

- Seattle Science Foundation, Seattle, Washington, USA
- Department of Anatomic Sciences, St. George's University School of Medicine, St. George's, Grenada
- Goodman Campbell Brain and Spine, Department of Neurological Surgery, Indiana University School of Medicine, Indianapolis, Indiana, USA
Correspondence Address:
Aaron A. Cohen-Gadol
Goodman Campbell Brain and Spine, Department of Neurological Surgery, Indiana University School of Medicine, Indianapolis, Indiana, USA
DOI:10.4103/sni.sni_446_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: R. Shane Tubbs, Marios Loukas, Nicholas M. Barbaro, Kushal J. Shah, Aaron A. Cohen-Gadol. External cortical landmarks for localization of the hippocampus: Application for temporal lobectomy and amygdalohippocampectomy. 22-Aug-2018;9:171
How to cite this URL: R. Shane Tubbs, Marios Loukas, Nicholas M. Barbaro, Kushal J. Shah, Aaron A. Cohen-Gadol. External cortical landmarks for localization of the hippocampus: Application for temporal lobectomy and amygdalohippocampectomy. 22-Aug-2018;9:171. Available from: http://surgicalneurologyint.com/surgicalint-articles/external-cortical-landmarks-for-localization-of-the-hippocampus-application-for-temporal-lobectomy-and-amygdalohippocampectomy/
Date of Submission
27-Nov-2017
Date of Acceptance
20-Jun-2018
Date of Web Publication
22-Aug-2018
Abstract
Background:Accessing the hippocampus for amygdalohippocampectomy and minimally invasive procedures, such as depth electrode placement, require an accurate knowledge regarding the location of the hippocampus.
Methods:The authors removed 10 human cadaveric brains from the cranium and observed the relationships between the lateral temporal neocortex and the underlying hippocampus. They then measured the distance between the hippocampus and superficial landmarks. The authors also validated their study using magnetic resonance imaging (MRI) scans of 10 patients suffering from medial temporal lobe sclerosis where the distance from the hippocampal head to the anterior temporal tip was measured.
Results:In general, the length of the hippocampus was along the inferior temporal sulcus and inferior aspect of the middle temporal gyrus. Although the hippocampus tended to be more superiorly located in female specimens and on the left side, this did not reach statistical significance. The length of the hippocampus tended to be shorter in females, but this too failed to reach statistical significance. The mean distance from the anterior temporal tip to the hippocampal head was identical in the cadavers and MRIs of patients with medial temporal lobe sclerosis.
Conclusions:Additional landmarks for localizing the underlying hippocampus may be helpful in temporal lobe surgery. Based on this study, there are relatively constant anatomical landmarks between the hippocampus and overlying temporal cortex. Such landmarks may be used in localizing the hippocampus during amygdalohippocampectomy and depth electrode implantation in verifying the accuracy of image-guided methods and as adjuvant methodologies when these latter technologies are not used or are unavailable.
Keywords: Anatomy, epilepsy surgery, hippocampectomy, landmarks, neurosurgery, temporal lobe
INTRODUCTION
Even with advancements in the pharmacological treatment of epilepsy, there is still a group of patients whose seizures have a higher tendency to be refractory to medical therapy. Medial temporal lobe epilepsy is often caused by medial temporal lobe sclerosis or lesional epileptogenic foci within the amygdala and hippocampal formation. The hippocampus and surrounding formation are made up of the cornu ammonis (hippocampus proper), subiculum, dentate gyrus, supracallosal gyrus, alveus, fimbria, and fornix.[
Anterior temporal lobectomy with amygdalohippocampectomy has proven efficacious for cessation of intractable seizures of medial temporal lobe origin. Aggressive resection of these medial temporal lobe structures has been associated with improved surgical outcomes.[
MATERIALS AND METHODS
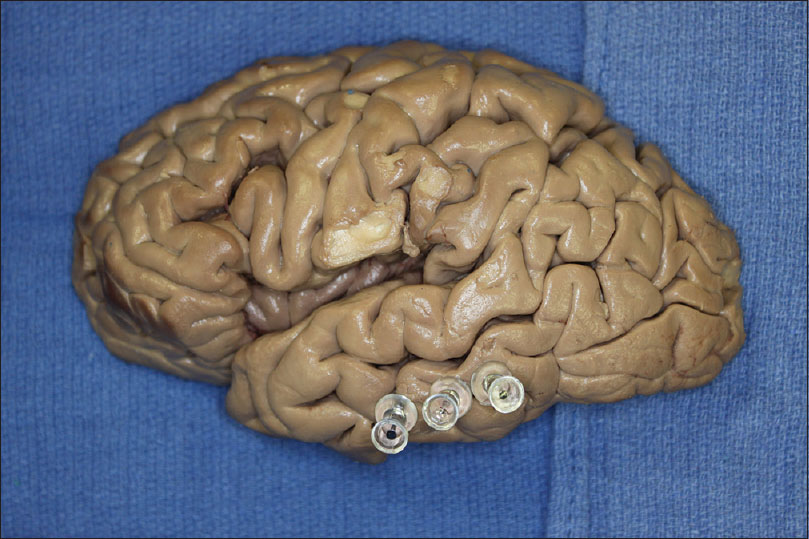
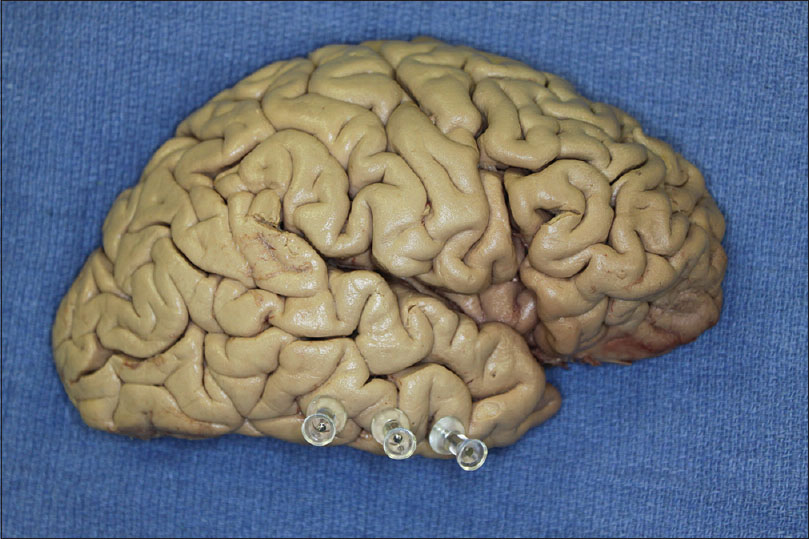
Ten formalin-fixed cadaveric brains (20 hemispheres) were removed from the craniums. The specimens were derived from 6 male and 4 female cadavers aged 35 to 75 years (mean 65 years) at death. Brains were next hemisected in the midline and the fornix identified and followed toward the left and right hippocampus. Once the hippocampus was isolated from a mesial approach, 6-cm long straight needles were placed into its head, tail, and the midpoint between these structures, and passed laterally in the axial plane until they reached the cortical surface. The specimens were then turned and pin exit sites were marked externally using smaller pins [Figures

The authors also validated their study using magnetic resonance imaging (MRI) scans of 10 patients suffering from medial temporal lobe sclerosis. Axial, coronal, and sagittal MRI scans were used to localize the head of the hippocampus on the affected side based on superficial landmarks. Reference lines from the PACS (Picture Archiving and Communication System) software allowed localization of the head of the hippocampus on the sagittal series where the distance from the anterior temporal tip to the head of the hippocampus was measured and recorded.
RESULTS
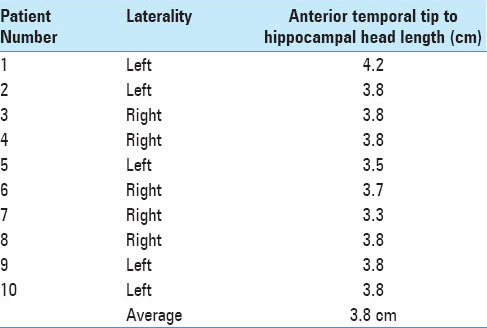
We did not observe any gross intracranial pathology or evidence of previous surgery in any specimen. The distance from the tip of the temporal lobe to the headof the hippocampus ranged from 3.5 to 4.3 cm (mean 3.8 cm) [Figures

In two right-sided specimens, the tail was deep to the superior temporal sulcus [
MRI scans of patients suffering from medial temporal lobe sclerosis were evaluated and the distance from the hippocampal head to the anterior temporal tip was recorded on the sagittal axis. The lengths varied from 3.3 cm to 4.2 cm (mean, 3.8 cm) [
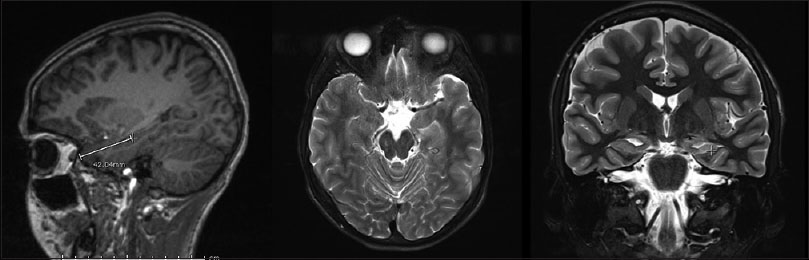
Figure 7
Sagittal, axial, and coronal sequences were used to identify the anatomical landmarks. Using the IntelliLink tool, the hippocampal head was marked on the axial plane and that position was identified on the sagittal plane. A measurement was taken from the anterior temporal tip to the hippocampal head and recorded
DISCUSSION
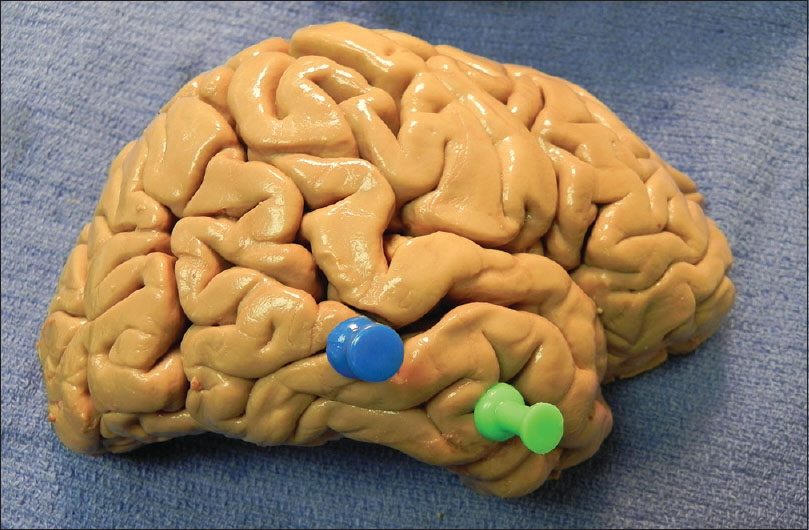
Localization of the hippocampus in relation to superficial structures is important for exposing the hippocampus during anteromedial temporal lobectomy and amygdalohippocampectomy procedures while minimizing the extent of neocortical resection, especially on the dominant hemisphere. Furthermore, intraoperative depth electrodes placed within the hippocampus can provide useful information regarding the relative epileptogenecity of this medial structure versus the temporal neocortex. Therefore, it is important to localize the hippocampus as accurately as possible using all the available data, including image guidance and surface landmarks. In our study, we found that the inferior temporal sulcus and middle temporal gyrus were relatively constant landmarks to the underlying hippocampus. In addition, and within approximately a centimeter, the length of the hippocampus was similar in length between sides and genders.
Surgical anatomy
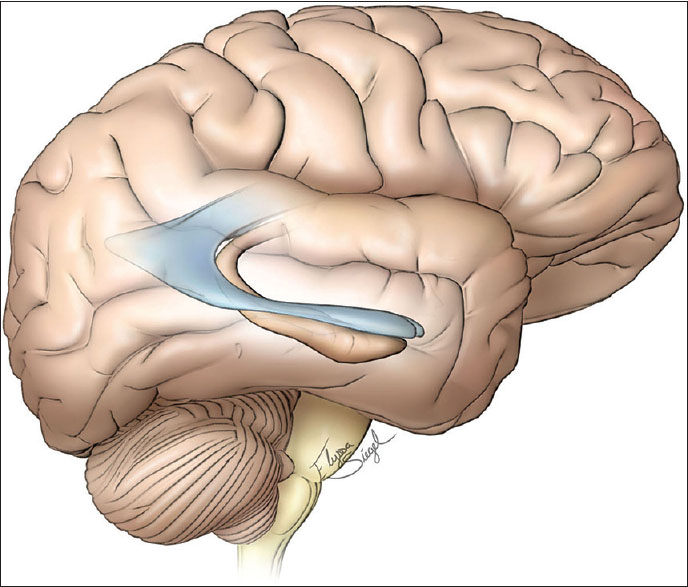
The hippocampus sits in the medial part of the temporal lobe and on the floor of the temporal horn of the lateral ventricle. The amygdala is situated anterior and superior to the head of the hippocampus. The uncus, which is part of the entorhinal cortex, wraps around the inferior border of the hippocampus and appears as a continuous homogeneous ovoid mass with the amygdala on MRI.[
Applications for selective amygdalohippocampectomy and depth electrode placement
The data presented about the localization of the head of the hippocampus 3–4 cm from the anterior temporal tip may have important implications regarding the extent of temporal neocortical resection necessary to perform an amygdalohippocampectomy. Based on the above data, a 3–4 cm anteromedial temporal neocortical resection will be adequate to expose the anterior aspect of the hippocampus. If a localized lesion is present along this anterior region, further neocortical resection will not be necessary. However, if an extensive hippocampectomy for medial temporal lobe sclerosis is contemplated, disconnection of the occipitotemporal fasciculus along the lateral aspect of the hippocampus will allow lateral mobilization of the temporal cortex (instead of its resection) to provide enough exposure to allow for a posterior hippocampectomy [
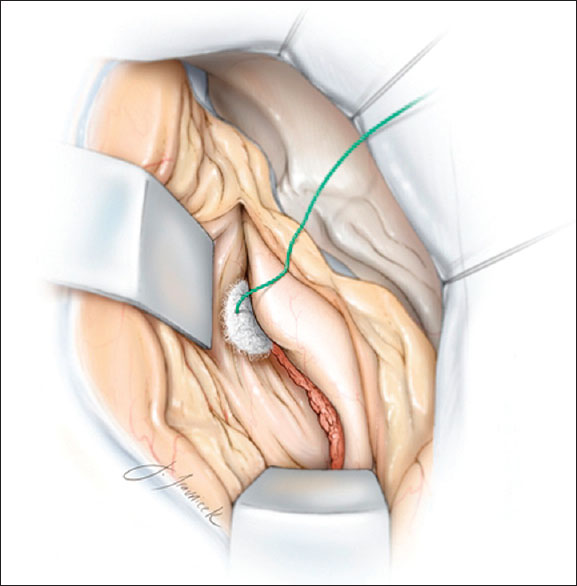
Figure 8
Disconnection of the occipitotemporal fasciculus along the lateral aspect of the hippocampus will allow lateral mobilization the temporal cortex (instead of its resection), to provide enough exposure to allow for a posterior hippocampectomy. A corticotomy within the middle temporal gyrus, along the mid portion of the temporal lobe, will expose the ventricle. Copyright, The Neurosurgical Atlas, used with permission
In a study by Davies et al.,[
CONCLUSIONS
We performed the above cadaveric study to better identify the relationships between the outer temporal cortex and the deeper lying hippocampus. Such landmarks may be useful to neurosurgeons in localizing the hippocampus in conjunction with or to verify imaged-guided technologies or when these devices are not used or are unavailable.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ayberk G, Yagli OE, Comert A, Esmer AF, Canturk N, Tekdemir I. Anatomic relationship between the anterior sylvian point and the pars triangularis. Clin Anat. 2012. 25: 429-36
2. Bronen RA, Cheung G. Relationship of hippocampus and amygdala to coronal MRI landmarks. Magn Reson Imaging. 1991. 9: 449-57
3. Davies KG, Phillips BLB, Hermann BP. MRI confirmation of accuracy of freehand placement of mesial temporal lobe depth electrodes in the investigation of intractable epilepsy. Br J Neurosurg. 1996. 10: 175-8
4. Duvernoy HM, Cattin F, Naidich TP, Fatterpekar G, Raybaud C, Risold PY.editors. The Human Hippocampus. Berlin Heidelberg: Springer-Verlag; 2005. p.
5. Naidich TP, Daniels DL, Haughton VM, Williams A, Pojunas K, Palacios E. Hippocampal formation and related structures of the limbic lobe: Anatomic-MR correlation. Part 1. Surface features and coronal sections. Radiology. 1987. 162: 747-54
6. Siadat MR, Soltanian-Zadeh H, Elisevich KV. Knowledge-based localization of hippocampus in human brain MRI. Comput Biol Med. 2007. 37: 1342-60
7. Sindou M, Guenot M. Surgical anatomy of the temporal lobe for epilepsy surgery. Adv Tech Stand Neurosurg. 2003. 28: 315-43
8. Van Gompel JJ, Meyer FB, Marsh WR, Lee KH, Worrell GA. Stereotactic electroencephalography with temporal grid and mesial temporal depth electrode coverage: Does technique of depth electrode placement affect outcome?. J Neurosurg. 2010. 113: 32-8
9. Wen HT, Rhoton AL, de Oliverira E, Cardoso ACC, Tedeschi H, Baccanelli M. Microsurgical anatomy of the temporal lobe: Part 1: Mesial temporal lobe anatomy and its vascular relationships as applied to amygdalohippocampectomy. Neurosurgery. 1990. 45: 549-92
10. Wyler AR, Hermann BP, Somes G. Extent of medial temporal resection on outcome from anterior temporal lobectomy: A randomized prospective study. Neurosurgery. 1995. 37: 982-90

