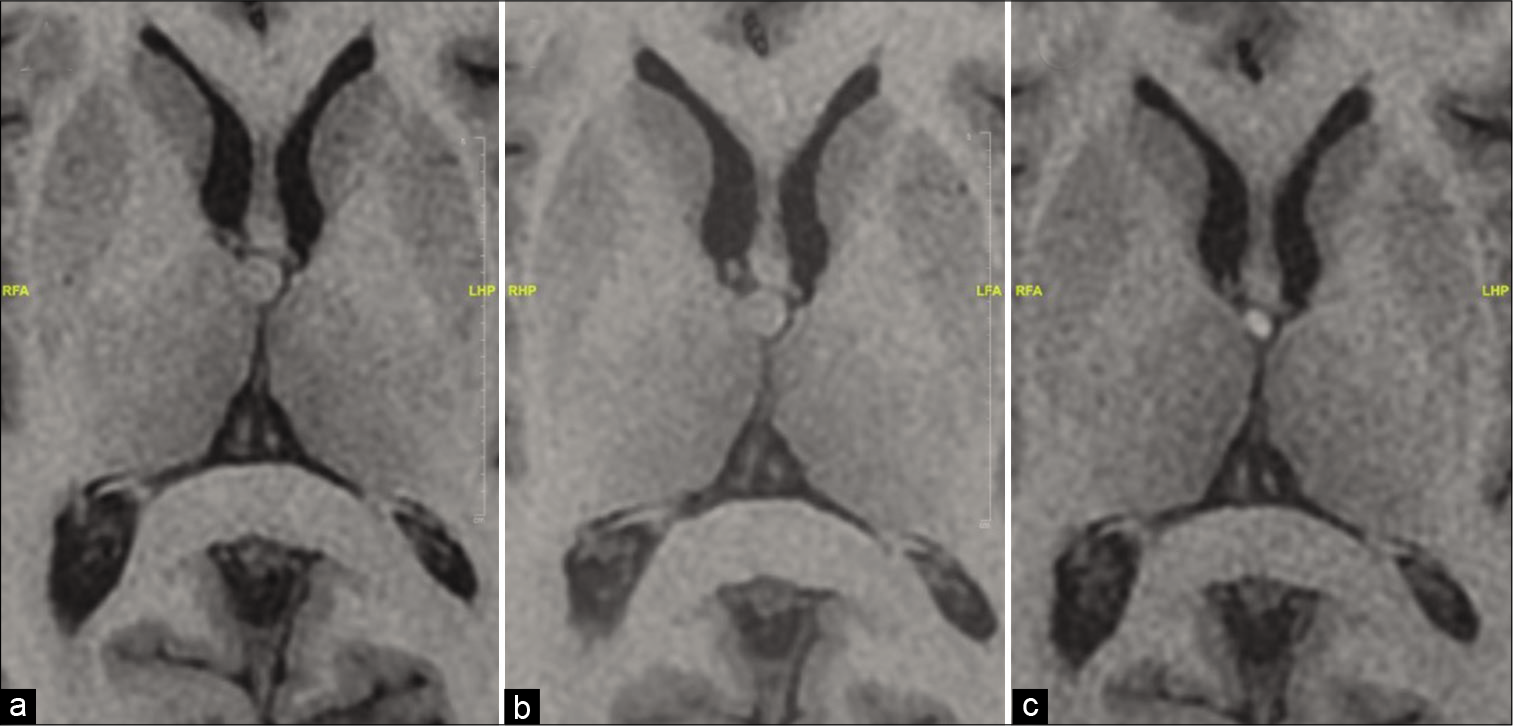
Figure 1:
T1 MRI axial images show the stability of the colloid cyst within the third ventricle, followed by regression images were acquired in July 2015 (a), August 2017 (b), and August 2019 (c). The cyst measured 5 mm initially and at follow-up scans 2 years later, and 2.5–3 mm at his follow-up scan in 2019. The 2019 scan also shows hyperintense signal in the cyst, suggesting colloid cyst involution.
DISCUSSION
Management of colloid cysts has typically been described in three different ways: definitive resection of the tumor, treatment of symptoms through a shunt and expectant management with regular imaging surveillance. Given the benign nature of this tumor type, with smaller, asymptomatic lesions, it is reasonable to choose surveillance over intervention and avoid the risks and complications associated with surgery. However, the risk of sudden death, which has been reported in cases of the untreated colloid cyst, along with improved surgical techniques with decreased risk, has caused some to favor intervention,[
Previous to this case report, there have been five other reports of patients observed to have had regression/ involution of a colloid cyst. The first report, published in 2002, described an 83-year-old man with symptoms similar to normal pressure hydrocephalus, with imaging revealing obstructive hydrocephalus due to a hyperdense lesion in the third ventricle.[
A fourth report published in 2016 described a 46-year-old woman with an incidental colloid cyst, initially asymptomatic, with planned intervention when she became symptomatic with headaches and cognitive deficits 3 years later.[
These five reports demonstrate that it is possible to have spontaneous resolution of a colloid cyst and suggest that conservative management is a viable approach to managing patients, particularly with asymptomatic colloid cysts identified incidentally. Here, we add to this fund of knowledge, demonstrating that without intervention, this tumor can remain stable for years and then begin to regress spontaneously. The cause of cyst initiation and regression is still incompletely understood. The previous reports suggest that cyst rupture may contribute to its resolution; however, other reports deny imaging findings suggestive of rupture but indeed show resolution. It is possible that rupture was missed, given the time spaced between imaging studies, or another mechanism of involution, still unknown, was responsible.
Some would argue that in this case, the patient presented with neurologic deficits and, therefore, cannot be classified as “asymptomatic.” On examination, the patient was consistently neurologically stable and remained that way throughout years of surveillance. He experienced chronic headaches, potentially caused by his ledipasvir/sofosbuvir treatment for hepatitis C.[
CONCLUSION
Colloid cysts are benign lesions, most commonly located within the third ventricle. They become symptomatic when cerebrospinal fluid (CSF) is occluded and intracranial pressure is raised. Fortunately, patients with symptomatic lesions can often be cured with surgical intervention with either cyst removal or shunting of the CSF. Uncertainty arises when patients are discovered to have colloid cysts incidentally; should the neurosurgeon intervene and remove the cyst or is a more conservative approach sufficient? This uncertainty is derived from our lack of understanding of these colloid cysts, their initiation, growth, and resolution. This case report demonstrates that colloid cysts can regress, which supports conservative management in patients who are asymptomatic at the discovery.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Annamalai G, Lindsay KW, Bhattacharya JJ. Spontaneous resolution of a colloid cyst of the third ventricle. Br J Radiol. 2008. 81: e20-2
2. Beaumont TL, Limbrick DD, Rich KM, Wippold FH, Dacey RG. Natural history of colloid cysts of the third ventricle. J Neurosurg. 2016. 125: 1420-30
3. Desai KI, Nadkarni TD, Muzumdar DP, Goel AH. Surgical management of colloid cyst of the third ventricle-a study of 105 cases. Surg Neurol. 2002. 57: 295-302
4. Gbejuade H, Plaha P, Porter D. Spontaneous regression of a third ventricle colloid cyst. Br J Neurosurg. 2011. 25: 655-7
5. Jeffree RL, Besser M. Colloid cyst of the third ventricle: A clinical review of 39 cases. J Clin Neurosci. 2001. 8: 328-31
6. Lagman C, Rai K, Chung LK, Nagasawa DT, Beckett JS, Tucker AM. Fatal colloid cysts: A systematic review. World Neurosurg. 2017. 107: 409-15
7. Little JR, MacCarty CS. Colloid cysts of the third ventricle. J Neurosurg. 1974. 40: 230-5
8. Motoyama Y, Hashimoto H, Ishida Y, Iida JI. Spontaneous rupture of a presumed colloid cyst of the third ventricle-case report. Neurol Med Chir (Tokyo). 2002. 42: 228-31
9. Mulcahy MJ, Chaganti J, Al-Khawaja D. The case of the disappearing colloid cyst. World Neurosurg. 2020. 135: 100-2
10. O’Neill AH, Gragnaniello C, Lai LT. Natural history of incidental colloid cysts of the third ventricle: A systematic review. J Clin Neurosci. 2018. 53: 122-6
11. Peeters SM, Daou B, Jabbour P, Ladoux A, Lahoud GA. Spontaneous regression of a third ventricle colloid cyst. World Neurosurg. 2016. 90: 704.e19-22
12. Ryder JW, Kleinschmidt-DeMasters BK, Keller TS. Sudden deterioration and death in patients with benign tumors of the third ventricle area. J Neurosurg. 1986. 64: 216-23
13. Tam E, Luetkemeyer AF, Mantry PS, Satapathy SK, Ghali P, Kang M. Ledipasvir/sofosbuvir for treatment of hepatitis C virus in sofosbuvir-experienced, NS5A treatment-naive patients: Findings from two randomized trials. Liver Int. 2018. 38: 1010-21

