

- Department of Neurosurgery, The Jikei University School of Medicine, Minato-Ku, Tokyo, Japan.
DOI:10.25259/SNI_858_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Toshihiro Ishibashi, Fumiaki Maruyama, Issei Kan, Tohru sano, Yuichi Murayama. Four-dimensional digital subtraction angiography for exploration of intraosseous arteriovenous fistula in the sphenoid bone. 02-Mar-2021;12:85
How to cite this URL: Toshihiro Ishibashi, Fumiaki Maruyama, Issei Kan, Tohru sano, Yuichi Murayama. Four-dimensional digital subtraction angiography for exploration of intraosseous arteriovenous fistula in the sphenoid bone. 02-Mar-2021;12:85. Available from: https://surgicalneurologyint.com/surgicalint-articles/four-dimensional-digital-subtraction-angiography-for-exploration-of-intraosseous-arteriovenous-fistula-in-the-sphenoid-bone/
Date of Submission
30-Nov-2020
Date of Acceptance
08-Jan-2021
Date of Web Publication
02-Mar-2021
Abstract
Background: Intraosseous arteriovenous fistula (AVF) is a rare clinical entity that typically presents with symptoms from their effect on surrounding structures. Here, we report a case of intraosseous AVF in the sphenoid bone that presented with bilateral abducens palsy.
Case Description: A previously healthy man presented with tinnitus for 1 month, and initial imaging suspected dural AVF of the cavernous sinus. Four-dimensional digital subtraction angiography (4D-DSA) imaging and a three-dimensional (3D) fused image from the bilateral external carotid arteries revealed that the shunt was in a large venous pouch within the sphenoid bone that was treated through transvenous coil embolization. His symptoms improved the day after surgery.
Conclusion: This is a case presentation of intraosseous AVF in the sphenoid bone and highlights the importance of 4D-DSA and 3D fused images for planning the treatment strategy.
Keywords: Dural arteriovenous fistula, Four-dimensional digital subtraction angiography, Intraosseous, Neuroendovascular, Sphenoid bone
INTRODUCTION
Arteriovenous fistulas (AVFs) in the cavernous sinus (CS) are often caused by venous pouches in various locations. Recently, intraosseous shunts have been reported to be the cause of AVF. We report a case of an AVF with an intraosseous shunt in the sphenoid bone, in which preoperative four-dimensional digital subtraction angiography (4D-DSA) and three-dimensional (3D) fused images were a useful treatment modality.
CASE PRESENTATION
A patient presented with tinnitus for 1 month and was referred to an ophthalmology clinic with a complaint of diplopia 7 days prior. Bilateral abducens nerve palsy was diagnosed on examination. Brain magnetic resonance imaging (MRI) showed an abnormal high intensity lesion within the sphenoid bone connected to the bilateral CS. This suggested a CS dural AVF (DAVF).
Cerebral angiography revealed an AVF with a shunt from the right external carotid artery (ECA) and the left ECA in the CS. The bilateral internal maxillary artery (IMA), accessory middle meningeal arteries, deep temporal arteries, and left ascending pharyngeal artery are the feeding arteries from the bilateral ECAs. The shunt flow was from the right ECA branches draining into the venous pouch and into the bilateral CS, then to the bilateral inferior petrosal sinus (IPS). Bilateral CS is the drainage route, which drains into the right superficial middle cerebral vein and intradurally to the right basal vein. Some of the venous drainage refluxed into the superior sagittal sinus [
Video 1
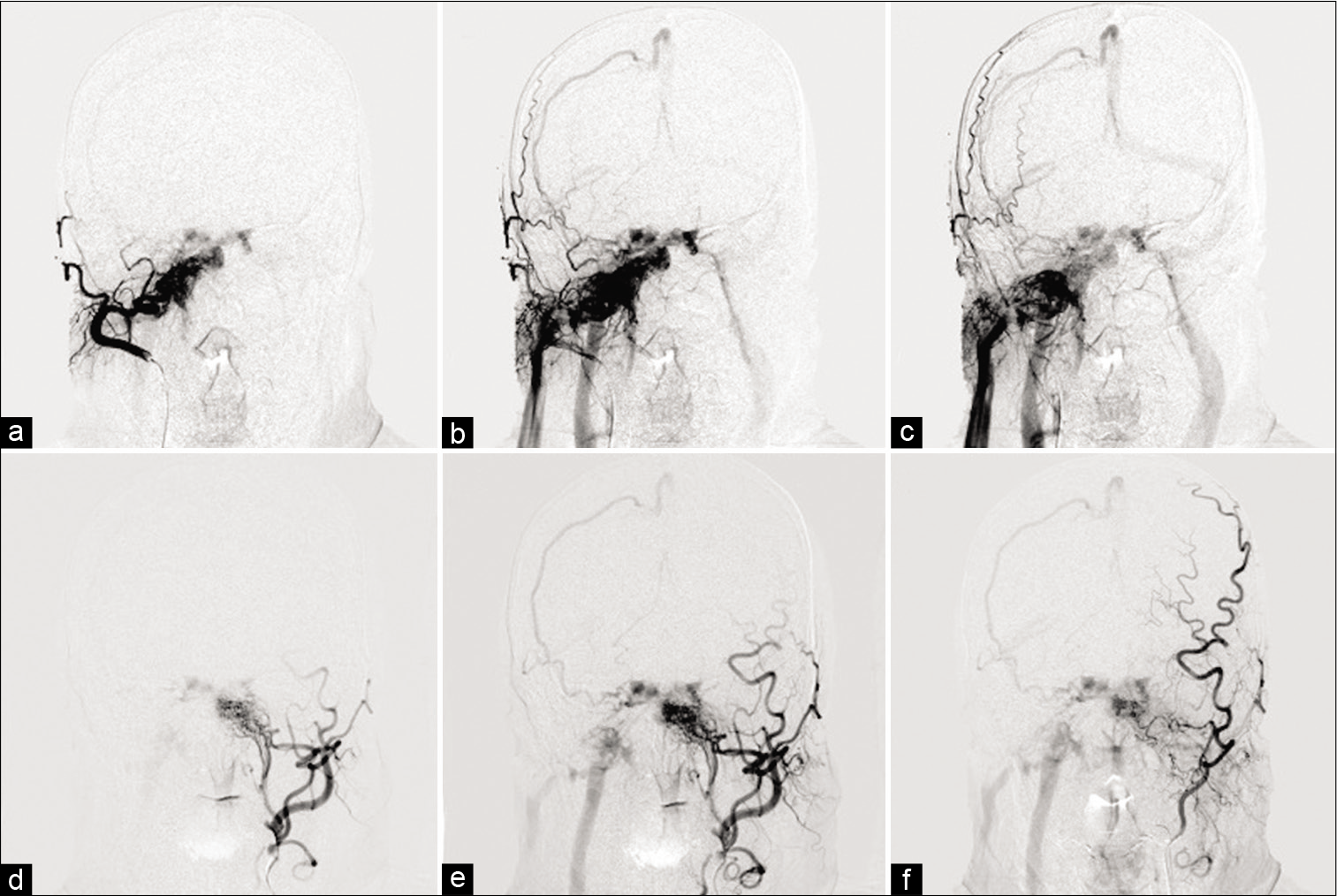
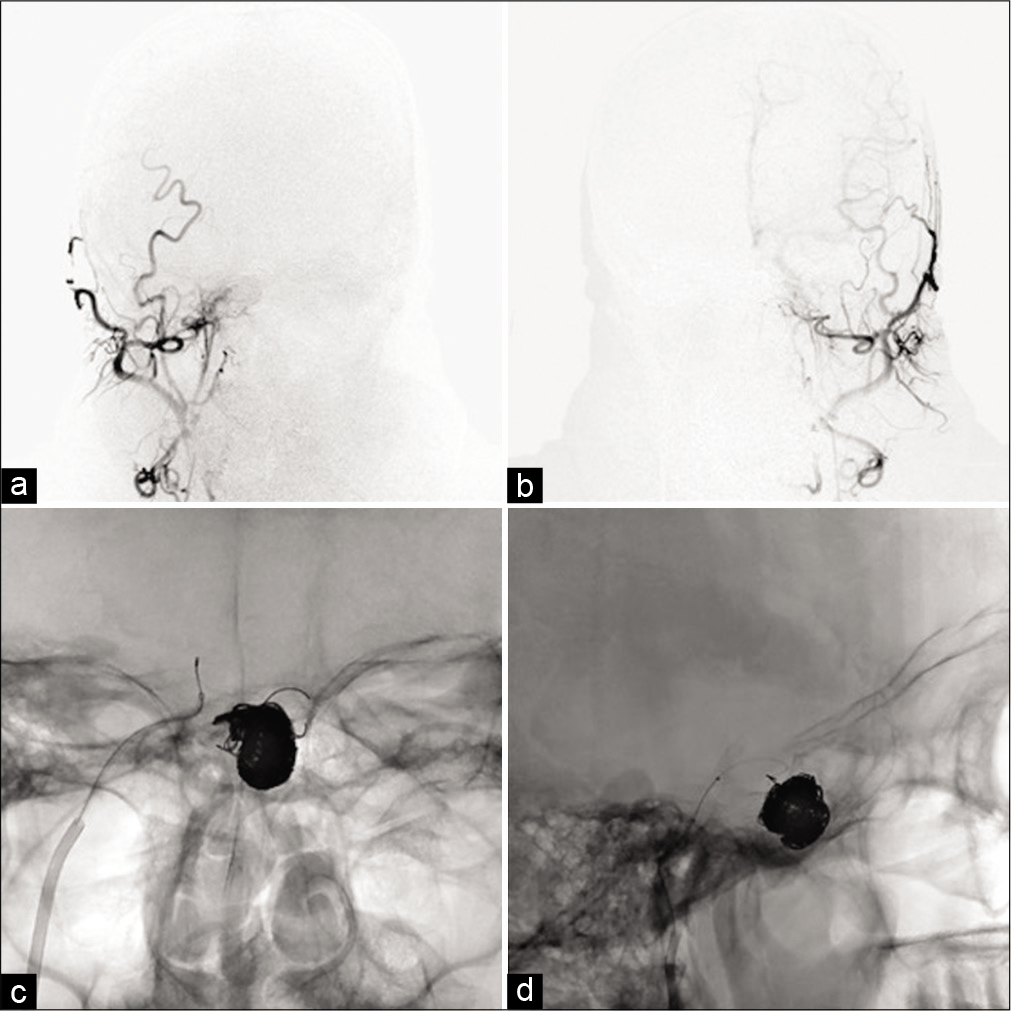
Figure 1:
Conventional angiograms from the right external carotid artery (ECA) (a,b,c) and the left ECA (d,e,f) showing a cavernous sinus arteriovenous fistula. The shunt flow from the bilateral ECA branches drain into the bilateral cavernous sinus and into the right superficial middle cerebral vein.
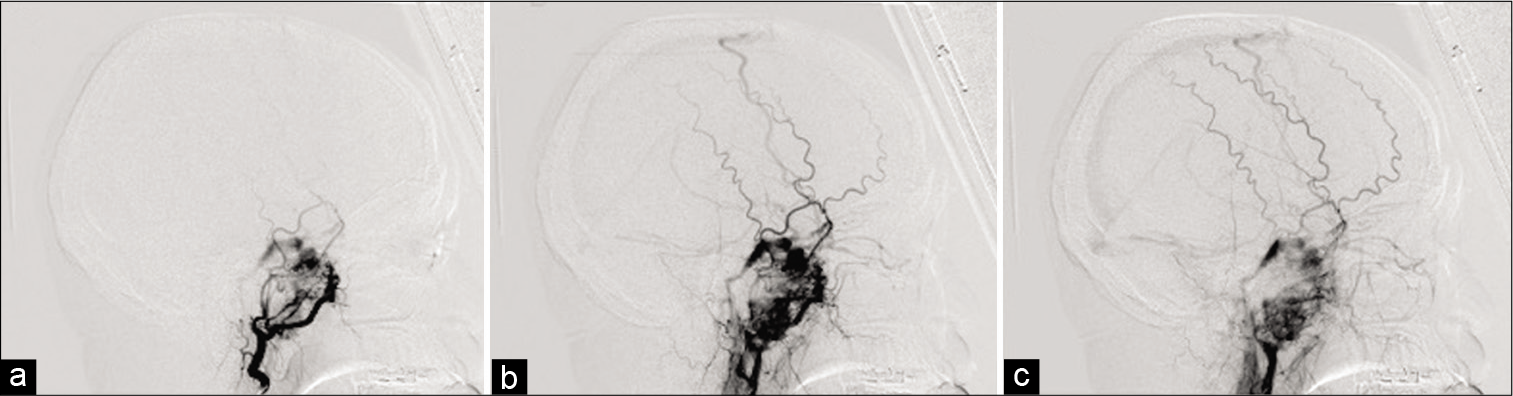
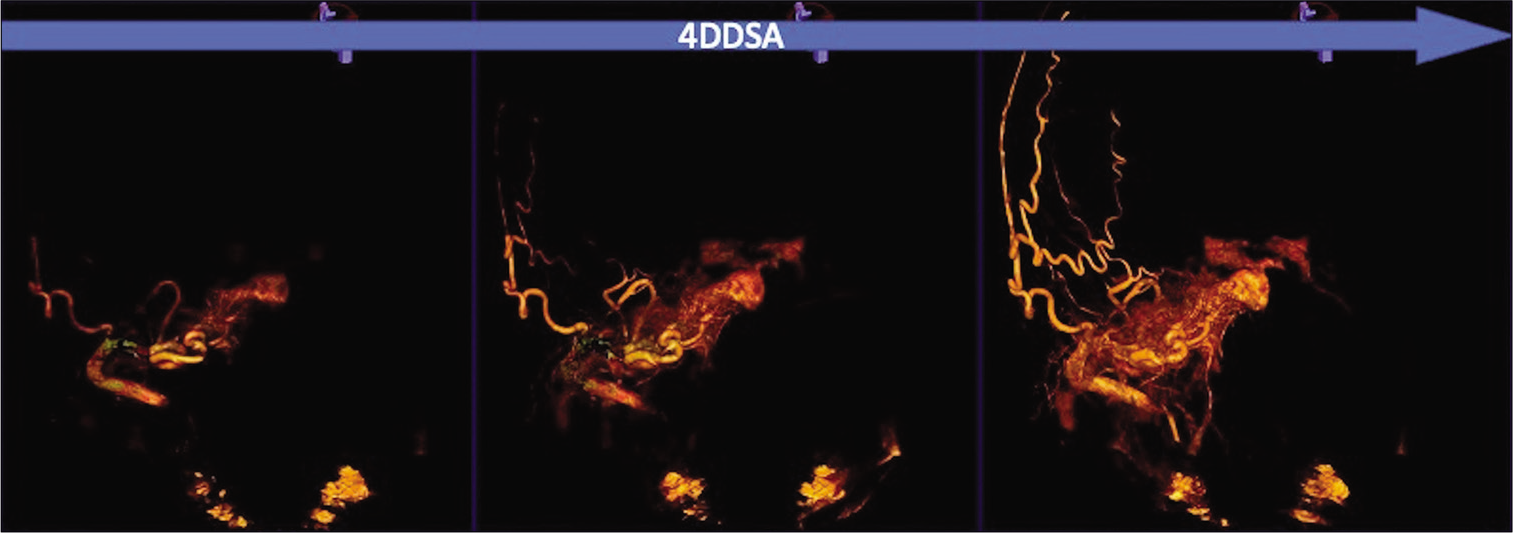
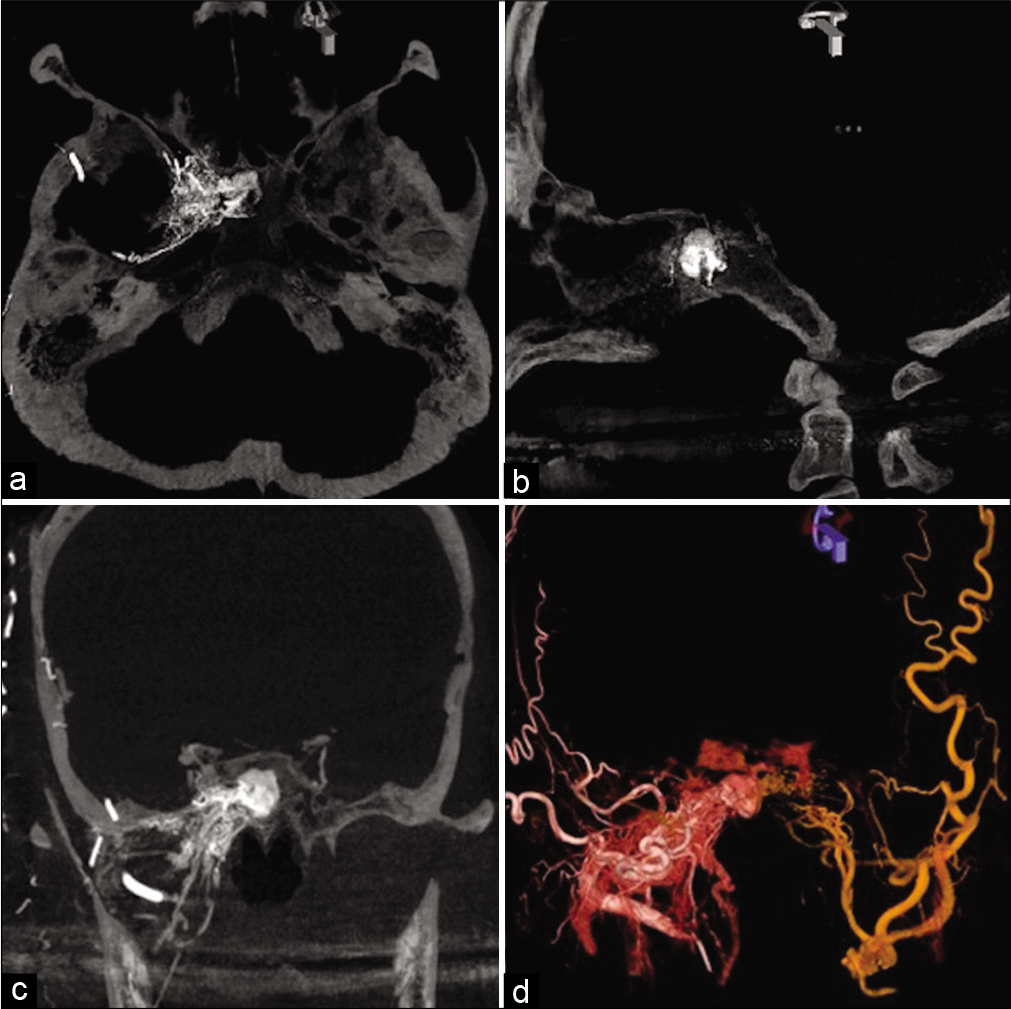
Figure 4:
Slab maximum intensity projection images (axial (a), sagittal (b), and coronal (c) views) of the right external carotid artery (ECA) angiogram revealed that the arteriovenous fistula was in the sphenoid bone. The three-dimensional fused image from bilateral ECAs (right ECA, orange; left ECA, pink) also showing that the venous pouch was fed by bilateral ECAs. The three-dimensional (3D) fused image from bilateral ECAs (right ECA, orange; left ECA, pink) also showing that the venous pouch was fed by bilateral ECAs (d).
4D-DSA
The images were acquired using commercially available biplane angiography systems equipped with 1920 × 2480 cesium iodide-amorphous silicon flat panel detectors covering an area of approximately 30 × 40 cm (Artis Q biplane and Artis Zee biplane; Siemens Healthcare GmbH, Forchheim, Germany). The patients underwent cerebral angiography using standard techniques. During 4D-DSA image acquisition, two rotational angiography scans were performed; a native mask run followed by a contrast-enhanced fill run with the injection of undiluted contrast medium (Iohexol 300 mg/mL, IOPAQUE; Fuji Pharma Co., Ltd., Tokyo, Japan). The protocol acquired 304 projections over a 260° rotation in 12 s. A power injector was used to inject contrast medium from a guiding catheter placed in the target artery. Undiluted contrast medium was injected with an injection rate of 3.0 mL/s with no X-ray delay, and the injection time was 7 s for 12 s 4D-DSA. Datasets were transferred to a workstation (syngo X- Workplace, Siemens Healthcare GmbH, Forchheim, Germany) for post processing where 4D-DSA images were created and appropriate Volume rendering present was selected for optimal visualization of the vasculature. To better visualize the vasculature relative to the bony structure, fusion images of 4D-DSA and 3D images of the skull from the mask run were generated by the workstation’s application (syngo Dual Volume, Siemens Health- care GmbH, Forchheim, Germany). The radiation dose was extracted from the dose reports automatically generated by the angiography systems and the volume of contrast medium used for 12 s 4D-DSA was retrieved from the medical records of the patients.
Treatment
Under general anesthesia, transvenous coil embolization of the DAVF was performed. A 6-French guiding catheter was navigated to the right internal jugular vein and a 5-French diagnostic catheter was placed into the left ascending pharyngeal artery. A 3.2-F intermediate catheter (TACTICS; Technocrat Corporation, Aichi, Japan) was used for supporting the microcatheter (SL10; Stryker, Kalamazoo, MI). The microcatheter with micro-guidewire (CHIKAI 0.014 inch Asahi Intecc) was advanced into the right CS through the right IPS. To confirm the location of the tip of the microcatheter, C-arm cone-beam computed tomography equipment (Artis Q biplane and Artis Q biplane; Siemens Healthcare GmbH, Forchheim, Germany) images were taken while the microcatheter was filled with contrast medium. A microcatheter in the venous sac was identified by a fusion of that image and a 3D DSA image of the left ECA [
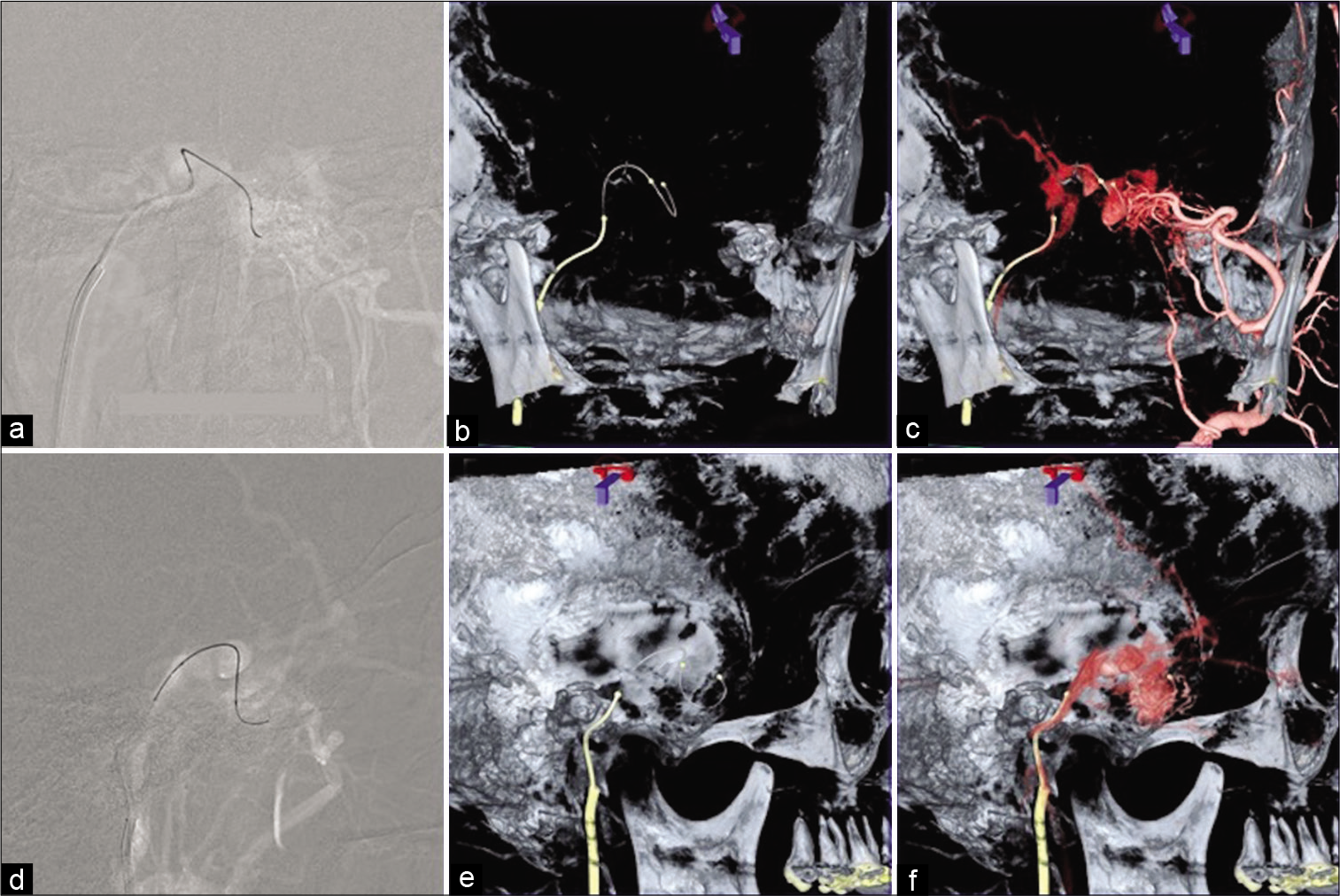
Figure 5:
Transvenous approach with positioning of the microcatheter into the venous pouch. A microcatheter in the venous sac was identified by digital subtraction angiography (DSA) road map image (a and d), Dyna computed tomography (CT) image (b and e) and fusion images Dyna CT and three-dimensional-DSA image of the left external carotid artery (c and f).
Outcome and follow-up
Bilateral ECA angiogram showed that the shunt had disappeared [
DISCUSSION
We report a case of intraosseous CS AVF in which the venous pouch was in the sphenoid bone. The most frequent location of the shunted pouch is the posterior part of CS.[
4D-DSA and 3D-DSA fusion images were useful in planning therapeutic strategies.
4D-DSA is a new imaging algorithm that provides time-resolved 3D DSA through a single acquisition in the AngioSuite.[
3D-DSA fusion images are also a useful imaging technique for treatment planning in intracranial vascular diseases involving multiple vessels.[
Transvenous endovascular approaches have been described to treat intraosseous AVF.[
CONCLUSION
This is a case presentation of intraosseous AVF in the sphenoid bone and highlights the importance of 4D-DSA and 3D fused images for planning the treatment strategy.
Ethics approval statements
The study was approved by the institutional review board (IRB) (29-228[8844]).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
Yuichi Murayama—UNRELATED for this article: Consultancy: Stryker, Kaneka Medix; Grants/Grants Pending: Stryker, Siemens K.K., Japan, Comments: research grant; Payment for Lectures Including Service on Speakers Bureaus: Stryker, Cerenovus, Kaneka Medix; Royalties: Stryker. Money paid to the institution.
Video available on:
www.surgicalneurologyint.com
References
1. Davis B, Royalty K, Kowarschik M, Rohkohl C, Oberstar E, Aagaard-Kienitz B. 4D digital subtraction angiography: Implementation and demonstration of feasibility. AJNR Am J Neuroradiol. 2013. 34: 1914-21
2. Fukuda K, Higashi T, Okawa M, Iwaasa M, Abe H, Inoue T. Fusion technique using three-dimensional digital subtraction angiography in the evaluation of complex cerebral and spinal vascular malformations. World Neurosurg. 2016. 85: 353-8
3. Hiramatsu M, Sugiu K, Haruma J, Hishikawa T, Takahashi Y, Murai S. Osseous arteriovenous fistulas in the dorsum sellae, clivus, and condyle. Neuroradiology. 2021. 63: 133-40
4. Jung C, Kwon BJ, Kwon OK, Baik SK, Han MH, Kim JE. Intraosseous cranial dural arteriovenous fistula treated with transvenous embolization. AJNR Am J Neuroradiol. 2009. 30: 1173-7
5. Kannath SK, Rajan JE, Sarma SP. Anatomical localization of the cavernous sinus dural fistula by 3D rotational angiography with emphasis on clinical and therapeutic implications. J Neuroradiol. 2017. 44: 326-32
6. Kato N, Yuki I, Hataoka S, Dahmani C, Otani K, Abe Y. 4D digital subtraction angiography for the temporal flow visualization of intracranial aneurysms and vascular malformations. J Stroke Cerebrovasc Dis. 2020. 29: 105327
7. Kiyosue H, Tanoue S, Hori Y, Hongo N, Mori H. Shunted pouches of cavernous sinus Dural AVFs: Evaluation by 3D rotational angiography. Neuroradiology. 2015. 57: 283-90
8. Kobkitsuksakul C, Jiarakongmun P, Chanthanaphak E, Pongpech S. Noncavernous arteriovenous shunts mimicking carotid cavernous fistulae. Diagn Interv Radiol. 2016. 22: 555-9
9. Mohimen A, Kannath SK, Jayadevan ER. Skull base osseous arteriovenous fistula-a rare clinical entity: Case report and literature review. World Neurosurg. 2017. 97: 760.e9-12
10. Park ES, Jung YJ, Yun JH, Ahn JS, Lee DH. Intraosseous arteriovenous malformation of the sphenoid bone presenting with orbital symptoms mimicking cavernous sinus Dural arteriovenous fistula: A case report. J Cerebrovasc Endovasc Neurosurg. 2013. 15: 251-4

