

- Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
Correspondence Address:
Satoshi Tsutsumi, Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
DOI:10.25259/SNI_760_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Satoshi Tsutsumi, Natsuki Sugiyama, Hideaki Ueno, Hisato Ishii. Does diploic venous flow drain extracranially in the pterional area? A magnetic resonance imaging study. 16-Sep-2022;13:425
How to cite this URL: Satoshi Tsutsumi, Natsuki Sugiyama, Hideaki Ueno, Hisato Ishii. Does diploic venous flow drain extracranially in the pterional area? A magnetic resonance imaging study. 16-Sep-2022;13:425. Available from: https://surgicalneurologyint.com/surgicalint-articles/11865/
Date of Submission
20-Aug-2022
Date of Acceptance
31-Aug-2022
Date of Web Publication
16-Sep-2022
Abstract
Background: To the best of our knowledge, no study using neuroimaging modalities has documented calvarial diploic veins (DVs) connected to the extracranial sites. This study aimed to characterize them using magnetic resonance imaging (MRI).
Methods: A total of 88 patients underwent thin-sliced contrast MRI. In addition, the DVs coursing through the pterional area were observed on three injected cadaver heads.
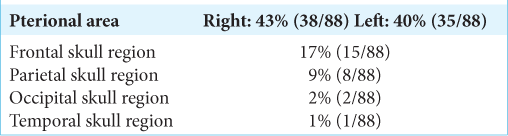
Results: On postcontrast MRI, the DVs of the pterional area directly drained into the temporalis muscle or supplied branches coursing into the muscle in 43% on the right side and 40% on the left. The DVs and their branches were highly variable in diameter and number. In 9% of cases, the DV of the pterional area was found to drain into an extracranial site and connected to large venous channels distributed in the temporalis muscle. Furthermore, in 17% of cases, the DVs drained into the extracranial sites in the frontal skull region, followed by 9% in the parietal, 2% in the occipital, and 1% in the temporal regions. The DVs coursed superficially in the pterional area on both sides of all three cadaver heads. On one side, the DV in the area was open to an extracranial site.
Conclusion: Part of the diploic venous flow drains extracranially in the pterional area. This area may provide an important interface between the calvarial DVs and the extracranial venous system.
Keywords: Diploic vein, Extracranial bypass, Magnetic resonance imaging, Pterion
INTRODUCTION
Diploic veins (DVs) are distinct venous channels formed in the calvarial diploe and are thought to show ontogenetic changes.[
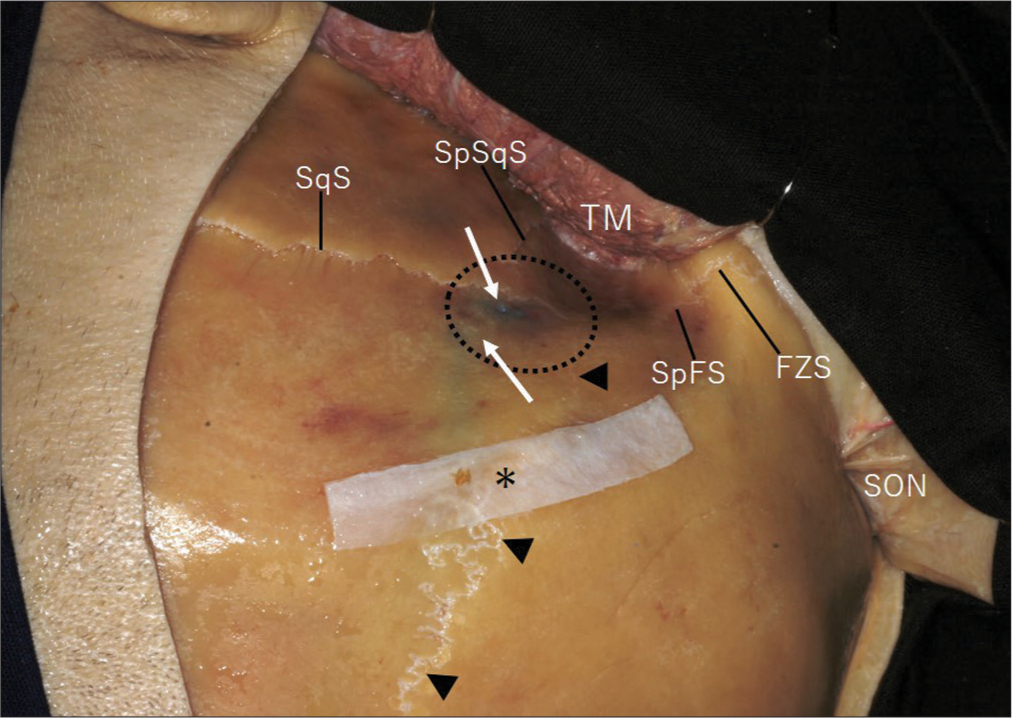
Figure 1:
A cadaver head, left side, showing reflection of the scalp flap and temporalis muscle for performing a frontotemporal craniotomy. The pterional area (within dashed circle) is formed by confluence of the coronal (arrowheads), squamosal (SqS), sphenofrontal (SpFS), and sphenosquamosal (SpSqS) sutures. FZS: Frontozygomatic suture; SON: Supraorbital nerve; TM: Temporalis muscle; Arrows: Diploic veins; Asterisk: Part of the fascia of temporalis muscle attached to the linea temporalis.
To the best of our knowledge, no study has yet used neuroimaging modalities for exploring calvarial DVs with extracranial courses. Therefore, this study aimed to characterize these veins using contrast-enhanced magnetic resonance imaging (MRI).
MATERIALS AND METHODS
This retrospective study included 88 outpatients who underwent MRI at the Medical Satellite Yaesu Clinic between April 2010 and October 2015. These patients presented with headache, dizziness, tinnitus, hearing loss, sensory disturbances, and focal seizures. Patients with the previous traumatic brain injury or skull fractures were excluded from the study. The study population consisted of 44 men and 44 women aged 50.4 ± 16.4 years (mean ± standard deviation; range, 13–78 years). Initial examinations using axial T1- and T2-weighted, T2 gradient echo, fluid-attenuated inversion recovery, and diffusion-weighted imaging confirmed that none of the patients had signs of pathological conditions in the scalp, skull, or intracranial dural sinuses. Subsequently, the patients underwent volumetric imaging examination with intravenous gadolinium infusion (0.1 mmol/kg) in the axial, coronal, and sagittal planes, involving the entire cranial vault. The following parameters were adopted: repetition time, 4.1 ms; echo time, 1.92 ms; slice thickness, 1 mm; interslice gap, 0 mm; matrix, 320 × 320; field of view, 250 mm; flip angle, 13°; and scan duration, 7 min 25 s. All imaging sequences were performed using a 3.0-T MRI scanner (Achieva R2.6; Philips Medical Systems, Best, The Netherlands). Imaging data were transferred to a workstation (Virtual Place Lexus 64, 64th edition; AZE, Tokyo, Japan) and independently analyzed by two authors (S.T. and H.I.). The DVs connected to the extracranial sites were assessed in the pterional and supratentorial calvarial convexity areas involving the frontal, parietal, occipital, and temporal skull regions. Due to the low detection performance of the DVs that were confirmed during the preliminary observations, postcontrast axial images were not used for analysis.
Furthermore, the DVs coursing in the pterional area were assessed on six sides of three cadaver heads. Before dissection, the internal jugular veins were injected bilaterally with blue silicone. Then, a scalp incision was made conforming with a conventional frontotemporal craniotomy. The scalp flap and temporalis muscle were reflected en bloc to observe the DVs in blue through the outer table. Dissections were performed by one of the authors (S.T.) at the Department of Neurological Surgery, University of Florida, Gainesville, FL, USA.
The study was conducted in accordance with the guidelines for human research of our institution and those of the Medical Satellite Yaesu Clinic. The written informed consent was obtained from all the patients before their participation in the study.
RESULTS
Examinations using contrast-enhanced MRI
The DVs draining into the extracranial sites were heterogeneously distributed over the skull. These DVs were most frequently identified in the pterional area and were found in 38 of 88 patients (43%) on the right side and 35 (40%) on the left side. These DVs were found to drain directly into the temporalis muscle or supply extracranial branches coursing into the muscle [
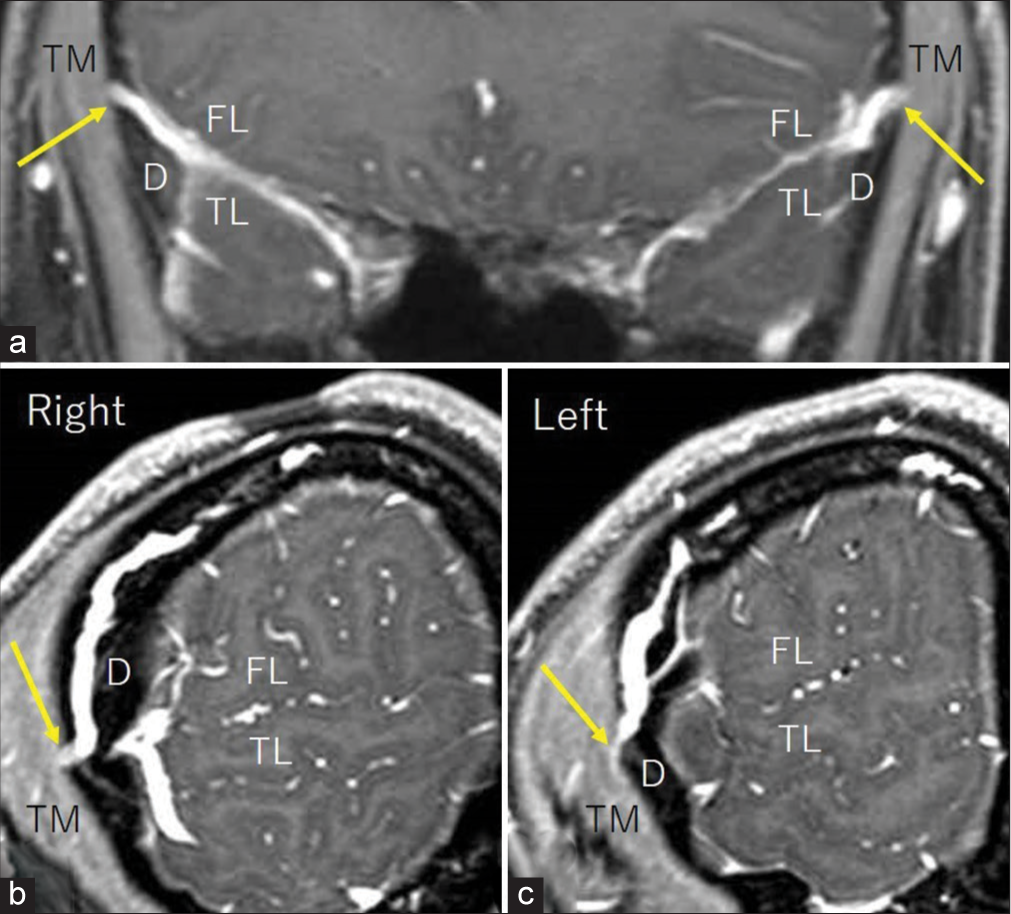
Figure 2:
Postcontrast coronal (a) and sagittal (b and c) T1-weighted magnetic resonance images at the corresponding levels showing diploic veins of the pterional area directly draining into the temporalis muscle (a and b, arrow) or supplying a branch coursing into the muscle (a and c, arrow). D: Diploe; FL: Frontal lobe; TL: Temporal lobe; TM: Temporalis muscle.
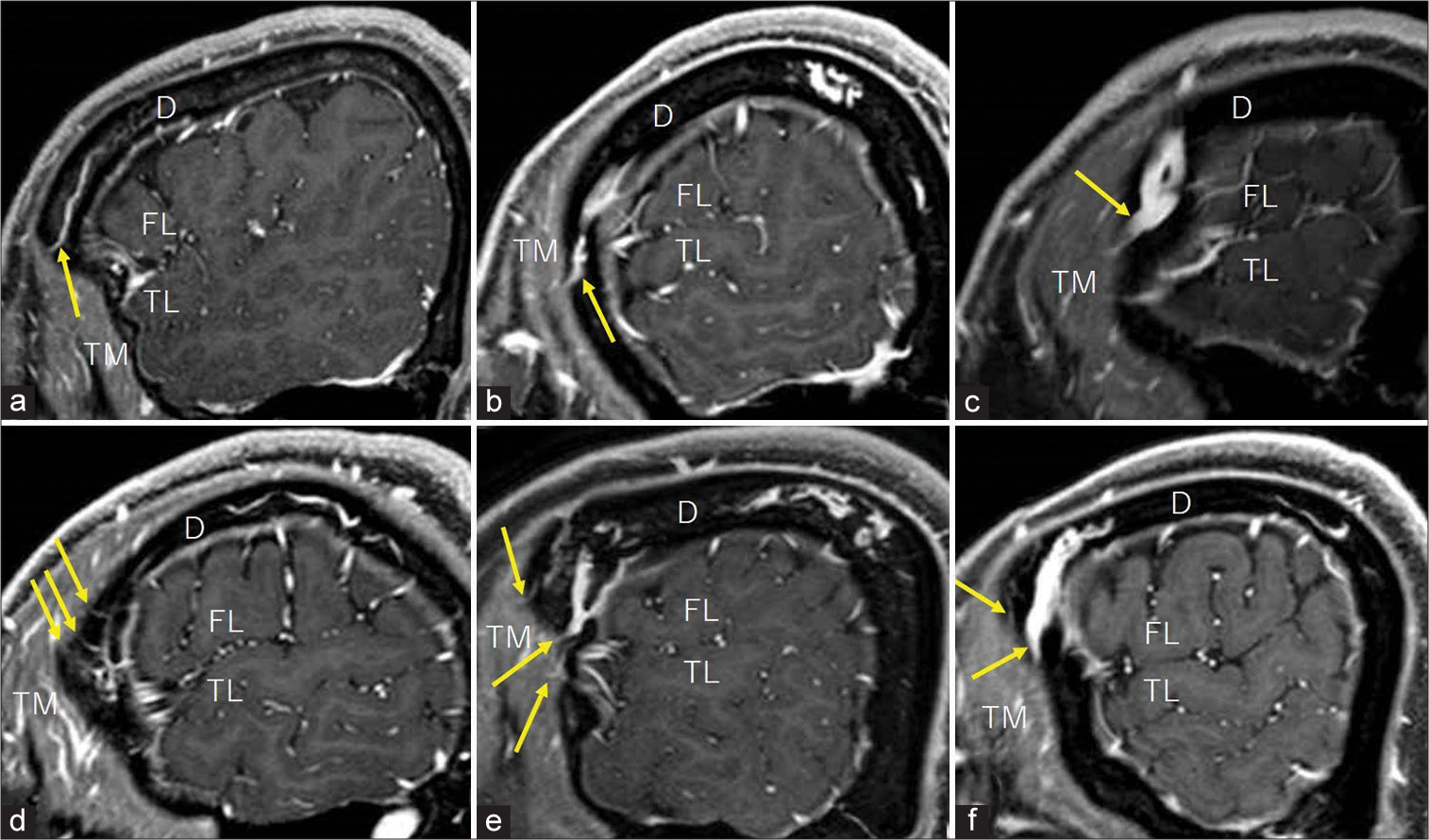
Figure 3:
Postcontrast sagittal T1-weighted magnetic resonance images of different patients showing the diploic veins of the pterional area supplying branches coursing into the extracranial sites with varying diameter and number (a-f, arrows). D: Diploe; FL: Frontal lobe; TL: Temporal lobe; TM: Temporalis muscle. Upper row: Left side; lower row: Right side.
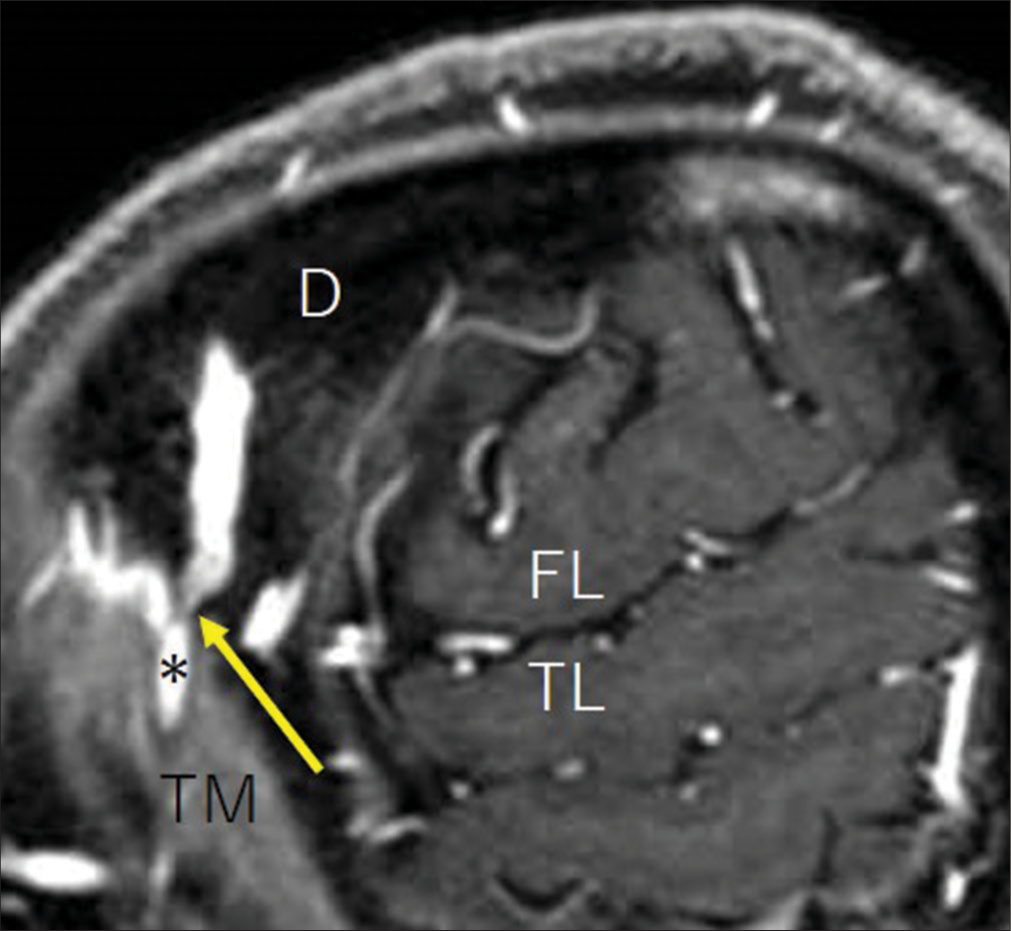
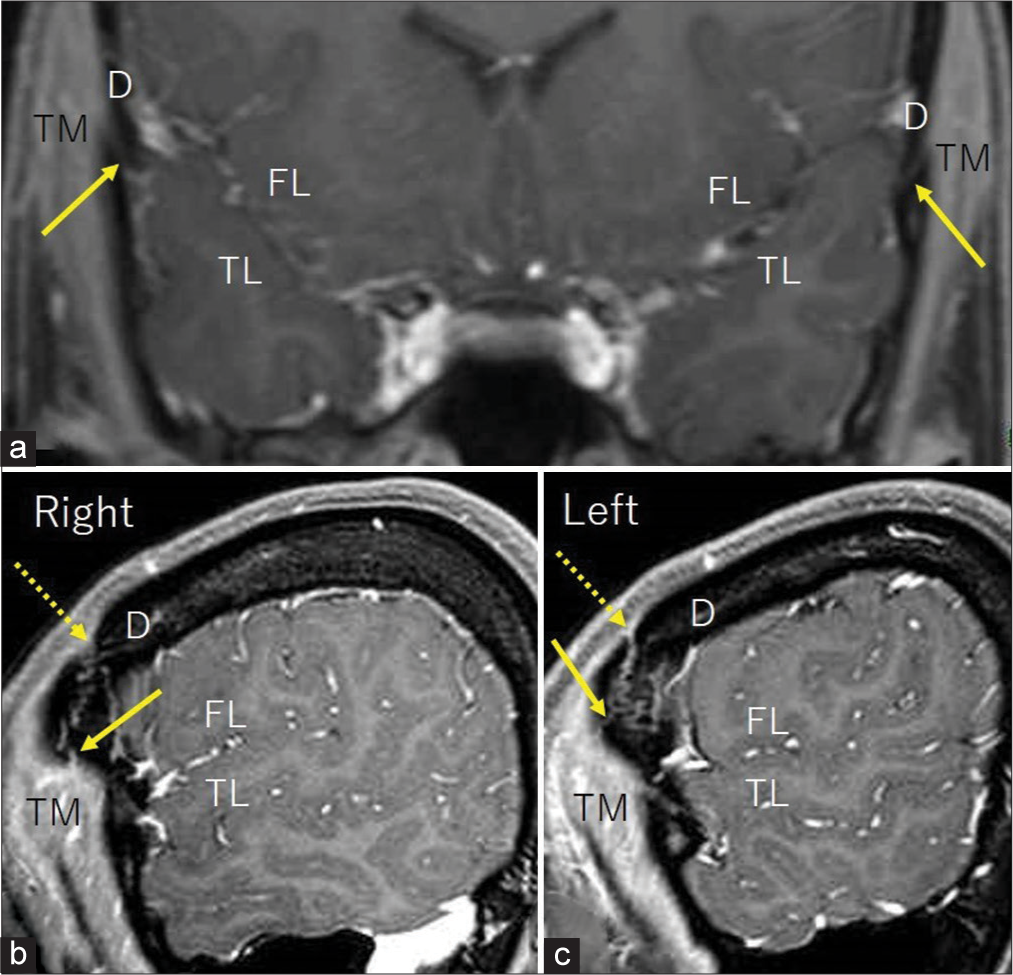
Figure 5:
Postcontrast coronal (a) and sagittal (b and c) T1-weighted magnetic resonance images at the corresponding levels showing the diploic veins draining into the extracranial sites both in the frontal skull region (b and c, dashed arrow) and pterional area (a-c, arrows). D: Diploe; FL: Frontal lobe; TL: Temporal lobe; TM: Temporalis muscle.
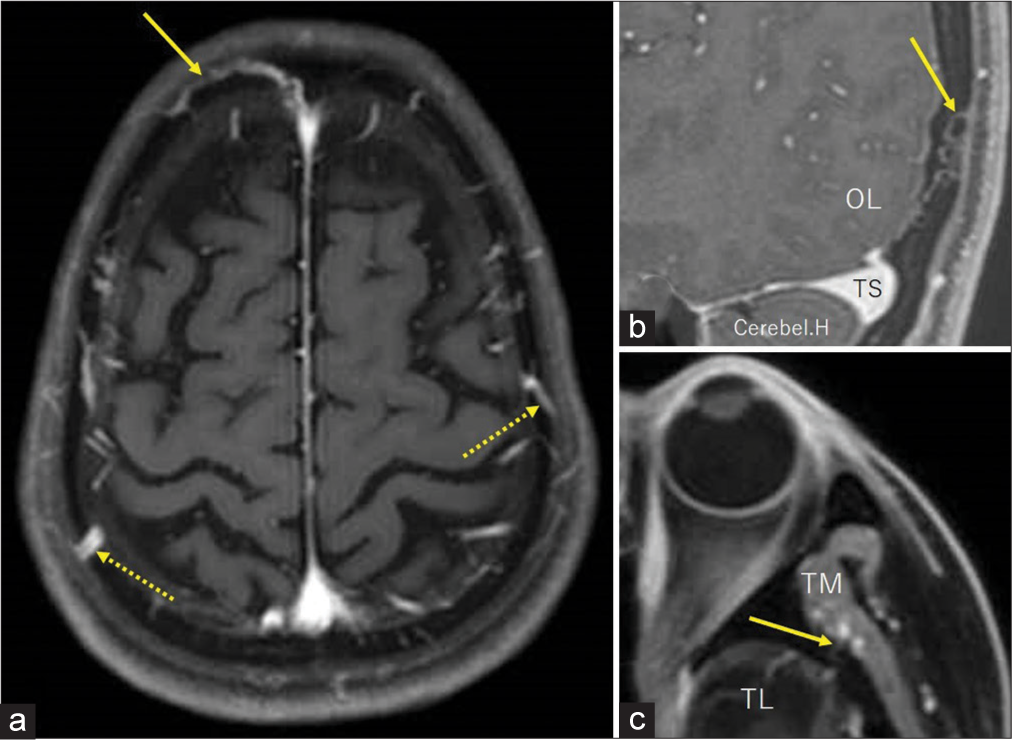
Figure 6:
Postcontrast axial (a), sagittal (b), and axial (c) T1-weighted magnetic resonance images of different patients showing the diploic veins draining into the extracranial sites in the frontal (a, arrow), parietal (a, dashed arrows), occipital (b, arrow), and temporal (c, arrow) skull regions.Cerebel. H: Right cerebellar hemisphere; OL: Occipital lobe; TL: Left temporal lobe; TM: Temporalis muscle; TS: Transverse sinus.
Cadaver dissection
On all dissected sides, part of the DVs injected with blue silicone was observed to course superficially in the diploe of the pterional area [
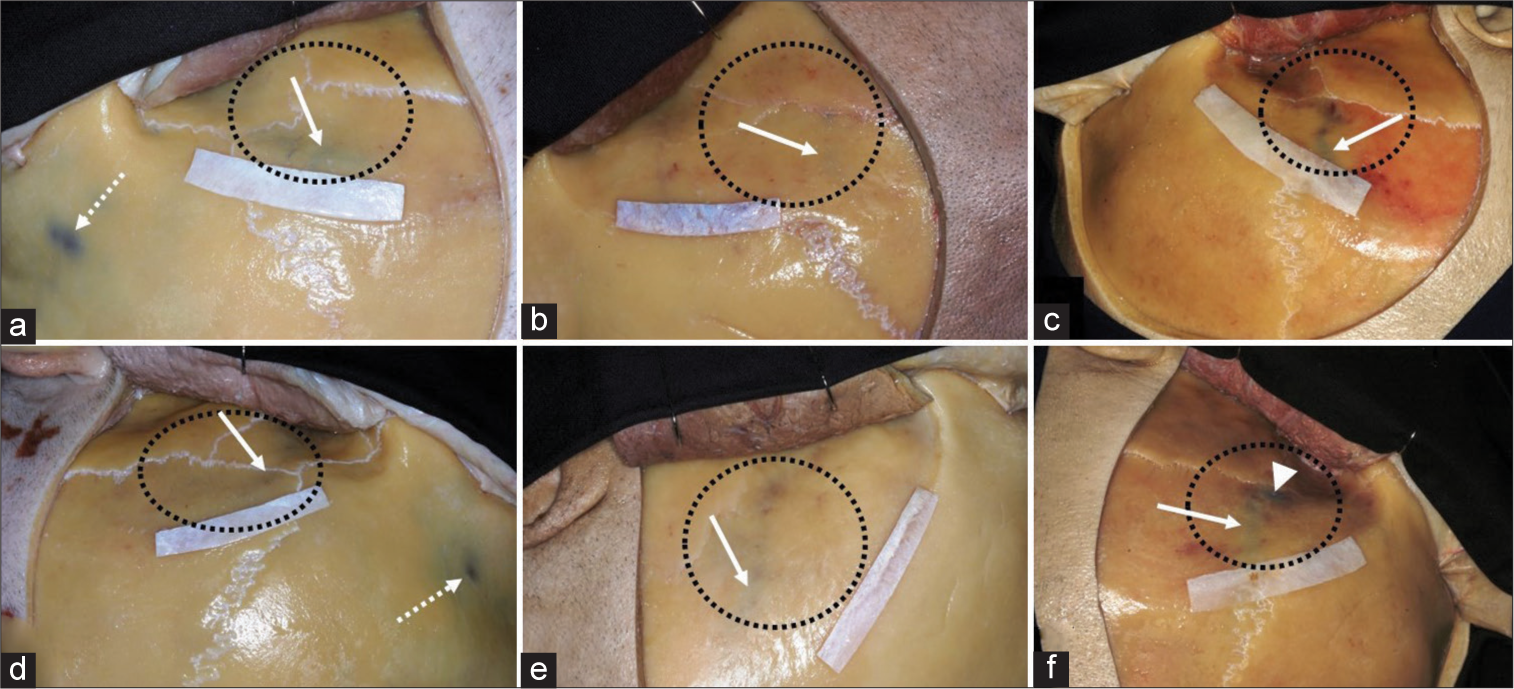
Figure 7:
(a-f) Six sides of three injected cadaver heads, after reflection of the scalp flaps for performing conventional frontotemporal craniotomies, showing the diploic veins coursing superficially in the diploe (arrow) of the pterional area (within dashed circle). On one side, a diploic vein in the area is open to the extracranial site (f, arrowhead). Dashed arrow: Diploic vein in the frontal bone; upper row: Right side; lower row: left side.
DISCUSSION
Despite investigations, connections between the intracranial and extracranial venous systems through calvarial DVs have not yet been documented.[
This study had several limitations. The cohort for MRI examinations consisted of patients with an inhomogeneous age distribution and uneven sex ratio. The patients were retrospectively evaluated and not randomly assigned. Furthermore, the DVs coursing through the pterional area were assessed using thin-sliced, contrast-enhanced MRI and a few dissected specimens. In contrast to a previous study describing ontogenetic changes in calvarial DVs, this study did not find such changes in DVs coursing in the pterional area or their branches connected to the extracranial venous system.[
CONCLUSION
The study showed that part of the diploic venous flow drains extracranially in the pterional area. This area may provide an important interface between the calvarial DVs and the extracranial venous system.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alarfaj A, Sankar T, Bhargava R, Tyler J, Walji A, Fox R. Magnetic resonance imaging analysis of human skull diploic anatomy. Surg Neurol Int. 2021. 12: 249
2. Asano K, Sobata E, Kubo O. Subepicranial varix mimicking sinus pericranii: Usefulness of three-dimensional computed tomography angiography and bone window computed tomography--case report. Neurol Med Chir (Tokyo). 2000. 40: 467-71
3. Aydin ME, Kopuz C, Demir MT, Corumlu U, Kaya AH. Localization of pterion in neonatal cadavers: A morphometric study. Surg Radiol Anat. 2010. 32: 545-50
4. Chang YC, Cantelmi D, Wisco JJ, Fattah A, Hannam AG, Agur AM. Evidence for the functional compartmentalization of the temporalis muscle: A 3-dimensional study of innervation. J Oral Maxillofac Surg. 2013. 71: 1170-7
5. Cheung LK. The blood supply of the human temporalis muscle: A vascular corrosion cast study. J Anat. 1996. 189: 431-8
6. García-González U, Cavalcanti DD, Agrawal A, Gonzalez LF, Wallace RC, Spetzler RF. The diploic venous system: Surgical anatomy and neurosurgical implications. Neurosurg Focus. 2009. 27: E2
7. Iwamuro H, Ikeda S, Taniguchi M. A rare case of diploic venous anomaly: Asymptomatic venous sac expanding in the diploe. Springerplus. 2016. 5: 1926
8. Kaido T, Kim YK, Ueda K. Diagnostic and therapeutic considerations for sinus pericranii. J Clin Neurosci. 2006. 13: 788-92
9. Natsis K, Antonopoulos I, Politis C, Nikolopoulos E, Lazaridis N, Skandalakis GP. Pterional variable topography and morphology. An anatomical study. Folia Morphol (Warsz). 2021. 80: 994-1004
10. Rangel-de Lázaro G, Neubauer S, Gunz P, Bruner E. Ontogenetic changes of diploic channels in modern human. Am J Phys Anthropol. 2020. 173: 96-111
11. Tsutsumi S, Nakamura M, Tabuchi T, Yasumoto Y, Ito M. Calvarial diploic venous channels: An anatomic study using high-resolution magnetic resonance imaging. Surg Radiol Anat. 2013. 35: 935-41
12. Tsutsumi S, Ono H, Ishii H, Yasumoto Y. Diploic veins of the cranial base: An anatomical study using magnetic resonance imaging. Surg Radiol Anat. 2019. 41: 1029-36
13. Tsutsumi S, Ono H, Yasumoto Y, Ishii H. Possible cerebrospinal fluid pathways in the middle fossa floor and pterional diploe: A magnetic resonance imaging study. Surg Radiol Anat. 2019. 41: 1045-51
14. Uz A, Korkmaz AC, Filgueira L, Guner MA, Tubbs RS, Demirciler AK. Anatomic analysis of the internal and external aspects of the pterion. World Neurosurg. 2020. 137: 84-8

