

- Department of Neurosurgery, University of Kansas Medical Center, Kansas City, KS, USA
Correspondence Address:
Kyle A. Smith
Department of Neurosurgery, University of Kansas Medical Center, Kansas City, KS, USA
DOI:10.4103/2152-7806.173313
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Smith KA, Crabtree K, Chamoun R. Delayed intraventricular metastasis of clival chordoma. Surg Neurol Int 05-Jan-2016;7:3
How to cite this URL: Smith KA, Crabtree K, Chamoun R. Delayed intraventricular metastasis of clival chordoma. Surg Neurol Int 05-Jan-2016;7:3. Available from: http://surgicalneurologyint.com/surgicalint_articles/delayed-intraventricular-metastasis-of-clival-chordoma/
Sir,
Intracranial chordomas are typically clival and extradural in location, yet these tumors can obviously invade the dura. However, primary intradural chordomas without local extension is a rare event with approximately 47 cases reported in literature. Furthermore, all intradural chordoma reports appear to be extraventricular in location.[
We present this unique case of an intraventricular recurrence of a clival chordoma and successful use of neuroendoscopy to explore and resect the tumor. A 60-year-old male, with a history of clival chordoma resection and adjuvant radiation nearly 10 years prior, presented with an intraventricular lesion on magnetic resonance imaging (MRI) obtained for stroke workup of the left sided weakness. Physical examination showed right third nerve palsy, left facial droop, and left sided weakness. MRI demonstrated an intraventricular enhancing lesion within the right lateral ventricle [Figure
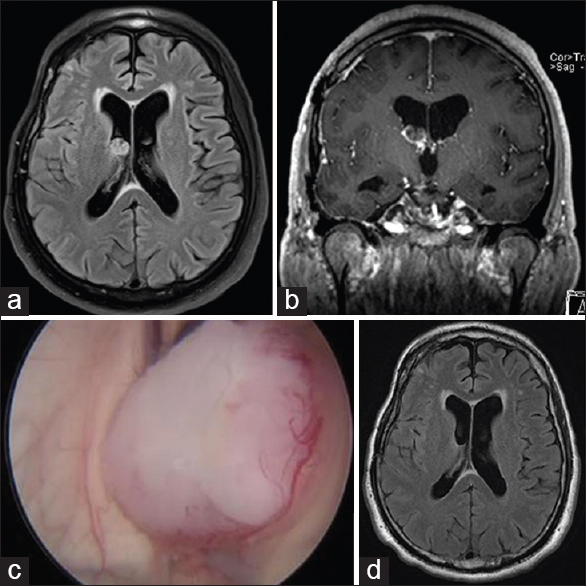
Figure 1
(a and b) Preoperative magnetic resonance imaging demonstrates an enhancing lesion, approximately 1.5 cm × 1.0 cm, along the ependymal surface within the right lateral ventricle caudothalamic notch. (c) Intraoperative view of intraventricular lesion via endoscope prior to resection. (d) Postoperative magnetic resonance imaging demonstrates gross total resection
This case illustrates a unique occurrence of intraventricular recurrence of clival chordoma approximately 10 years after initial resection with good result via an endoscopic technique. Prior reports have typically focused on intradural, extraventricular metastases. A solitary intraventricular chordoma neoplasm is a rare, interesting event. Furthermore, neuroendoscopy is a useful technique for tumor resection and proves viable in the resection of chordomas.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. AlOtaibi F, Guiot MC, Muanza T, Di Maio S. Giant petroclival primary intradural chordoma: Case report and systematic review of the literature. J Neurol Surg Rep. 2014. 75: e160-9
2. Ito E, Saito K, Nagatani T, Ishiyama J, Terada K, Yoshida M. Intradural cranial chordoma. World Neurosurg. 2010. 73: 194-7

