

- Department of Neurosurgery, Edelweiss Hospital, Bandung, Jawa Barat, Indonesia.
- Department of Pediatrics, Edelweiss Hospital, Bandung, Jawa Barat, Indonesia.
- Department of Clinical Pathology, Edelweiss Hospital, Bandung, Jawa Barat, Indonesia.
Correspondence Address:
Ahmad Faried
Department of Clinical Pathology, Edelweiss Hospital, Bandung, Jawa Barat, Indonesia.
DOI:10.25259/SNI_932_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ahmad Faried1, Akhmad Imron1, Almira Aliyannissa2, Dini Indrawati3. Delayed subaponeurotic fluid collection on an infant’s head: Underreported case and review of the literature. 17-May-2021;12:233
How to cite this URL: Ahmad Faried1, Akhmad Imron1, Almira Aliyannissa2, Dini Indrawati3. Delayed subaponeurotic fluid collection on an infant’s head: Underreported case and review of the literature. 17-May-2021;12:233. Available from: https://surgicalneurologyint.com/surgicalint-articles/10807/
Date of Submission
22-Dec-2020
Date of Acceptance
01-Apr-2021
Date of Web Publication
17-May-2021
Abstract
Background: Delayed subaponeurotic fluid collection (DSFC) is a relatively uncommon problem, probably under reported soft swelling in the scalp which usually develops in infancy that occurs weeks to months after birth. Although the exact etiology remains unclear, several theories have been postulated such as (i) cerebrospinal fluids (CSF) leak from microfractures of the skull and (ii) disrupted lymphatic drainage, gradually liquefying subaponeurotic bleeding. Here, we reported typical clinical findings of DSFC and analysis of the fluid aspirate from our patient. To the best of our knowledge, this is the first case reported from Asia, particularly from Indonesia.
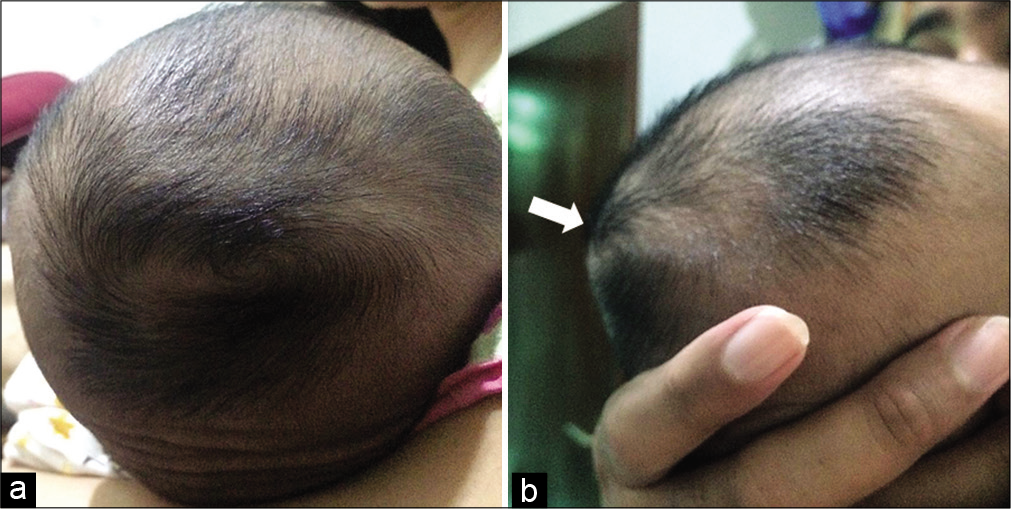
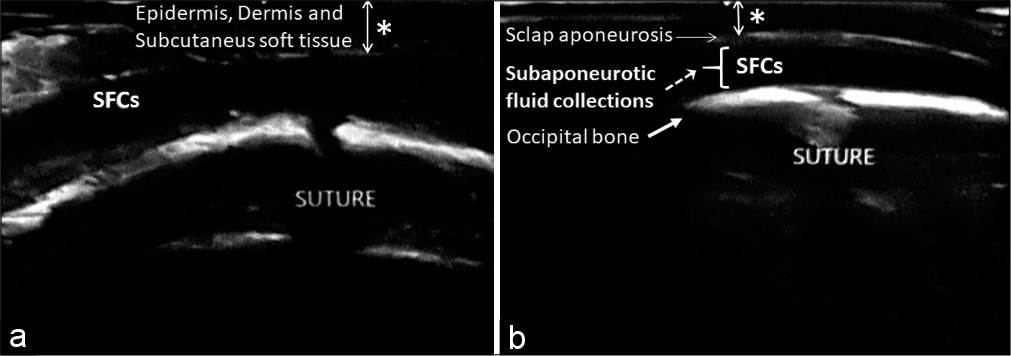
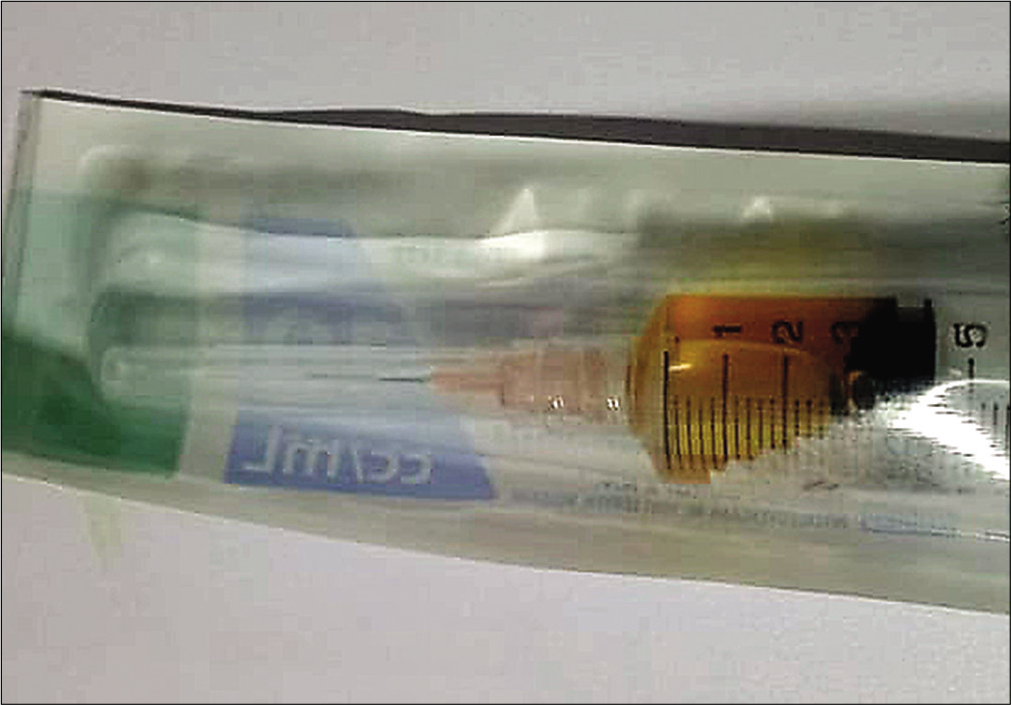
Case Description: A healthy 2-month-old girl infant presented with 2 weeks history of occipital painless fluctuant scalp mass with no swelling. She was born at term from a nulliparous mother; by emergency cesarean delivery following failed induction of labor. There was no history of scalp injury at birth nor recent head trauma; ultrasonography showed translucent fluid in subaponeurotic or subgaleal space. The fluid collection was noted to be fluctuant, free-flowing across suture lines, without discoloration or bruising; when placed supine, the fluid collected at her midocciput. A diagnostic tap confirmed the presence of serosanguinous CSF led to a diagnosis of DSFC.
Conclusion: Herein, we reported the first DSFC case from Indonesia. With no previous experience of the condition, a definitive diagnosis was possible through a very carefully physical examination and history taking, along with a good communication among the neurosurgeon, pediatrician, and the clinical pathologist.
Keywords: Delayed subaponeurotic fluid collection, Infancy, Underreported case
INTRODUCTION
Acquired scalp swelling in neonates and infants is a common condition. Several diagnostic considerations include subaponeurotic or subgaleal hemorrhage, cephalhematoma, caput succedaneum, and delayed subaponeurotic fluid collections (DSFCs).[
CASE PRESENTATION
A healthy 2-month-old girl infant was referred to our hospital by her anxious parents, presented with 2 weeks history of occipital painless fluctuant scalp mass with no swelling and suspected of having a subaponeurotic or subgaleal hemorrhage. She was initially admitted to the Outpatient Pediatric Clinic, Edelweiss Hospital, Bandung, West Java, Indonesia, before being consulted to the Department of Neurosurgery. She was born at term from a primigravida mother, birth was by emergency cesarean section following failed induction of labor with no history of fetal scalp electrode usage; scalp injury at birth nor recent head trauma. The fluid collection was noted to be fluctuant, free-flowing across the suture lines, without discoloration or bruising skin and when supine, the fluid collected at his midocciput [
DISCUSSION
DSFCs are recently described clinical entity within only 62 case reports in medical literatures up to date (searching PubMed using the search term “DSFCs”). All 16 articles were reviewed by the first author and data were then extracted). There were 15 cases reported from the United States of America,[
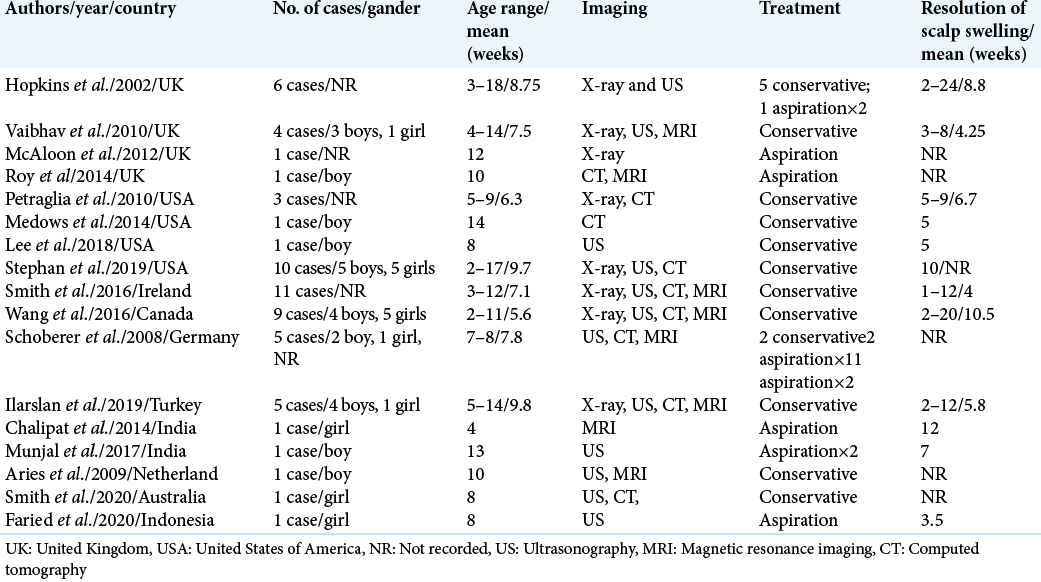
Hopkins et al. reported the first six cases of DSFCs that managed conservatively and one case was managed by a needle aspiration of the collection on two occasions when serosanguinous fluid was aspirated ×2 after diagnosis.[
All patients have no recent head trauma or illness. Growth, development, and behavior are normal.[
DSFCs is self-limiting condition that might masquerades a nonaccidental injury and should not prompt work-up in an otherwise clinically well infant.[
CONCLUSION
The diagnosis of DSFCs is primarily clinical examination and history taking, along with a good communication among colleagues; current gold standard treatment remains conservative.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Dr. Ahmad Faried supported by Grants-in-Aids from Universitas Padjadjaran, Bandung, Indonesia.
Conflicts of interest
There are no conflicts of interest.
References
1. Aries MJ, van Dam SW, Hoving EW, Brouwer OF. An infant with a cranial swelling: Sub-aponeurotic fluid collection. Ned Tijdschr Geneeskd. 2009. 153: A713
2. Chalipat S, Karambelkar G, Dhobale V, Agarkhedkar SR, Jadhav R. Sub-aponeurotic fluid collection: A rare cause of scalp swelling in infancy. Pediatr Oncall J. 2014. 11: 85
3. Hopkins RE, Inward C, Chambers T, Grier D. Sub-aponeurotic fluid collections in infancy. Clin Radiol. 2002. 57: 114-6
4. Ilarslan NE, Gunay F, Kaynak SS, Ucan B, Fitoz OS, Ince E. A rare cause of scalp swelling in infancy: Delayed subaponeurotic fluid collections in five cases. Childs Nerv Syst. 2019. 35: 875-8
5. Lee JJ, Wenger TL. Delayed subaponeurotic fluid collections of infancy. J Pediatr. 2018. 197: 310-0
6. McAloon J, McCabe J. An unusual swelling on an infant’s head. Arch Dis Child Fetal Neonatal Ed. 2013. 98: 410
7. Medows M, Mohammad Nijres B. Delayed subaponeurotic (subgaleal) fluid collection. BMJ Case Rep. 2014. 2014: bcr2013203457
8. Munjal S, Kumar S. Subaponeurotic cerebrospinal fluid collection in an infant. J Pediatr Neurosci. 2017. 12: 271-2
9. Petraglia AL, Moravan MJ, Marky AH, Silberstein HJ. Delayed sub-aponeurotic fluid collections in infancy: Three cases and a review of the literature. Surg Neurol Int. 2010. 1: 34
10. Roy HA, Magdum S. Sub-aponeurotic fluid collection in a neonate associated with fetal scalp electrode monitoring: A brief communication. Eur J Obstet Gynecol Reprod Biol. 2014. 181: 343-4
11. Schoberer A, Yagmur E, Boltshauser E, Korinth M, Niggemann P, Häusler M. Sub-aponeurotic fluid collections: A delayed-onset self-limiting cerebrospinal fluid fistula in young infants. Eur J Paediatr Neurol. 2008. 12: 401-3
12. Smith A, Kandamany N, Okafor I, Robinson I, Foran A, McNamara R. Delayed infant subaponeurotic (subgaleal) fluid collections: A case series of 11 infants. J Emerg Med. 2016. 50: 881-6
13. Smith B. Delayed subaponeurotic fluid collection of infancy. J Paediatr Child Health. 2020. 2020: 15245
14. Stephan AM, Feldman KW, Otjen JP, Metz JB. Delayed subaponeurotic fluid collections: A benign cause of scalp swelling in infancy. Pediatr Emerg Care. 2019. 2019: 1720
15. Vaibhav A, Smith R, Millman G, Cooper J, Dwyer J. Subaponeurotic or subgaleal fluid collections in infancy: An unusual but distinct cause of scalp swelling in infancy. BMJ Case Rep. 2010. 2010: bcr0420102915
16. Wang S, Drake J, Kulkarni AV. Management and outcome of spontaneous subaponeurotic fluid collections in infants: The Hospital for Sick Children experience and review of the literature. J Neurosurg Pediatr. 2016. 18: 442-7
17. Worthen M, Leonard TH, Blair TR, Gupta N. Experiences of parents caring for infants with rare scalp mass as identified through a disease-specific blog. J Am Board Fam Med. 2015. 28: 750-8

