

- Department of Neurosurgery, Otsu City Hospital,
- Department of Rehabilitation, Hikari Hospital, Shiga, Japan.
Correspondence Address:
Toshinari Kawasaki, Department of Neurosurgery, Otsu City Hospital, Shiga, Japan.
DOI:10.25259/SNI_189_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Toshinari Kawasaki1, Motohiro Takayama1, Yoshinori Maki2, Tamaki Kobayashi1, Yoshihiko Ioroi1. Early postoperative sacral fracture after short-segment posterior lumbar interbody fusion for L5/S1 isthmic spondylolisthesis: A case report. 15-Apr-2022;13:142
How to cite this URL: Toshinari Kawasaki1, Motohiro Takayama1, Yoshinori Maki2, Tamaki Kobayashi1, Yoshihiko Ioroi1. Early postoperative sacral fracture after short-segment posterior lumbar interbody fusion for L5/S1 isthmic spondylolisthesis: A case report. 15-Apr-2022;13:142. Available from: https://surgicalneurologyint.com/surgicalint-articles/11541/
Date of Submission
19-Feb-2022
Date of Acceptance
16-Mar-2022
Date of Web Publication
15-Apr-2022
Abstract
Background: Early postoperative sacral fractures are extremely rare complications of single-level posterior lumbar interbody fusions (PLIFs).
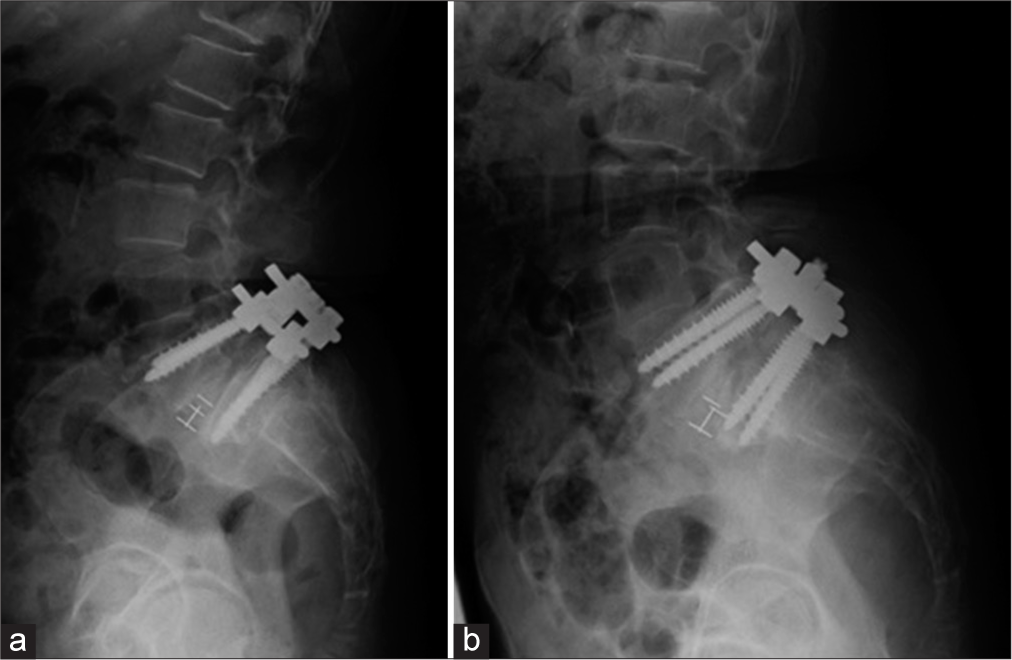
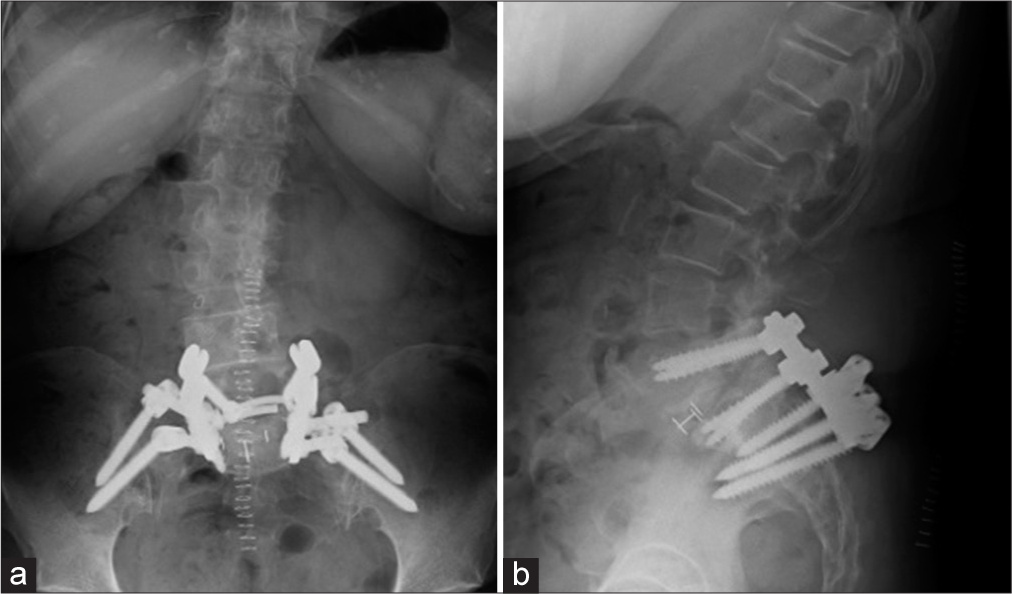
Case Description: A 71-year-old female presented with lower back pain and right S1 radiculopathy attributed to MR-documented L5/S1 isthmic spondylolisthesis. Following a L5 laminectomy and bilateral L5/S1 PLIF, she experienced sacral pain while sitting. When the MR showed a sacral insufficiency fracture with anterolisthesis at L5/S1, a secondary posterior fusion was extended to the pelvis, utilizing bilateral iliac screws. Following this reoperation, the patient did well and went on to achieve arthrodesis.
Conclusion: Early postoperative sacral fractures that occur following single-segment L5/S1 PLIF for isthmic spondylolisthesis warrant fusion to the pelvis with bilateral iliac screws.
Keywords: Iliac screws, Isthmic spondylolisthesis, Sacral fracture, Short-segment posterior lumbar interbody fusion
INTRODUCTION
Early postoperative sacral fractures following L5/S1 posterior lumbar interbody fusion (PLIF) are rare. Here, a 71-year-old female sustained a postoperative sacral fracture after a L5/S1 PLIF performed for isthmic spondylolisthesis. Following a secondary fusion to the pelvis utilizing bilateral iliac screws, the patient’s complaints resolved.
CASE DESCRIPTION
Clinical presentation and first surgery
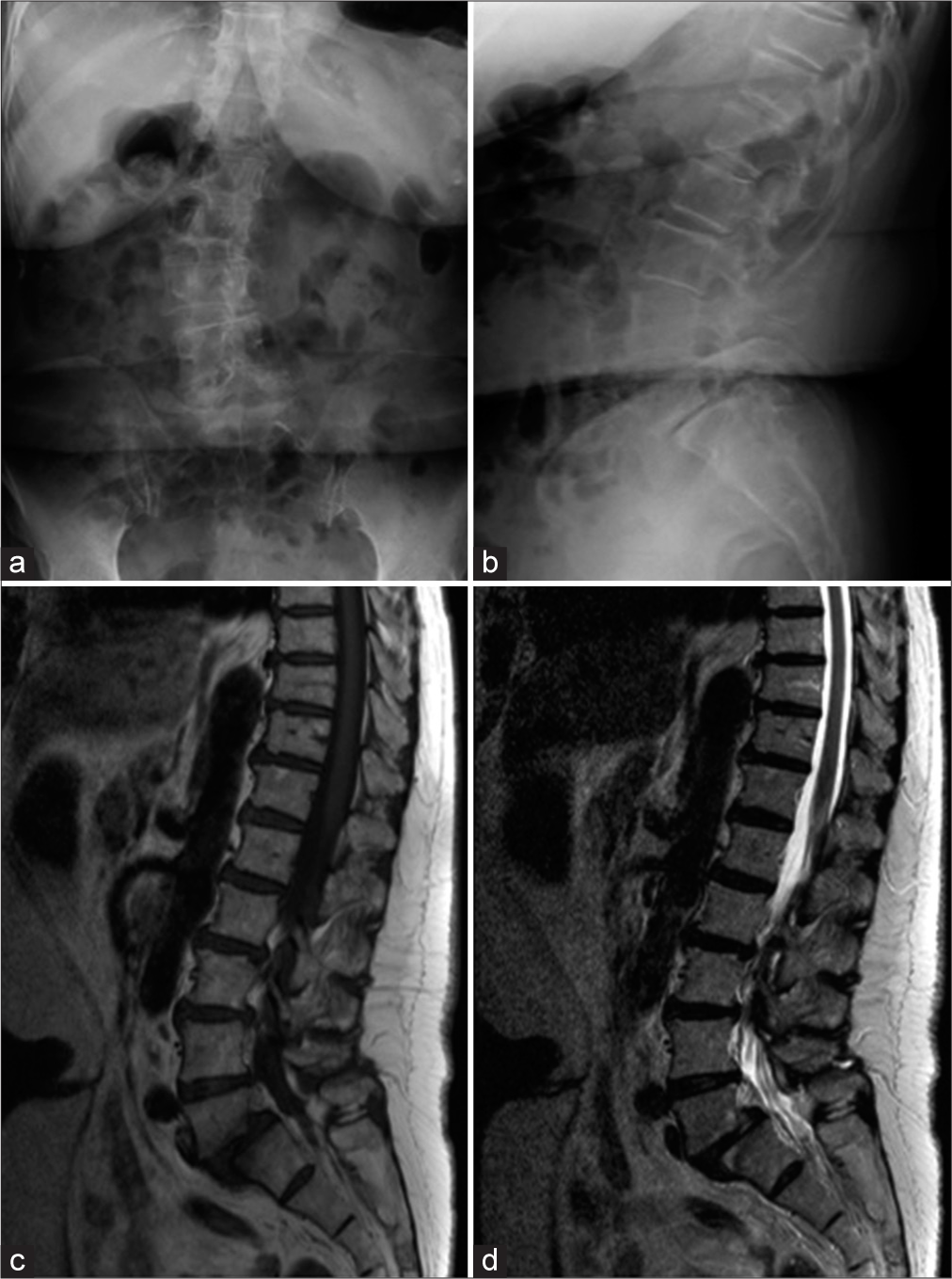
A 71-year-old female with low back pain and right lower extremity sciatica had initial MR and CT studies that revealed L5/S1 isthmic spondylolisthesis (near Grade 3) and a Cobb’s angle of 19.3° [

Second surgery
Two weeks later, the right leg numbness recurred. By the 3rd postoperative week, X-rays and MRI studies showed a sacral insufficiency fracture, with instability above the sacral fracture, and anterolisthesis of S1 [
DISCUSSION
Sacral insufficiency fractures are typically complications of previous long-segment instrumented lumbosacral fusions, but rarely involve single-level PLIF [

CONCLUSION
A 71-year-old female developed an early postoperative sacral fracture after a L5/S1 PLIF for isthmic spondylolisthesis. Following extension of the fusion to the pelvis using bilateral iliac screws, the patient became asymptomatic and achieved successful arthrodesis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Grimm JO, Jackson RP, Hamilton AC. Stress fracture of the pelvis: A complication following instrumented lumbar fusion. Orthop Trans. 1993. 17: 108
2. Klineberg E, McHenny T, Bellabarba C, Wagner T, Chapman J. Sacral insufficiency fractures caudal to instrumented posterior lumbosacral arthrodesis. Spine (Phila Pa 1976). 2008. 33: 1806-11
3. Mathews V, McCance SE, O’Leary PF. Early fracture of the sacrum or pelvis: An unusual complication after multilevel instrumented lumbosacral fusion. Spine (Phila Pa 1976). 2001. 26: E571-5
4. Odate S, Shikata J, Kimura H, Soeda T. Sacral fracture after instrumented lumbosacral fusion: Analysis of risk factors from spinopelvic parameters. Spine (Phila Pa 1976). 2013. 38: E223-9
5. Papadopoulos EC, Cammisa FP, Girardi FP. Sacral fractures complicating thoracolumbar fusion to the sacrum. Spine (Phila Pa 1976). 2008. 33: E699-707
6. Vavken P, Krepler P. Sacral fractures after multi-segmental lumbosacral fusion: A series of four cases and systematic review of literature. Eur Spine J. 2008. 17: S285-90
7. Wilde GE, Miller TT, Schneider R, Girardi FP. Sacral fractures after lumbosacral fusion: A characteristic fracture pattern. AJR Am J Roentgenol. 2011. 197: 184-8
8. Wood KB, Geissele AE, Ogilvie JW. Pelvic fractures after long lumbosacral spine fusions. Spine (Phila Pa 1976). 1996. 21: 1357-62

