

- Department of Neurosurgery, Kawasaki Saiwai Hospital, Kawasaki, Japan.
Correspondence Address:
Hidenori Matsuoka, Department of Neurosurgery, Kawasaki Saiwai Hospital, Kawasaki, Japan.
DOI:10.25259/SNI_286_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hidenori Matsuoka, So Ohashi, Michihisa Narikiyo, Ryo Nogami, Hirokazu Nagasaki, Yoshifumi Tsuboi. Dysphagia after occipital cervical fusion for retro-odontoid pseudotumor with ossification of the anterior longitudinal ligament. 29-Apr-2022;13:184
How to cite this URL: Hidenori Matsuoka, So Ohashi, Michihisa Narikiyo, Ryo Nogami, Hirokazu Nagasaki, Yoshifumi Tsuboi. Dysphagia after occipital cervical fusion for retro-odontoid pseudotumor with ossification of the anterior longitudinal ligament. 29-Apr-2022;13:184. Available from: https://surgicalneurologyint.com/surgicalint-articles/11560/
Date of Submission
26-Mar-2022
Date of Acceptance
06-Apr-2022
Date of Web Publication
29-Apr-2022
Abstract
Background: Ossification of the anterior longitudinal ligament (OALL) of the cervical spine is a relatively rare disease. If patients present with dysphagia, hoarseness, and/or dyspnea, they may require surgery.
Case Description: Over a 7-month period, a 55-year-old female with a history of cerebral palsy developed a progressive quadriparesis accompanied by diffuse sensory loss (i.e., clumsiness of the hand/legs and gait disturbance). The cervical spine X-rays showed atlanto-axial subluxation with instability, while the cervical MRI demonstrated “pseudotumor in the retro-odontoid” region. Following an occipital cervical fusion (C0-C2) surgery, her quadriparesis resolved. Nevertheless, she had persistent dysphagia that worsened over 6 months. Video fluoroscopy revealed severe mechanical stenosis of the pharynx, which was attributed to OALL extending from the C3-C6 levels. Following OALL resection through a right anterior approach utilizing diamond burrs and an ultrasonic bone curette, the dysphagia rapidly resolved.
Conclusion: We report a rare case of retro-odontoid pseudotumor successfully treated with a posterior C0-C2 cervical fusion. Additional symptomatic C3-C6 OALL, responsible for progressive dysphagia, was later managed with focal anterior OALL resection.
Keywords: Atlanto-axial subluxation, Dysphasia, Occipital cervical fusion, Symptomatic OALL, Video fluoroscopy
INTRODUCTION
Cervical ossification of the anterior longitudinal ligament (OALL), a subtype of diffuse idiopathic skeletal hyperostosis (DISH), rarely causes dysphagia requiring direct anterior cervical resection.[
CASE DESCRIPTION
Over a 7-month period, a 55-year-old female with a history of athetoid cerebral palsy developed a progressive quadriparesis. Cervical X-rays showed atlanto-axial subluxation (AAS) with instability. The cervical MR showed a retro-odontoid “pseudotumor” focally compressing the ventral cord, while the cervical CT showed OALL extending from C3-C6. For her progressive myelopathy and retro-odontoid mass with AAS, she underwent that a C0-C2 posterior fusion with C1 was arch resection. Postoperatively, although her quadriparesis resolved, she exhibited increasing dysphagia., The follow-up MRI demonstrated regression of the retro-odontoid pseudotumor [
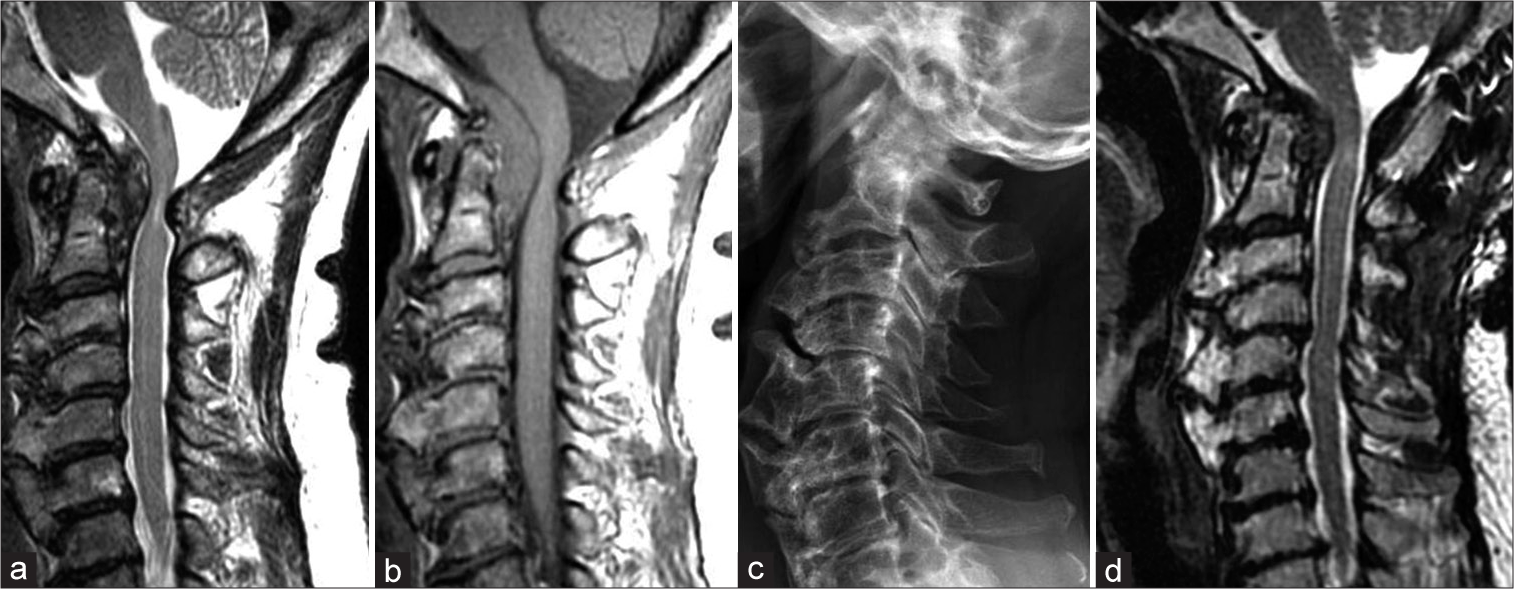
Figure 1:
Preoperative MRI showed severe compression of spinal nerves due to retro-odontoid tumor (a: T2WI, b: T1WI). Cervical X-ray showed OALL like a bird’s beak at the C3-6 level (c), and follow-up MRI 6 months after the first surgery clearly showed that the cerebrospinal fluid around the spinal cord had recovered and the retro-odontoid tumor was shrinking (d).
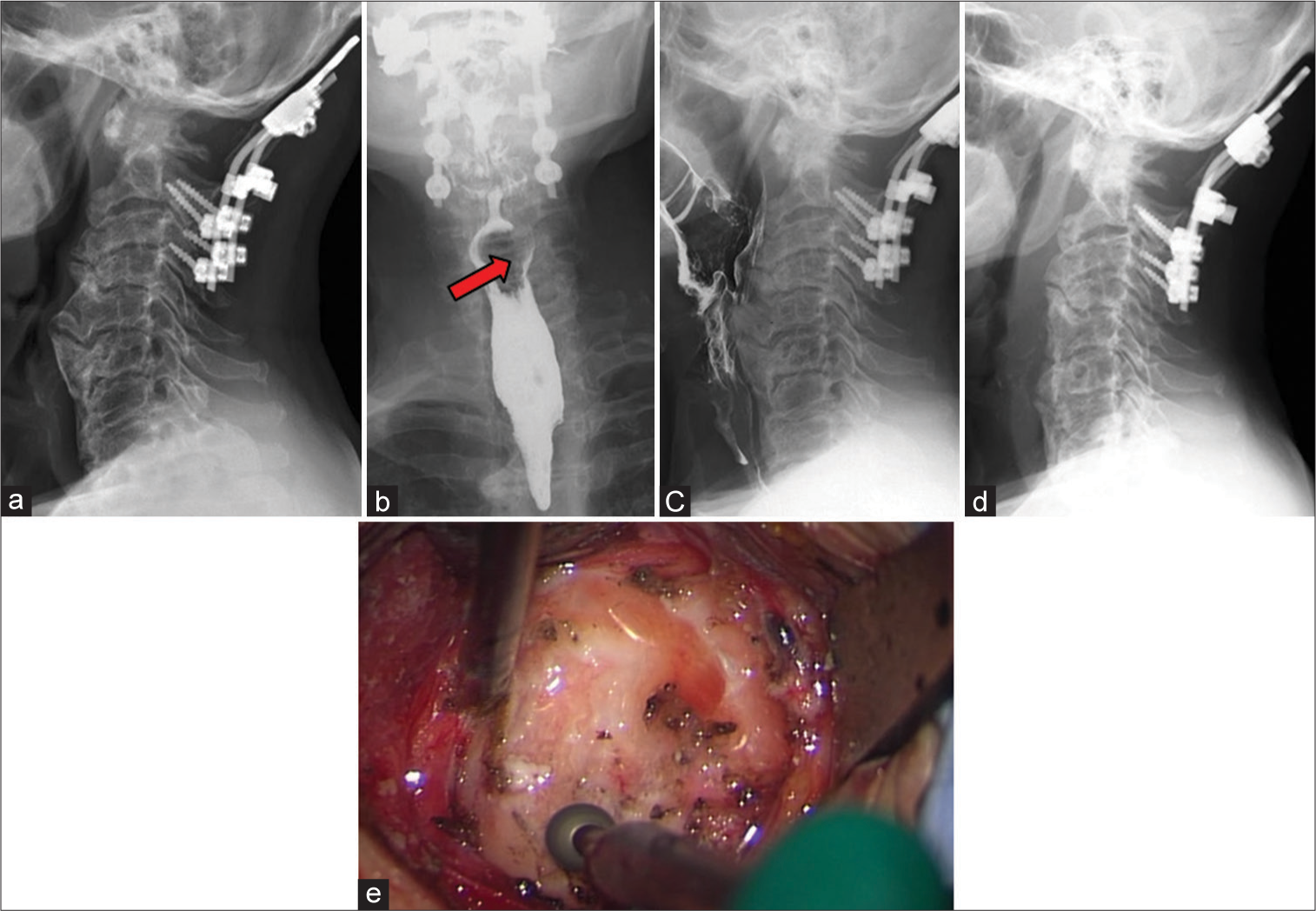
Figure 2:
Aggressive OALL is prominent on cervical X-ray after the first surgery (a). Preoperative video fluoroscopy revealed a filling defect due to OALL at the C5/6 level (b,c). The red arrow in Figure 2b indicates contrast loss. Cervical X-ray after OALL resection showing adequate smoothening of the OALL (d). In the operative field, the OALL is flattened with a diamond burr (e).
DISCUSSION
OALL, also called Forestier’s disease, is considered a subtype of DISH.[

CONCLUSION
Patients with retro-odontoid “pseudotumor” may require a posterior C0-C2 fusion. Here, the preoperative workup should include both an MR and CT to determine if there is any accompanying subaxial cervical OALL that may become symptomatic following the C0-C2 fusion and later require direct anterior OALL resection.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Epstein NE, Hollingsworth R. Ossification of the cervical anterior longitudinal ligament contributing to dysphagia. Case report. J Neurosurg. 1999. 90: 261-3
2. Forestier J, Rotes-Querol J. Senile ankylosing hyperostosis of the spine. Ann Rheum Dis. 1950. p. 9321-30
3. Izeki M, Neo M, Takemoto M. Fujibayashi S, Ito H, Nagai K. The O-C2 angle established at occipito-cervical fusion dictates the patient’s destiny in terms of postoperative dyspnea and/or dysphagia. Eur Spine J. 2014. 23: 328-36
4. Kaneyama S, Sumi M, Takabatake M, Kasahara K, Kanemura A, Hirata H. The prediction and prevention of dysphasia after occipitospinal fusion by use of the S-line (swallowing line). Spine. 2017. 42: 718-25
5. Miyata M, Neo M, Fujibayashi S, Ito H, Takemoto M, Nkamura T. O-C2 angle as a predictor of dyspnea and/or dysphagia after occipitocervical fusion. Spine (Phila Pa 1976). 2009. 34: 184-8
6. Mizuno J, Nakagawa H, Song J. Symptomatic ossification of the anterior longitudinal ligament with stenosis of the cervical spine: A report of seven cases. J Bone Joint Surg Br. 2005. 87: 1375-9
7. Nishimura H, Endo K, Aihara T, Murata K, Suzuki H, Matsuoka Y. Risk factor of dysphagia in patients with ossification of the anterior longitudinal ligament. J Orthop Surg (Hong Kong). 2020. 28: 1-5
8. Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology. 1976. 119: 559-68
9. Song J, Mizuno J, Nakagawa H. Clinical and radiological analysis of ossification of the anterior longitudinal ligament causing dysphasia and hoarseness. Neurosurgery. 2006. 58: 913-9

