

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran.
DOI:10.25259/SNI_104_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Housain Soufiani, Shaghayegh Rahimizadeh. Double-level myelopathy due to atlantoaxial dislocation (os odontoideum) and subaxial cervical spondylosis with angular kyphosis. 09-May-2020;11:100
How to cite this URL: Abolfazl Rahimizadeh, Housain Soufiani, Shaghayegh Rahimizadeh. Double-level myelopathy due to atlantoaxial dislocation (os odontoideum) and subaxial cervical spondylosis with angular kyphosis. 09-May-2020;11:100. Available from: https://surgicalneurologyint.com/surgicalint-articles/10011/
Date of Submission
16-Mar-2020
Date of Acceptance
15-Apr-2020
Date of Web Publication
09-May-2020
Abstract
Background: The surgical management of cervical spondylotic myelopathy (CSM) attributed to os odontoideum (OO with atlantoaxial instability atlantoaxial instability) and subaxial kyphosis together pose significant surgical challenges.
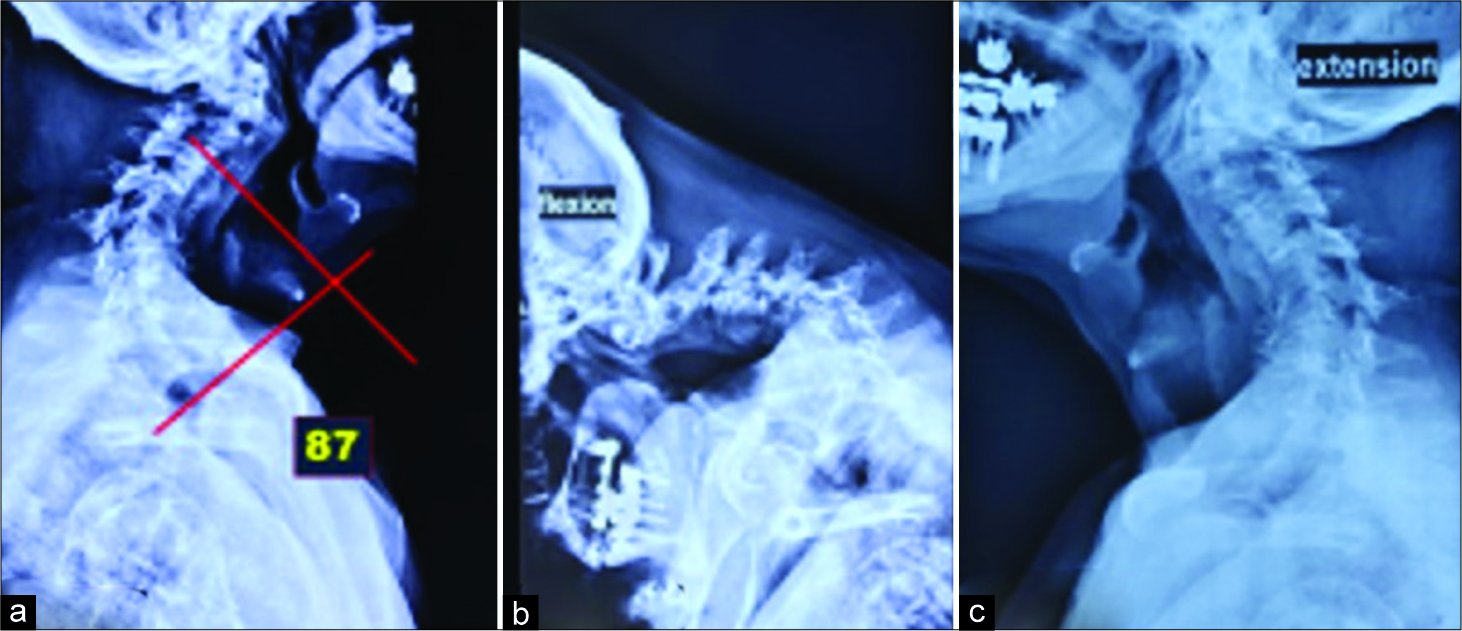
Case Description: An elderly male presented with CSM/myelopathy and severe quadriparesis attributed to an unstable OO and 87° fixed, subaxial cervical kyphosis. After performing a 540° spinal cord decompression with atlantoaxial fixation, the patient did well.
Conclusion: Double-level CSM due to an unstable OO and subaxial kyphosis is rare and typically requires combined 540° decompression and stabilization.
Keywords: Anterior osteotomy, Cervical spine, Fixed cervical kyphosis, Pedicle screw fixation, Smith-Peterson osteotomy
INTRODUCTION
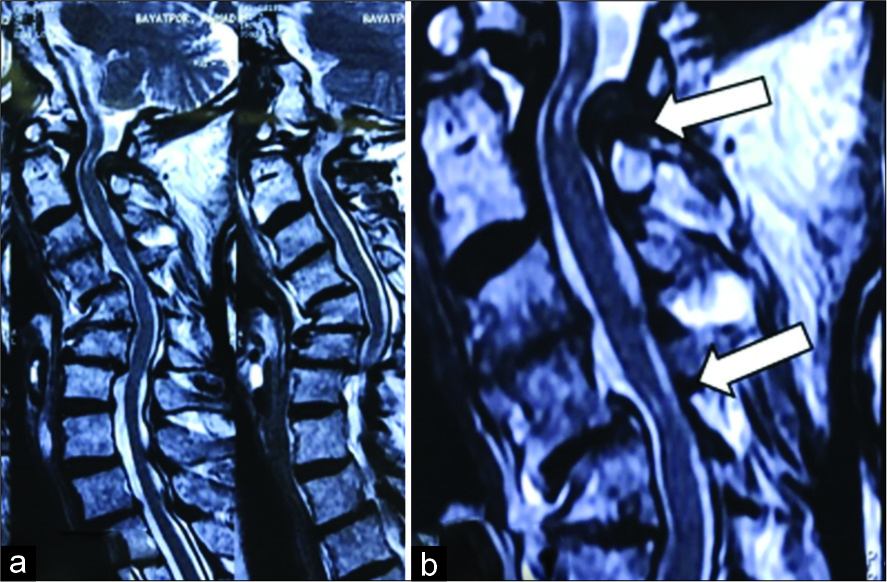
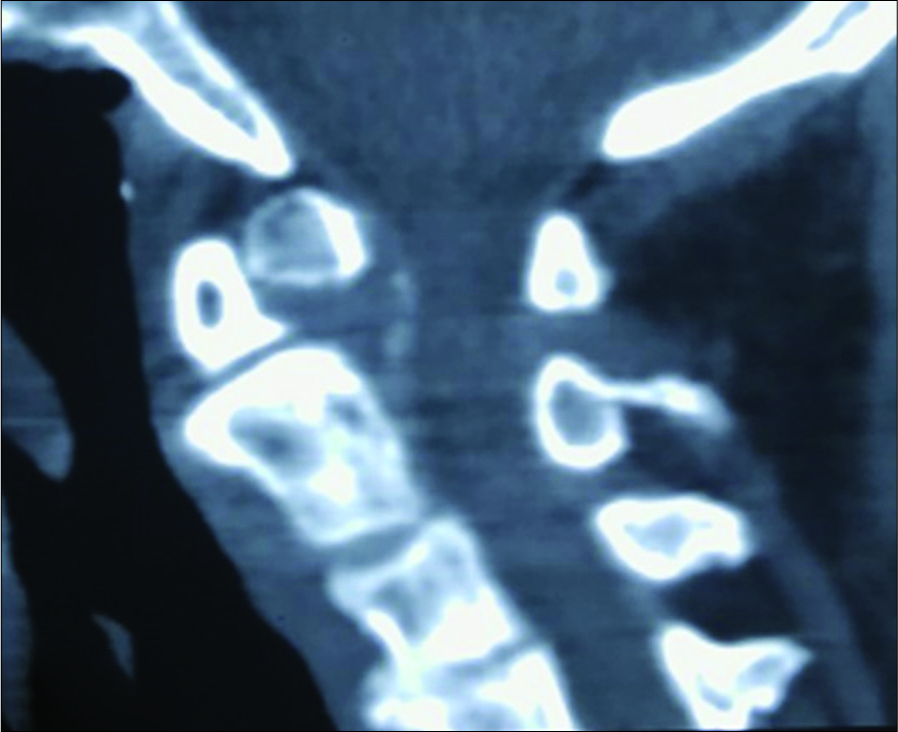
Unstable os odontoideum (OO) with atlantoaxial dislocation and subaxial “draping of the cervical spinal cord” over a kyphotic deformity contributed to dual-level significant cord compression and myelopathy in a 78-year-old male.[
Following a 540° anterior-posterior-anterior decompression and fusion, the patient improved.
CASE REPORT
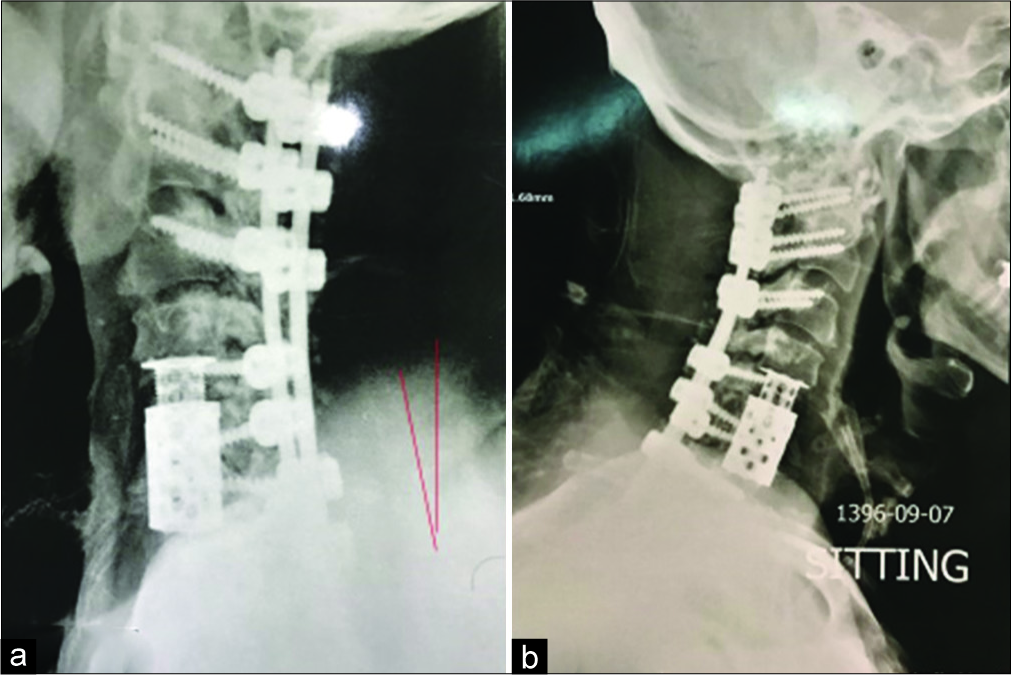
A 78-year-old wheel chair bound male developed a severe spastic quadriparesis with sphincter disturbance over a 2-year period. His modified Japanese Orthopedic Association (mJOA) score was 8. Cervical X-rays, MR, and CT studies demonstrated OO instability with subaxial C4-C6 cord compression; there was an accompanying 87° fixed kyphosis [
Surgical intervention
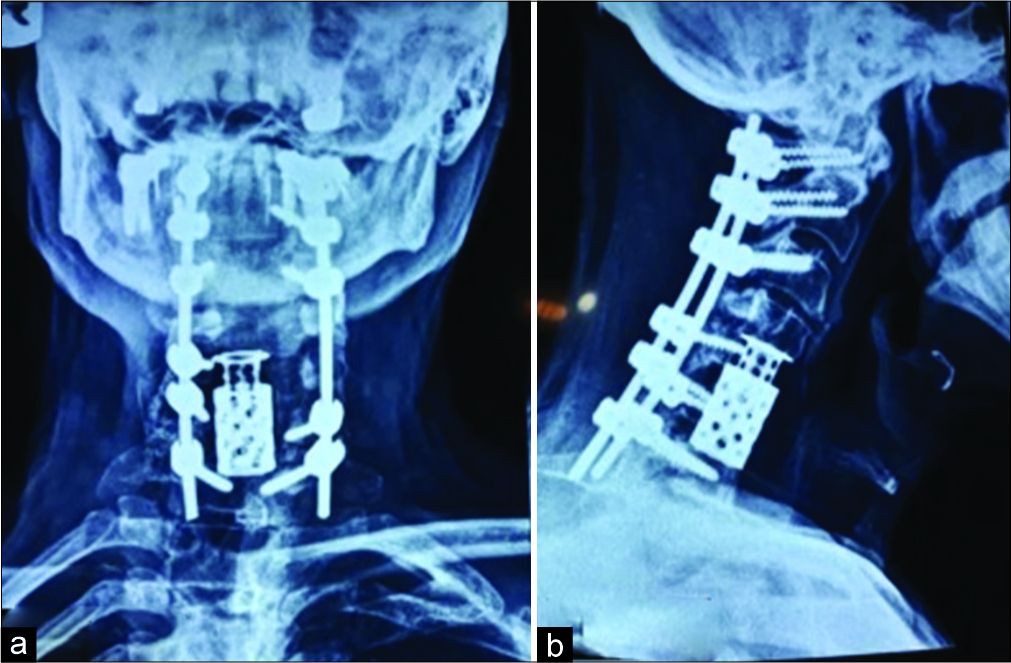
The patient underwent a C2 to C7 laminectomy with C1 lateral mass screw placements and insertion of bilateral pedicle screws from C2 to C7 bilaterally [

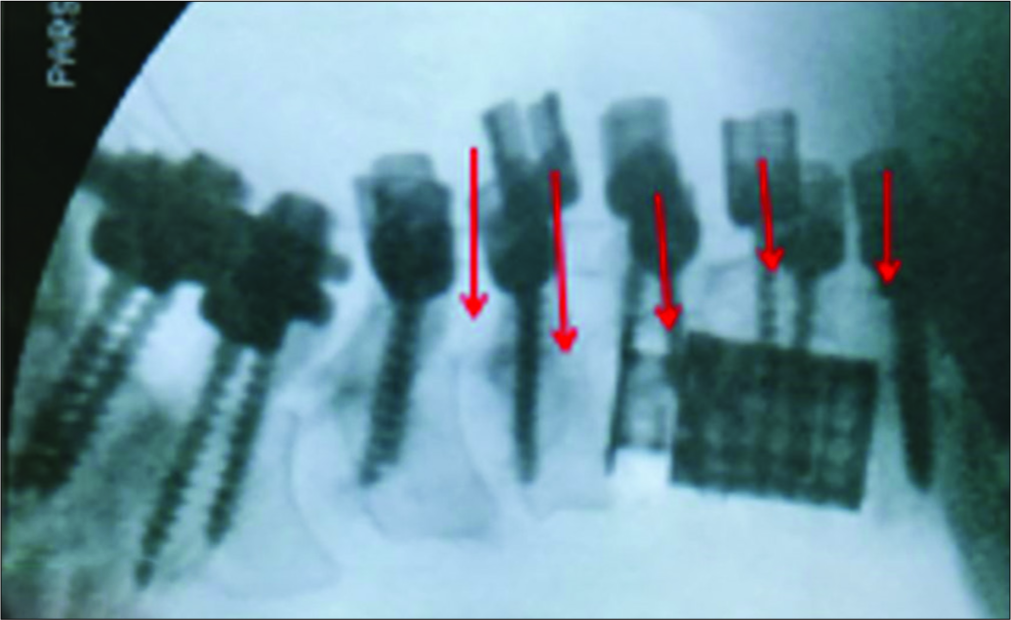
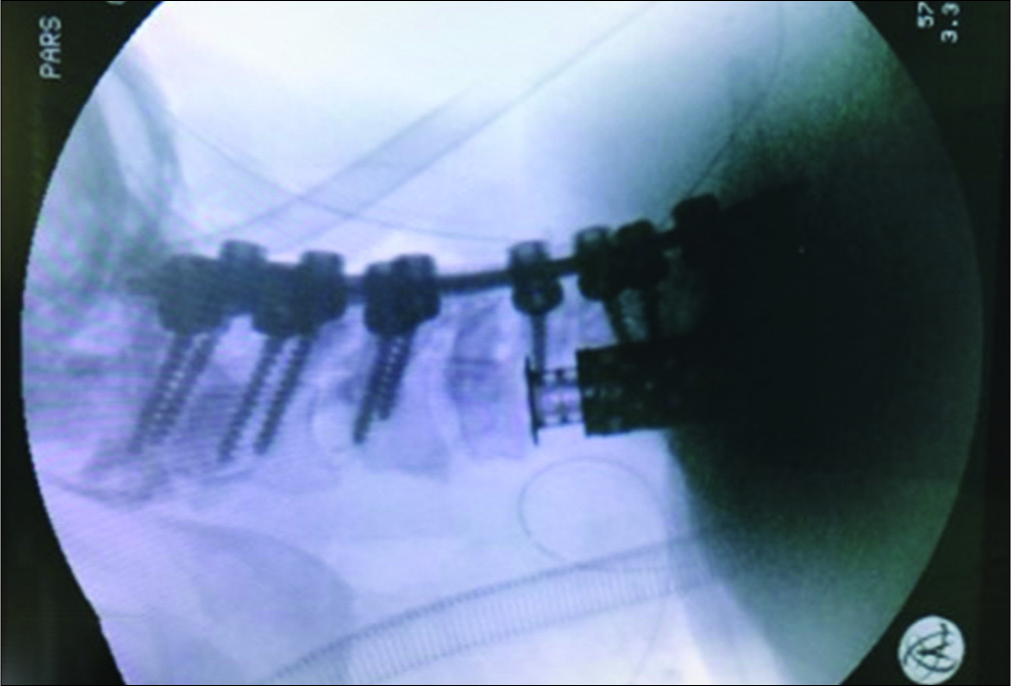
The intraoperative cervical cross-table X-ray ultimately confirmed adequate C1 to C7 instrumentation with a 100° correction of the kyphosis [
DISCUSSION
Management of OO with instability
The discovery of a symptomatic OO in an elderly patient is rare; we found only 12 such cases in the literature.[
Treatment of subaxial CK
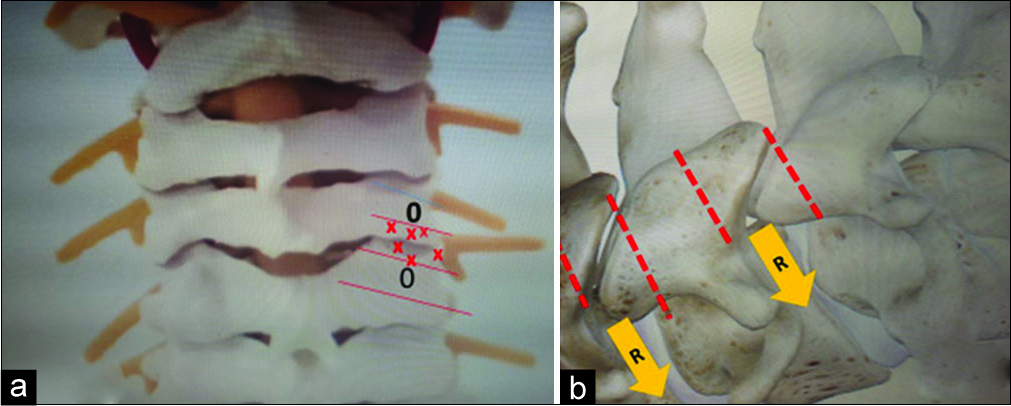
With an angular kyphosis from 30° to 90°, 540° surgery with a combination of anterior-posterior-anterior decompression/fusion may be warranted. In this case, while supine, the patient underwent a two-level corpectomy with three-level anterior osteotomy (C4-C6) (ATO).[
CONCLUSION
For patients displaying OO/instability and subaxial cervical kyphosis, combined anterior followed by posterior decompression/fusion surgery may be warranted.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ganju A, Ondra SL, Shaffrey CI. Cervical kyphosis. Tech Orthop. 2002. 17: 345-54
2. Kim HJ, Piyaskulkaew C, Riew KD. Anterior cervical osteotomy for fixed cervical deformities. Spine (Phila Pa 1976). 2014. 39: 1751-7
3. O’Shaughnessy BA, Liu JC, Hsieh PC, Koski TR, Ganju A, Ondra SL. Surgical treatment of fixed cervical kyphosis with myelopathy. Spine (Phila Pa 1976). 2008. 33: 771-8
4. Rahimizadeh A, Malekmohammadi Z, Karimi M, Rahimizadeh A, Asgari N. Unstable os odontoideum contributing to cervical myelopathy and obstructive sleep apnea. Surg Neurol Int. 2019. 10: 125-
5. Rahimizadeh A, Rahimizadeh A. Os odontoideum: A review article. Orthop Res Traumatol. 2016. 1: 33-55
6. Rahimizadeh A, Soufiani HF, Hassani V, Rahimizadeh A. Atlantoaxial subluxation due to an os odontoideum in an achondroplastic adult: Report of a case and review of the literature. Case Rep Orthop. 2015. 2015: 142586-
7. Rahimizadeh A, Williamson WL, Rahimizadeh S, Amirzadeh M. Atlantoaxial subluxation secondary to unstable os odontoideum in a patient with arrested hydrocephalus due to congenital aqueductal stenosis: A case report. Int J Spine Surg. 2018. 12: 549-56
8. Rahimizadeh A, Williamson WL, Rahimizadeh S, Amirzadeh M. Surgical management of an elderly patient with free floating os odontoideum. J Spine Neurosurg. 2019. 8: 1-4
9. Rimizadeh A, Habibi G. Os odontoideum in an elderly: Report of a case and review. World Spinal Column J. 2011. 2: 102-8
10. Rimizadeh A. Oral Presentation: Marked Cervical Kyphotic Deformity: Report of 22 Cases with Special Reference to Multilevel Cervical Posterior Osteotomy. Eur spine J. 2016. 25: S334-S76
11. Sin AH, Acharya R, Smith DR, Nanda A. Adopting 540-degree fusion to correct cervical kyphosis. Surg Neurol. 2004. 61: 515-22

