

- Department of Spine Surgery, Baby Memorial Hospital, Calicut, Kerala, India,
- Department of Orthopedics, Baby Memorial Hospital, Calicut, Kerala, India,
- Department of Anaesthesia, Baby Memorial Hospital, Calicut, Kerala, India,
- Department of Hemato-Oncology, Baby Memorial Hospital, Calicut, Kerala, India,
- Neurology, Baby Memorial Hospital, Calicut, Kerala, India,
- Pathology, Baby Memorial Hospital, Calicut, Kerala, India.
Correspondence Address:
Suresh S. Pillai, Department of Spine Surgery, Arayidathu Bridge, Indira Gandhi Road, Calicut - 673 004, Kerala, India.
DOI:10.25259/SNI_567_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Suresh S. Pillai1, P. A. Ramsheela2, Rijil Deepak3, Shinto Francis4, C. Jayakrishnan5, Ani Praveen6, Neena Mampally6. Epidural extension of dorsal vertebral D1–D7 hemangiomas with congenital cutaneous hemangiomas: Case report and literature review. 13-Sep-2021;12:457
How to cite this URL: Suresh S. Pillai1, P. A. Ramsheela2, Rijil Deepak3, Shinto Francis4, C. Jayakrishnan5, Ani Praveen6, Neena Mampally6. Epidural extension of dorsal vertebral D1–D7 hemangiomas with congenital cutaneous hemangiomas: Case report and literature review. 13-Sep-2021;12:457. Available from: https://surgicalneurologyint.com/surgicalint-articles/11113/
Date of Submission
07-Jun-2021
Date of Acceptance
28-Jul-2021
Date of Web Publication
13-Sep-2021
Abstract
Background: There are only rare reports of simultaneous multiple thoracic vertebral, epidural, and congenital cutaneous hemangiomas occurring at the same levels.
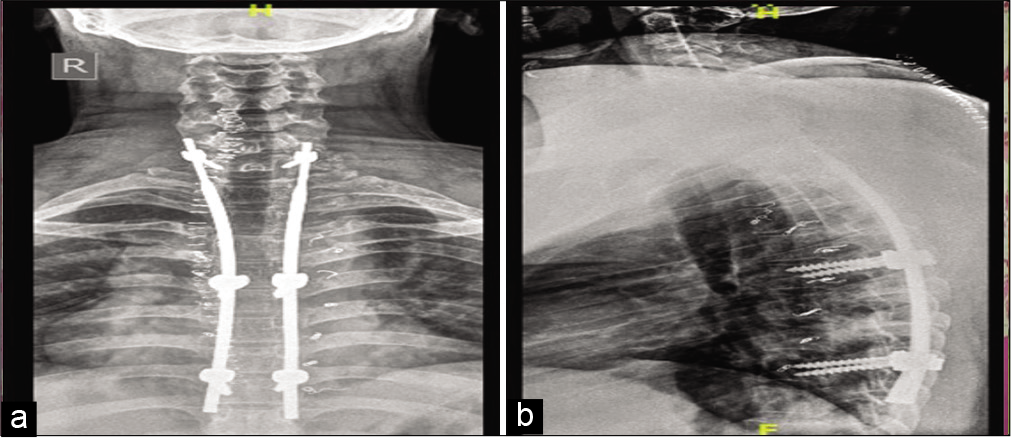
Case Description: A 24-year-old male presented with a progressive paraparesis attributed to multiple vertebral hemangiomas (MVH) with epidural extension (i.e. resulting in D1–D3 significant cord compression.), plus congenital cutaneous lesions at the D2–D7 levels. Following preoperative angioembolisation, a D1–D7 laminectomy was performed along with a C7–D8 pedicle screw fixation. Pathologically the bone and cutaneous lesions were spinal cavernous hemangiomas. Postoperatively, the patient regained normal function. As complete excision was not feasible, he subsequently received radiotherapy to prevent tumor recurrence.
Conclusion: MVH with multilevel epidural extension resulting in significant cord compression and congenital cutaneous lesions should undergo attempted tumor excision followed by radiation therapy where complete removal is not feasible.
Keywords: Compressive myelopathy, Congenital cutaneous hemangioma, Epidural hemangioma, Vertebral hemangioma
INTRODUCTION
Multiple vertebral hemangiomas (MVH) typically involve multiple vertebral bodies, and occasionally extend into the epidural space. They represent 2–3% of all spinal tumors, and usually follow an indolent, asymptomatic course. However, a subset may develop symptoms/ signs of significant cord compression, attributed to combinations of epidural cord compression, pathological fractures, and/or hemorrhages, warranting surgery. Histologically, MVH are characterized into one of three categories; the capillary, cavernous, arteriovenous, or the venous type. Here, a 24-year-old presented with the new onset of a paraparesis attributed to MVH extending from D1 to D7 with epidural extension/cord compression and accompanying cutaneous lesions at the same levels. The spinal lesion required extensive thoracic cord decompression with fusion, followed by radiation therapy to address residual disease.
CASE REPORT
A 24-year-old male presented with 6 months of a progressive paraparesis that exacerbated over the past 2 months. Notably, he had a large cherry red cutaneous lesion on the left side of the thorax, (i.e. left side of the chest from sternum to mid line at the back), also involving the left arm/forearm (i.e. from the nape of neck to just below the scapula involving the lateral/medial arm/forearm) since birth [

Neurological
On examination, he had 3–4/5 motor strength diffusely in the lower extremities and a relative sensory level below D4 level without sphincter involvement.
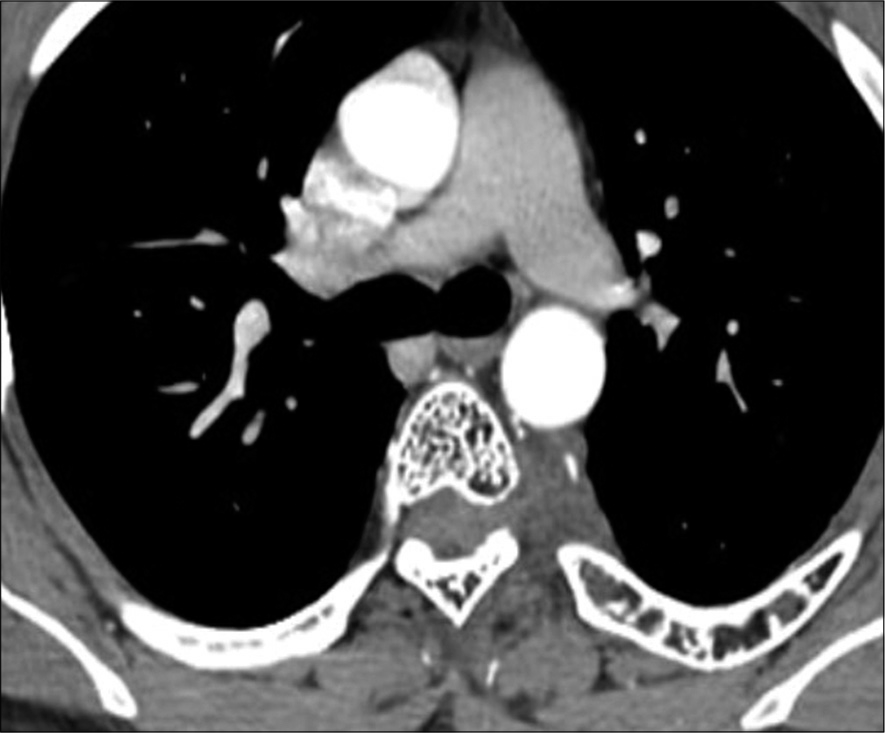
CT Findings
The thoracic CT showed irregular lytic lesions with coarse thickened trabeculae involving the D1 through D7 vertebral levels, also including the left 1st through 6th ribs. Axial studies showed the typical “polka-dot” pattern of vertebral involvement [
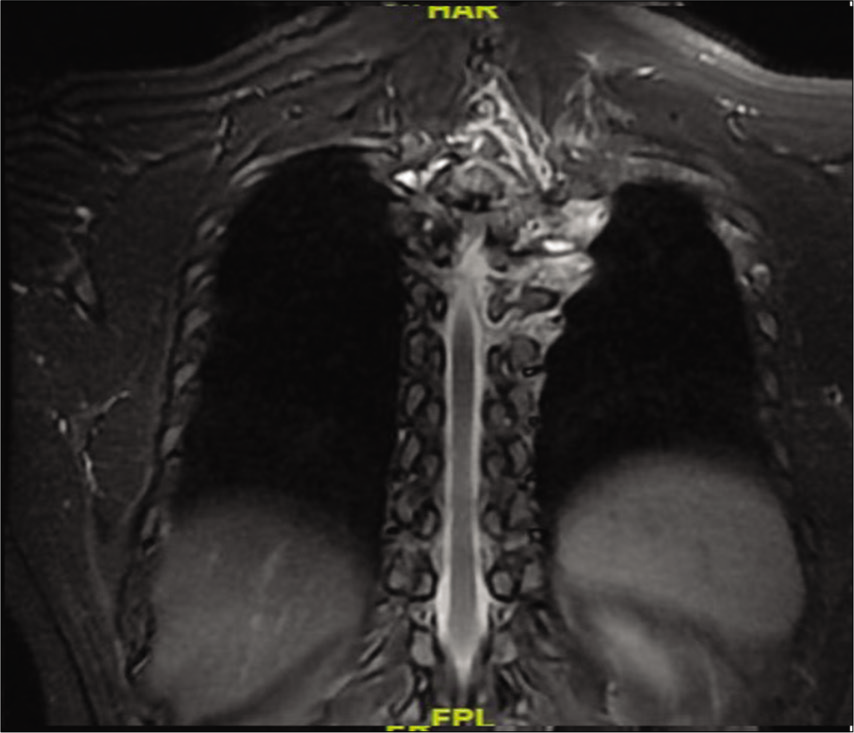
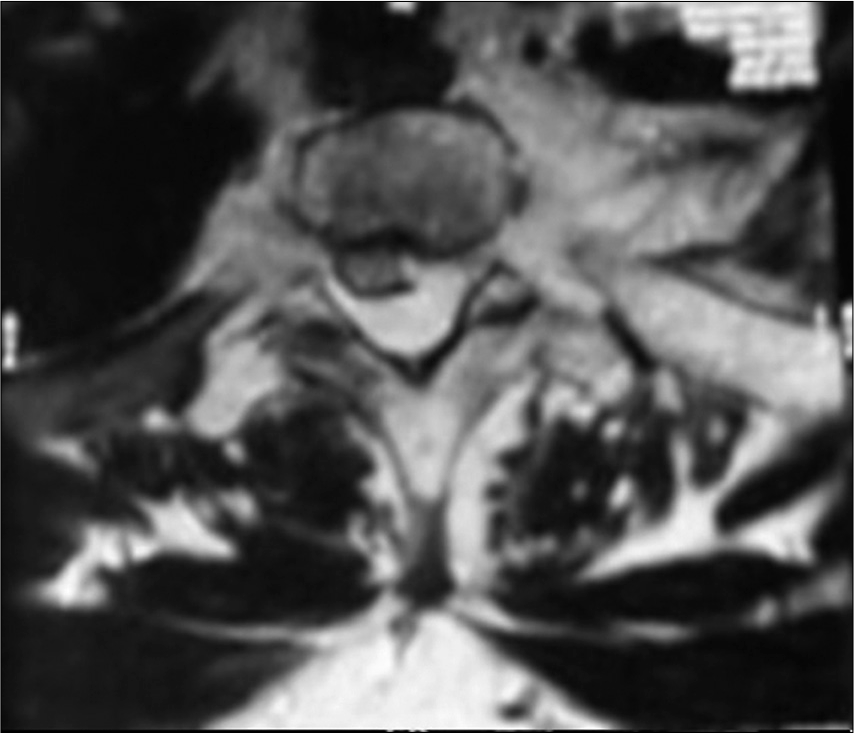
MR findings
On the MR, tumor was hypointense on both T1W and T2W images and enhanced with contrast (i.e., encasing the cervicodorsal spinal cord from C7 to D8 with transforaminal extension). There was also a subtle increased intracord T2W hyperintensities seen at the D2-D3 vertebral levels [
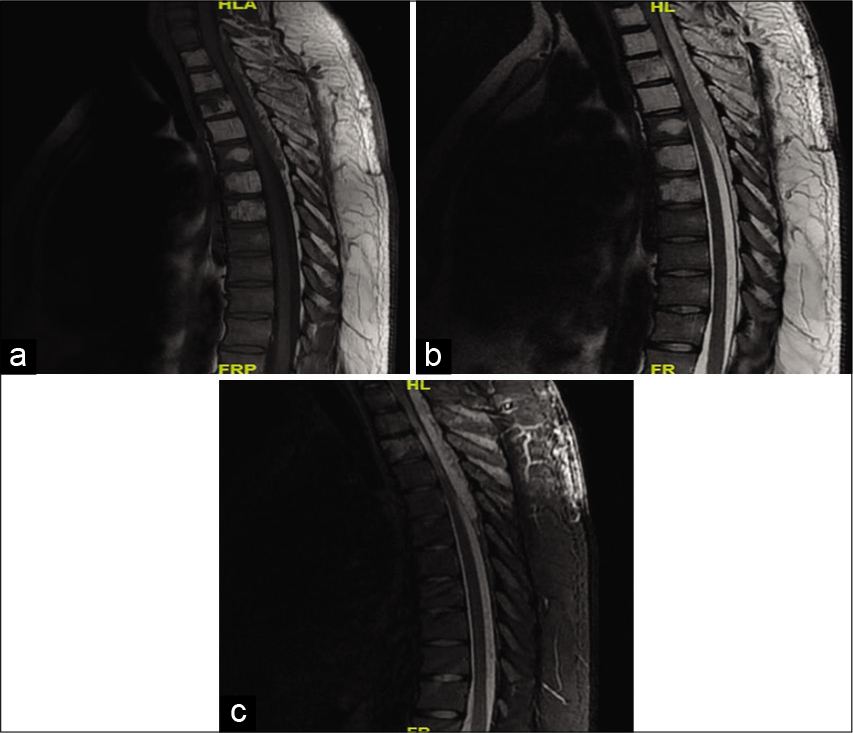
Figure 3:
MRI dorsal spine Sagittal view (a) T1W image (b) T2W image (c) STIR image showing altered bone marrow signal intensity involving D1–D7 vertebrae appearing hypointense on both T1W and T2W images with contiguous involvement of posterior element. Patchy residual normal bone marrow signal noted in D1–D7 vertebrae. Extra dural/epidural lesion arising from C7 to D8 vertebrae appearing hypointense on T1W and hyperintense on T2W/STIR causing significant mass effect on cervicodorsal spinal cord. Intracord T2W/STIR hyperintense signal at D2–D3 level.
Thoracic CT angiography (CTA) with embolization
The Thoracic CTA showed a highly vascular lesion extending from D1 to D7 that was mostly left-sided (i.e. extra and intracanalicular tumor), the major feeders were embolized before surgery (i.e., with gel foam and coils).
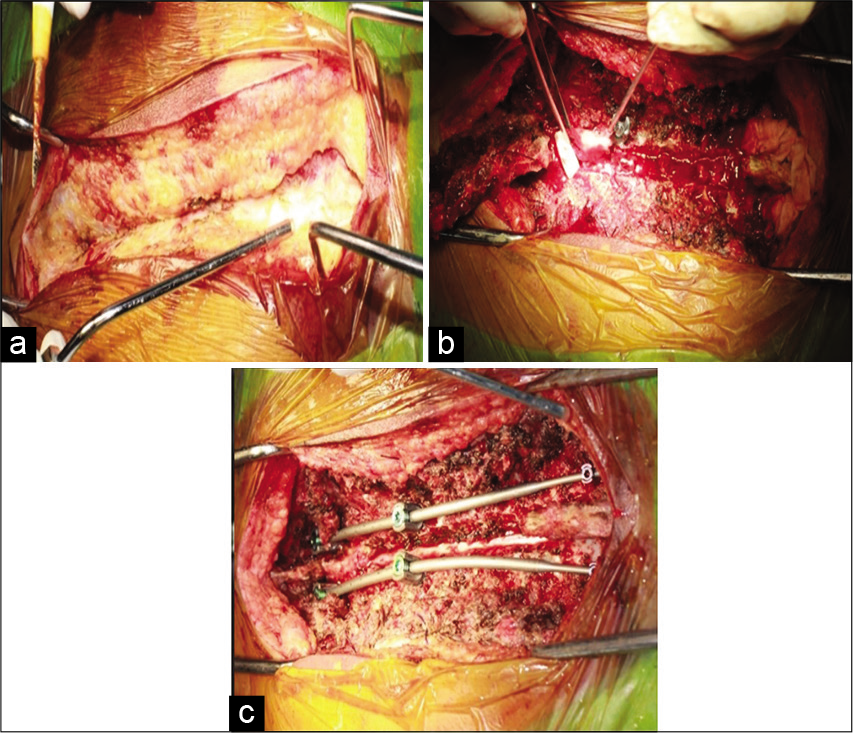
Surgery
Following a D1–D7 laminectomy, a red brown, soft lesion was encountered a leash of blood vessels. Tumor was adherent to the dorsal thecal sac and demonstrated lateral, foraminal, and left-sided paraspinal extension [
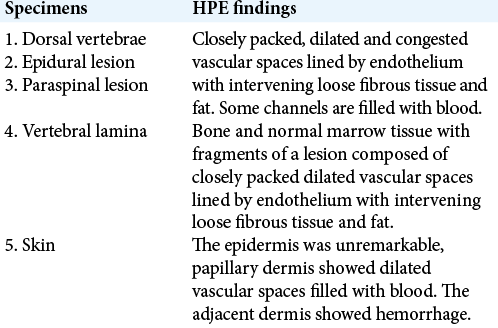
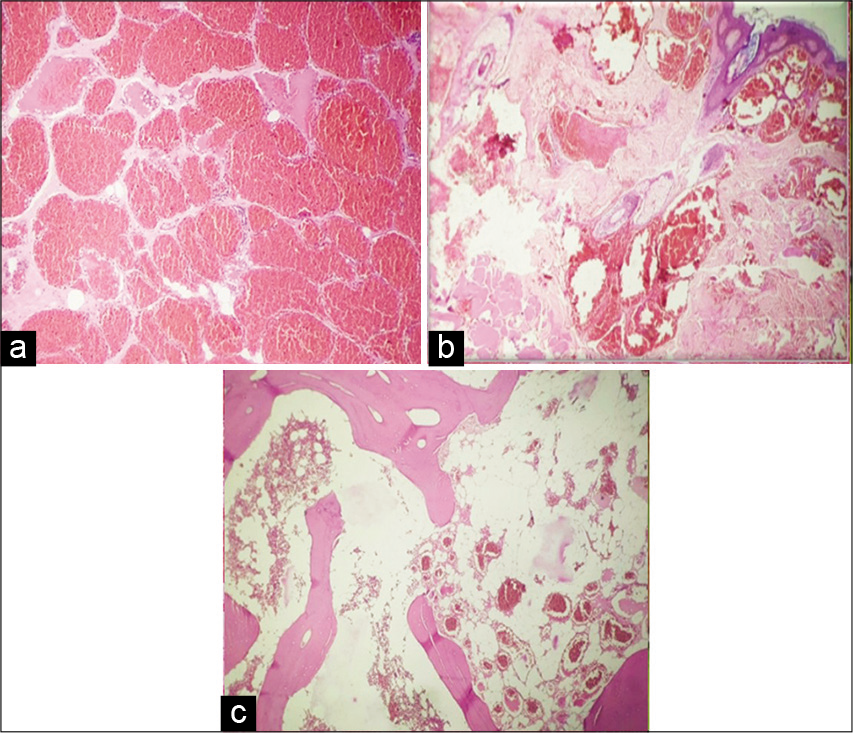
Pathology
The frozen sections (i.e., from the epidural, lamina, paraspinal, and skin) were all consistent with a cavernous hemangioma [
Postoperative recovery
The patient had an uneventful recovery; 1 week later, at discharge, he had improved and was able to ambulate without weakness. Two months later his muscle strength was 5/5 bilaterally.
Postoperative adjunctive radiation therapy
The patient underwent postoperative radiotherapy to the tumor bed to treat surgically inaccessible tumor, and limit the chance of recurrence.
DISCUSSION
According to the WHO classification, vertebral hemangiomas are considered to a be a benign vasoformative neoplasms of bone.[
In the case, we presented, the patient has a congenital cutaneous hemangioma at same levels as the vertebral/epidural tumor sites. Whereas, some literature describes case with concomitant occurrence of haemangiomas in other organs like liver and spleen in association with spinal haemangioma.[
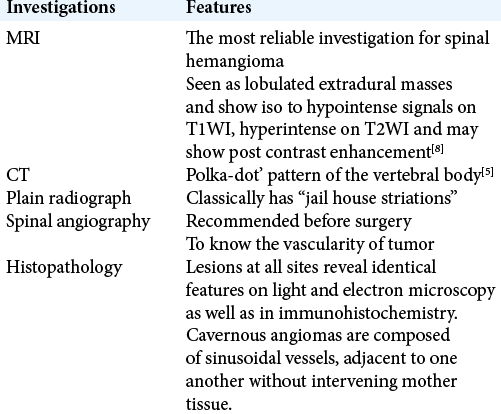
MR imaging is the most reliable investigation for spinal hemangioma [
CONCLUSION
MVH with epidural extension plus congenital cutaneous lesions rarely occur simultaneously at the same levels. In the presence of compression, gross total excision of tumor is optimal, but subtotal removals may be followed by adjunctive radiation therapy to limit the chance of tumor recurrence.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Acosta FL, Dowd CF, Chin C, Tihan T, Ames CP, Weinstein PR. Current treatment strategies and outcomes in the management of symptomatic vertebral hemangiomas. Neurosurgery. 2006. 58: 287-95
2. Fletcher CD, Unni KK, Mertens F.editors. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon, France: IARC Press; 2002. p.
3. Guthkelch AN. Haemangiomas involving the spinal epidural space. J Neurol Neurosurg Psychiatry. 1948. 11: 199-210
4. Johnston LM. Epidural hemangioma with compression of spinal cord. J Am Med Assoc. 1938. 110: 119-22
5. Kan CH, Saw CB, Rozaini R, Fauziah K, Ng CM, Saffari MH. Bilateral epidural extension of thoracic capillary vertebral (intraosseous) hemangioma mimicking spinal meningioma. Med J Malaysia. 2008. 63: 154-6
6. Rodallec MH, Feydy A, Larousserie F, Anract P, Campagna R, Babinet A. Diagnostic imaging of solitary tumors of the spine: What to do and say. Radiographics. 2008. 28: 1019-41
7. Ropper AE, Cahill KS, Hanna JW, McCarthy EF, Gokaslan ZL, Chi JH. Primary vertebral tumors: A review of epidemiologic, histological, and imaging findings, Part I: Benign tumors. Neurosurgery. 2011. 69: 1171-80
8. Sharma MS, Borkar SA, Kumar A, Sharma MC, Sharma BS, Mahapatra AK. Thoracic extraosseous, epidural, cavernous hemangioma: Case report and review of literature. J Neurosci Rural Pract. 2013. 4: 309-12

