

- Department of Neurosurgery, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
- Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
Correspondence Address:
Suryanarayanan Bhaskar
Department of Neurosurgery, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
DOI:10.25259/SNI_710_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nitin Kumar1, Jaskaran Singh Gosal1, Sarbesh Tiwari2, Mayank Garg1, Suryanarayanan Bhaskar1, Deepak Kumar Jha1. Craniovertebral junction anomaly with kissing carotids. 06-Nov-2020;11:377
How to cite this URL: Nitin Kumar1, Jaskaran Singh Gosal1, Sarbesh Tiwari2, Mayank Garg1, Suryanarayanan Bhaskar1, Deepak Kumar Jha1. Craniovertebral junction anomaly with kissing carotids. 06-Nov-2020;11:377. Available from: https://surgicalneurologyint.com/surgicalint-articles/10372/
Date of Submission
08-Oct-2020
Date of Acceptance
17-Oct-2020
Date of Web Publication
06-Nov-2020
Abstract
Background: “Kissing carotids” typically involves the lower C4-C6 retropharyngeal space. Here, we describe a case of “kissing carotids” observed at the C1-C2 level in conjunction with basilar invagination (BI).
Case Description: A 34-year-old-male presented with congenital atlantoaxial dislocation and BI. The initial surgical plan was for a transoral decompression (TOD). However, this approach was abandoned when the preoperative computed tomography angiography (CTA) documented “kissing carotids” lying anteriorly at the C1-C2 level.
Conclusion: Obtaining a CTA before performing a TOD for BI is essential to prevent an intraoperative catastrophic hemorrhage due to the laceration of “kissing carotids.”
Keywords: Atlantoaxial dislocation, Basilar invagination, Craniovertebral junction, Kissing carotids
INTRODUCTION
Kissing carotids has been described involving the retropharyngeal space, typically at lower cervical levels, C4-C6.[
CASE REPORT
A 34-year-old male presented with neck pain and a progressive spastic quadriparesis (3–4/5) of 3 years duration. The MR showed atlantoaxial dislocation (AAD) with severe compression of the spinal cord at the craniovertebral junction (CVJ) [
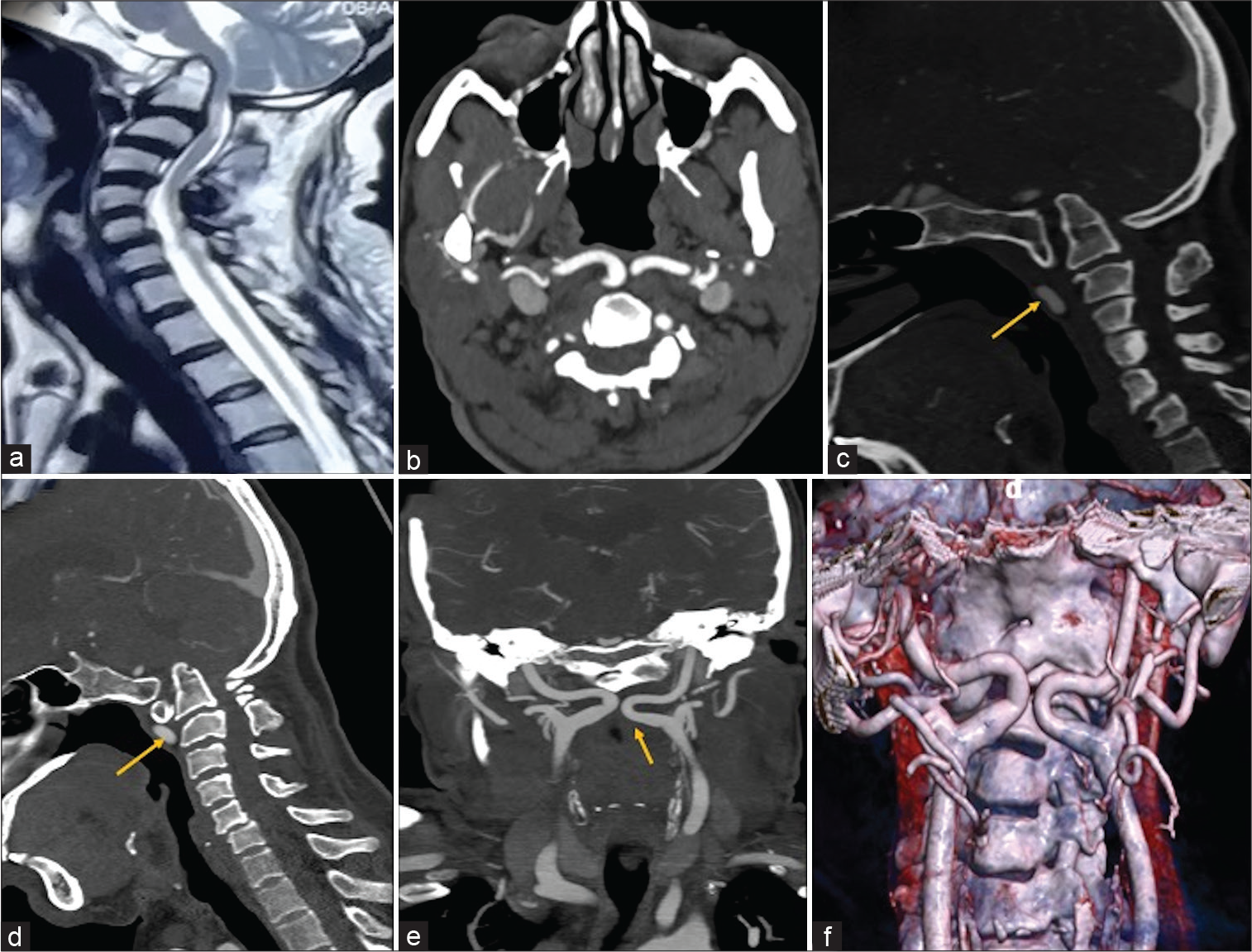
Figure 1:
(a) T2 sagittal MR craniovertebral junction showing the presence of BI with severe compression of the spinal cord. No evidence of Chiari or syrinx. The axial (b), sagittal (c and d), and coronal (e) source images of CT angiogram of neck vessels show an abnormal tortuous and retropharyngeal course of bilateral cervical internal carotid arteries, coming nearby at C1-2 level (yellow arrow). Note the atlantooccipital assimilation and basilar invagination. The volume rendering technique image (f) shows the proximity of the carotids in relation to C1-C2: “Kissing carotids.”
DISCUSSION
Kissing carotids have been described in the retropharyngeal space at lower cervical levels (C4-C6).[
CONCLUSION
Obtaining a CTA before performing a TOD for BI is indispensable to prevent the laceration of “kissing carotids.”
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chandak S, Mandal A, Singh A. Kissing carotids: An unusual cause of dysphagia in a healthy child. J Pediatr Neurosci. 2016. 11: 380-1
2. Windfuhr JP, Stow NW, Landis BN. Beware of kissing carotids. ANZ J Surg. 2010. 80: 668-9
3. Zafar M, Kiani A, Galiatsatos N, Rahmani MJ. Kissing carotids. Br J Hosp Med (Lond). 2020. 81: 2-3

