

- Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
- Stem Cell Unit, Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
- Department of Orthopaedics and Traumatology, Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
- Department of Anesthesiology and Intensive Care Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
- Department of Internal Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
Correspondence Address:
Ahmad Faried
Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia.
DOI:10.25259/SNI_828_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ahmad Faried1,2, Nucki Nursjamsi Hidajat2,3, Ali Budi Harsono2, Gezy Weita Giwangkancana4, Yovita Hartantri5, Akhmad Imron1, Muhammad Zafrullah Arifin1. Delayed definitive treatment of life-threatening neurosurgery patient with suspected coronavirus disease 2019 infection in the midst of pandemic: Report of two cases. 13-Jan-2021;12:18
How to cite this URL: Ahmad Faried1,2, Nucki Nursjamsi Hidajat2,3, Ali Budi Harsono2, Gezy Weita Giwangkancana4, Yovita Hartantri5, Akhmad Imron1, Muhammad Zafrullah Arifin1. Delayed definitive treatment of life-threatening neurosurgery patient with suspected coronavirus disease 2019 infection in the midst of pandemic: Report of two cases. 13-Jan-2021;12:18. Available from: https://surgicalneurologyint.com/surgicalint-articles/10521/
Date of Submission
17-Nov-2020
Date of Acceptance
17-Dec-2020
Date of Web Publication
13-Jan-2021
Abstract
Background: Coronavirus disease 2019 (COVID-19) pandemic has affected global health system; in the context of the COVID-19 pandemic, both surgeon and anesthesiologist often dealt with emergency situation, optimal timing of surgery and safety protocol in hospital setting must be implemented with many facets for both patients and health-care providers.
Case Description: We reported two cases. Case#1 - A 16-year-old male was referred to our hospital, due to a decreased of consciousness following a motor vehicle accident. Head CT scan revealed an epidural hemorrhage on the left temporoparietal. The patient was suspected for having COVID-19 from the reactivity of his serum against SARS-CoV-2 antigen. Procedures for the confirmation of COVID-19 and surgical preparation caused 12 h delayed from the admission. Nevertheless, the patient was deteriorated clinically before he was transported to the operating room and died after 6 cycles of cardiopulmonary resuscitation. Case#2 - A 25-year-old male was referred to RSHS, due to a decreased of consciousness, diagnosed as bilateral proximal shunt exposed with suspected COVID-19; delay occurred due to unavailability of negative pressure intensive unit for postoperative care. This caused 5760 h (4 days) delayed for bilateral shunt removal and temporary extraventricular drainage.
Conclusion: Optimal timing of surgery, a good safety, and health protocol during pandemic in emergency setting are an obligation to protect health providers and patients. A decision-making plan must be organized precisely to maintain alertness, achieve the highest possible standard of care, and outcome in emergency surgical cases. Lack of monitoring must be abated to avoid fatality for patient, especially in emergency surgery setting.
Keywords: Definitive treatment, Neurosurgery, Suspected Coronavirus disease 2019 patients
INTRODUCTION
Coronavirus disease 2019 (COVID-19) pandemic has affected global health-care system.[
CASE PRESENTATION
Characteristics of patients with suspected COVID-19 in our emergency unit
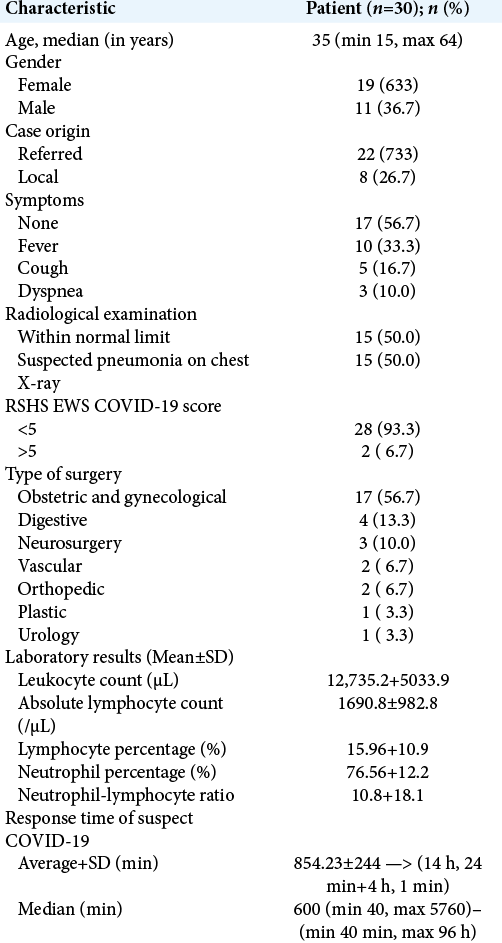
The initial screening for potential COVID-19 infection was conducted by the emerging and reemerging infectious disease team (PINERE). Patients were screened for COVID-19 before surgery by PINERE using RSHS modified early warning score (RSHS EWS consists of standard questionnaire, laboratory, and radiology). Suspected COVID-19 was declared based on RSHS EWS values ≥5. Between May 1, 2020, and June 31, 2020, 166 patients were consulted to our unit with indications for emergency surgical procedures, with 30 subjects (18.1%) who were declared as patients with suspected COVID-19. The median age was 35 years old (YO) [the youngest 15 YO and the oldest 64 YO]. Most cases were female (n = 19; 63.3%) with obstetric as the most common group (n = 17; 56.7%). Majority of subjects were referred from other cities (n = 22; 73.3%) and only 8 patients (26.7%) came from our city. We observed that more than a half of patients were came without symptoms of COVID-19 (n = 17; 56.7%); only 10 patients (33.3%) with fever, 5 patients (16.7%) with cough, and 3 patients (10%) with dyspnea. Radiological examination shown half of patients (n = 15; 50%) suspected pneumonia on their chest X-ray. RSHS EWS values ≥5 for COVID-19 were only 2 patients (6.7%). The mean value of leukocyte was 12,735.2 ± 5033.9/ul, absolute lymphocyte was 1690.8 ± 982.8/ul, lymphocyte was 15.96 ± 10.9%, neutrophil was 76.56 ± 12.2%, and neutrophil-lymphocyte ratio was 10.8 ± 18.1. The average response time of suspected COVID-19 patients from arrival to surgery was 14 h 24 min ± 4 h 1 min with the median response time which was 10 h (min 40 min and max 96 h) [
Death case report #1: Medical history and physical examination
A 16 YO boy who was riding a motorcycle without helmet was hit by another motorcycle and suffered a moderate traumatic brain injury (TBI), was found unconscious and admitted to our center. Primary survey shown a clear airway with C-spine control, body temperature of 37.3°C, heart rate 100×/m, respiratory rate 22×/m, blood pressure 120/80 mmHg, and Glasgow Coma Scale (GCS) of 10 (E3M5V2). Cardiorespiratory examination showed no abnormalities. Pupils were round, isochoric with diameter of 3 mm on both eyes, normal pupillary reflex, and no motor weakness on both extremities. However, we found a hematoma on his left temporal.
Laboratory findings
We conducted routine laboratory examination and rapid antibody against SARS-CoV-2 for routine screening during pandemic. All hematology parameters were normal except for a slight leukocytosis (leukocyte 17,340/μL). However, the patient was found to be reactive for SARS-CoV-2 antigen at 5 h from admission.
Diagnostic imaging
Patient’s chest x-ray within normal limits [

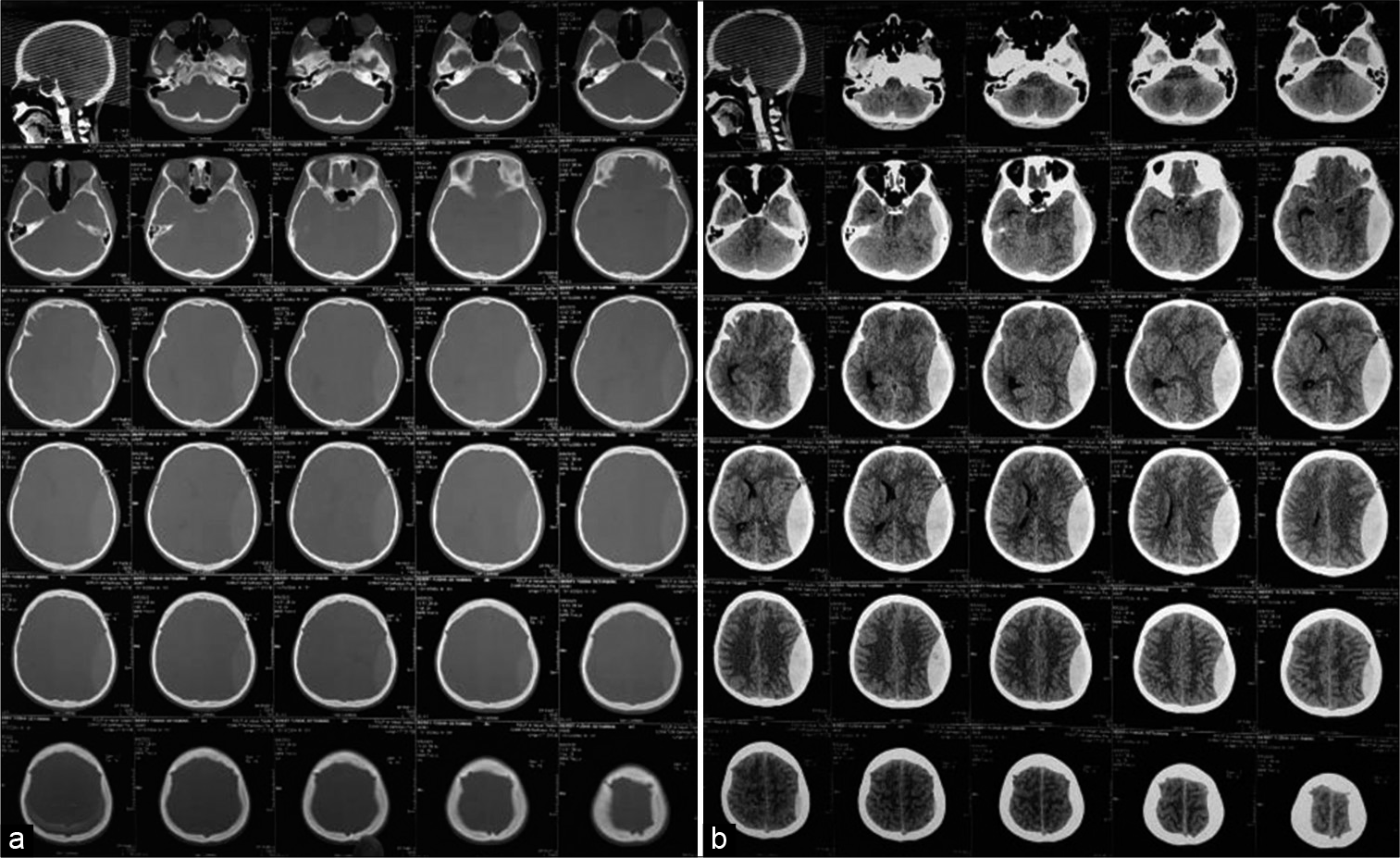
Figure 2:
Following of the noncontrast head CT scan showed the presence soft-tissue swelling on the left temporal without bone fracture (a); compressed sulci, gyri, Sylvian fissure, and ventricles, then a massive biconvex hyperdense mass on the left temporoparietal region (±40 cc) with midline shift >5 mm (b).
Treatment
We planned an emergency craniotomy. However, surgery to evacuate EDH was delayed due to health and safety protocols for patients suspected with COVID-19. As soon as the suspected COVID-19 diagnosis was established, the patient was moved to a separate COVID-19 isolation room with less neurological monitoring. There was no burr hole equipment in our emergency room for COVID-19 patients. Every patient suspected or confirmed with COVID-19 was consulted to PINERE team in infection and operating room (OR) needs more time to be prepared for an infectious patient. This caused 12 h delayed from the admission. Nevertheless, the patient was deteriorated clinically before he was transported to the OR and died after 6 cycles of cardiopulmonary resuscitation.
Dead case report #2: Medical history and physical examination
A 25 YO male, 3 days before admission, the patient looked drowsy and difficult to be awaken; the complaint preceded with cough, shortness of breath, and fever. His family complained of exposed shunt since a month ago. Primary survey was within normal limit, body temperature of 38.9°C, heart rate 118×/m, respiratory rate 26×/m, blood pressure 130/80 mmHg, and GCS of 7 with tracheostomy (E2M5Vtc); on respiratory examination, crackles were heard in both side of the lungs, but O2 saturation was still within the range of 96–98%. Pupils were round, an isochore with 3/5 mm in diameter, absent of pupillary reflexes on the left side, and at bilateral Kocher point, the proximal part of the shunt was found exposed at both parietal regions.
Laboratory findings
We conducted laboratory examination and the antibody test against SARS-CoV-2 for screening. The result was found to be reactive for SARS-CoV-2 antigen after 1 day since the admission; hematology parameters were within normal limits.
Diagnostic imaging
The chest X-ray showed homogenous radio-opaque areas in bilateral lung fields suggestive as bilateral pneumonia [
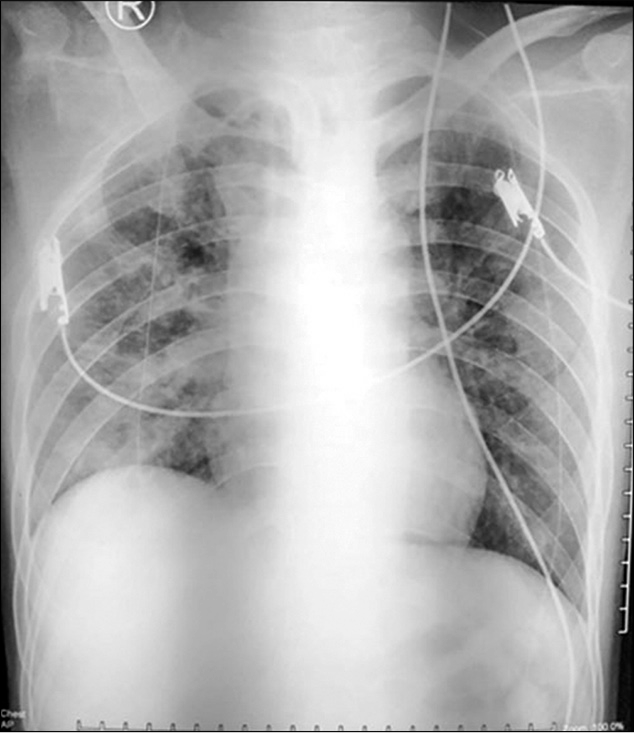
Treatment
As soon as the suspected COVID-19 diagnosis was established, the patient was treated in emergency COVID-19 isolation room. However, surgery to remove the both shunt tubes was delayed due to health and safety protocols. After consulted to PINERE team and OR ready for surgery, another delay occurred due to the full capacity of the COVID ICU for the postoperative care. This caused 5760 h or 4 days delayed from the admission administration to, in this case, bilateral shunt removal and temporary EVD.
DISCUSSION
A total of 30 patients (18.1%) from 166 patients were consulted to our emergency unit with consideration as a suspected COVID-19 patient (May–June 2020); only one patient had reverse transcription polymerase chain reaction (RT-PCR) (+). Most of the cases were female (63.3%) and needed emergency cesarean (SC) section. Female predominant for emergency surgery and suspected to have COVID-19 is similar to previous studies in the US and Italy, since SC is the most common surgery done in all countries including Indonesia.[
Death case report #1
TBI is one of the leading cause of death in young people, especially in the Southeast Asia.[
There were several reasons for devastating outcome in this patient. First, during the early months of the pandemic, our hospital was not equipped with on-site PCR equipment with COVID-19 and since the previous studies have shown that COVID-19 has a typical pneumonia-like symptom without a specific clinical characteristic, it was difficult to diagnose. The only available kit for screening on that period was a rapid antibody test which on previous reports shows promising sensitivity and specificity for SARS-CoV-2 active infection although later studies rebutted those results; we used SD Biosensor SARS-CoV-2 antibodies kit for the rapid test and yielded results within 15 min.[
After the patient was transferred to isolation room for reactive result in COVID-19 antibody test, there was lack of neurological monitoring. Neurological monitoring was recommended to be performed at least once every hour.[
Moreover, there was no emergency burr hole equipment in the isolation room of the emergency unit prepared for COVID-19 patients, so the life-saving emergency procedure was not performed. Unfortunately, the patient died in the isolation room of our emergency ward after waiting for 12.5 h without definitive treatment, in this case, craniotomy.
Death case report #2
The Vp shunt exposure on the scalp is a serious complication; the common complications were exposure of the shunt 23.3% (13.3% exposed shunt reservoir and 10% exposed distal catheter).[
CONCLUSION
Optimal timing of surgery, a good safety, and health protocol during pandemic in emergency setting are an obligation to protect health providers and patients. A decision-making plan must be organized precisely to maintain alertness, achieve the highest possible standard of care, and outcome in emergency surgical cases. Hospital management and infectious disease team must make strategic protocol to balance staff safety, effective time management, especially in time-dependent neurosurgical patient, and ultimately best interest and outcome of the patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Indonesian Ministry of Research and Technology (National Agency for Research and Innovation) in collaboration with the Institute of Fund Management for Education No. 160/M/ KPT/2020 for COVID-19.
Conflicts of interest
There are no conflicts of interest.
References
1. Al-Jabir A, Kerwan A, Nicola M, Alsafi Z, Khan M, Sohrabi C. Impact of the Coronavirus (COVID-19) pandemic on surgical practice-Part 2 (surgical prioritisation). Int J Surg. 2020. 79: 233-48
2. Al-Muharraqi MA. Testing recommendation for COVID-19 (SARS-CoV-2) in patients planned for surgery-continuing the service and suppressing the pandemic. Br J Oral Maxillofac Surg. 2020. 58: 503-5
3. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW. Surgical management of acute epidural hematomas. Neurosurgery. 2006. 58: S7-15
4. Bulters D, Belli A. A prospective study of the time to evacuate acute subdural and extradural haematomas. Anaesthesia. 2009. 64: 277-81
5. Cenzato M, DiMeco F, Fontanella M, Locatelli D, Servadei F. Editorial, Neurosurgery in the storm of COVID-19: Suggestions from the Lombardy region. Italy (ex malo bonum). J Neurosurg. 2020. 10: 1-2
6. Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC, Punchak M. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2019. 130: 1080-97
7. Doglietto F, Vezzoli M, Gheza F, Lussardi GL, Domenicucci M, Vecchiarelli L. Factors associated with surgical mortality and complications among patients with and without Coronavirus disease 2019 (COVID-19) in Italy. JAMA Surg. 2020. 155: 1-14
8. Geeraerts T, Velly L, Abdennour L, Asehnoune K, Audibert G, Bouzat P. Management of severe traumatic brain injury (first 24hours). Anaesth Crit Care Pain Med. 2018. 37: 171-86
9. Hamdan AR. Ventriculoperitoneal shunt complications: A local study at Qena University Hospital: A retrospective study. Egypt J Neurosurg. 2018. 33: 8
10. He J, Guo Y, Mao R, Zhang J. Proportion of asymptomatic Coronavirus disease 2019: A systematic review and meta-analysis. J Med Virol. 2020. p.
11. Hecht N, Wessels L, Werft FO, Schneider UC, Czabanka M, Vajkoczy P. Need for ensuring care for neuro-emergencies-lessons learned from the COVID-19 pandemic. Acta Neurochir (Wien). 2020. 162: 1795-801
12. Hogan A. COVID-19 and emergency surgery. Br J Surg. 2020. 107: e180
13. Jangra K, Paliwal S, Tripathi M. COVID-19 and neurosurgery: Time for triage. J Neuroanaesthesiol Crit Care. 2020. 7: 67-9
14. Kast J, Duong D, Nowzari F, Chadduck WM, Schiff SJ. Time-related patterns of ventricular shunt failure. Childs Nerv Syst. 1994. 10: 524-8
15. Khairat A, Waseem M.editors. Epidural hematoma. Stat Pearls. Treasure Island, FL: Stat Pearls Publishing; 2020. p.
16. Maugeri R, Anderson DG, Graziano F, Meccio F, Visocchi M, Iacopino DG. Conservative vs. surgical management of post-traumatic epidural hematoma: A Case and review of literature. Am J Case Rep. 2015. 16: 811-7
17. Morris M, Pierce A, Carlisle B, Vining B, Dobyns J. Pre-operative COVID-19 testing and decolonization. Am J Surg. 2020. 220: 558-60
18. Niryana W, Teddy H, Golden N, Widyadharma E. Related risk factors and outcome of patients post trepanation epidural hematoma evacuation. Biomed Pharmacol J. 2017. 10: 717-23
19. Reddy GK, Bollam P, Caldito G. Long-term outcomes of ventriculoperitoneal shunt surgery in patients with hydrocephalus. World Neurosurg. 2014. 81: 404-10
20. STANDARD Q for Coronavirus Disease 2019 (COVID-19) IgM/IgG Duo. Available from: http://www.sdbiosensor.com/xe/product/7662 [Last accessed on 16 Nov 2020].
21. Sergides IG, Whiting G, Howarth S, Hutchinson PJ. Is the recommended target of 4 hours from head injury to emergency craniotomy achievable?. Br J Neurosurg. 2006. 20: 301-5
22. Tenenbein P, Riazi S, Johnstone J, Keshavjee S, Karkouti K. The case for routine screening for SARS-CoV-2 before surgery. Can J Anaesth. 2020. 67: 1315-20
23. COVID-19 CONTINGENCY Procedure Guidelines. Available from: https://www.unmc.edu/coronavirus [Last accessed on 16 Nov 2020].
24. Yehia BR, Winegar A, Fogel R, Fakih M, Ottenbacher A, Jesser C. Association of race with mortality among patients hospitalized with Coronavirus disease 2019 (COVID-19) at 92 US hospitals. JAMA Netw Open. 2020. 3: e2018039

