

- Department of Neurological Surgery, Hospital Municipal Miguel Couto, Rua Mario Ribeiro, Brazil,
- Department of Internal Medicine, School of Medicine, Federal University of Rio de Janeiro, R. Prof. Rodolpho Paulo Rocco, Rio de Janeiro, Brazil,
- Department of Neurological Surgery, Vanderbilt University School of Medicine, Nashville, Tennessee, United States.
Correspondence Address:
Caio Perret, Department of Neurological Surgery, Hospital Municipal Miguel Couto, Rua Mario Ribeiro, Rio de Janeiro, Brazil.
DOI:10.25259/SNI_601_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Caio Perret1, Raphael Bertani1, Mauricio Mendes Barbosa2, Savio Batista2, Stefan W. Koester3, Paulo Santa Maria1, Hugo Schiavini1. Hemorrhage due to attempted excision of a frontal exophytic lesion: A cautionary tale. 11-Oct-2021;12:512
How to cite this URL: Caio Perret1, Raphael Bertani1, Mauricio Mendes Barbosa2, Savio Batista2, Stefan W. Koester3, Paulo Santa Maria1, Hugo Schiavini1. Hemorrhage due to attempted excision of a frontal exophytic lesion: A cautionary tale. 11-Oct-2021;12:512. Available from: https://surgicalneurologyint.com/surgicalint-articles/11171/
Date of Submission
15-Jun-2021
Date of Acceptance
08-Sep-2021
Date of Web Publication
11-Oct-2021
Abstract
Background: Despite mainly benign, exophytic subcutaneous cranial masses present with a myriad of differential diagnosis possibilities, ranging from simple, superficial lesions to complex lesions involving the central nervous system. Although the gold standard imaging modality for the diagnosis of these lesions is magnetic resonance imaging, Doppler Ultrasonography can be a useful, inexpensive, and available tool for evaluation of lesions that could potentially be safely treated in the primary care setting, and lesions that would demand advanced neurosurgical care.
Case Description: This patient presented with a complex exophytic plasmocytoma that was first diagnosed and erroneously approached as a subcutaneous lipoma with surgical resection in an outpatient surgical setting. This interpretive approach resulted in the failure of the procedure due to significant hemorrhage. The patient was immediately referred to neurosurgical care and transferred to our center. Admission doppler ultrasound imaging revealed absence of the frontal bone, the enriched and profuse vascularization, allowing further and proper diagnostic approach and treatment.
Conclusion: Ultrasound could be a reliable, fast, and simple imaging method aiding practitioners to perform a better workup for patients with exophytic subcutaneous cranial masses.
Keywords: Forehead subcutaneous mass, Plasmacytoma, Ultrasound in neurosurgery
INTRODUCTION
The term exophytic tumor is used to define masses that expand to the skin’s external surface. Soft subcutaneous tumor differentials are dermoid cysts, hemangiomas, lipomas, epidermal inclusion cysts, and osteomas.[
In certain locations and histological subtypes, these CNS tumors might equally present as soft slow-growing, solitary forehead masses, with no otherwise neurological deficits [
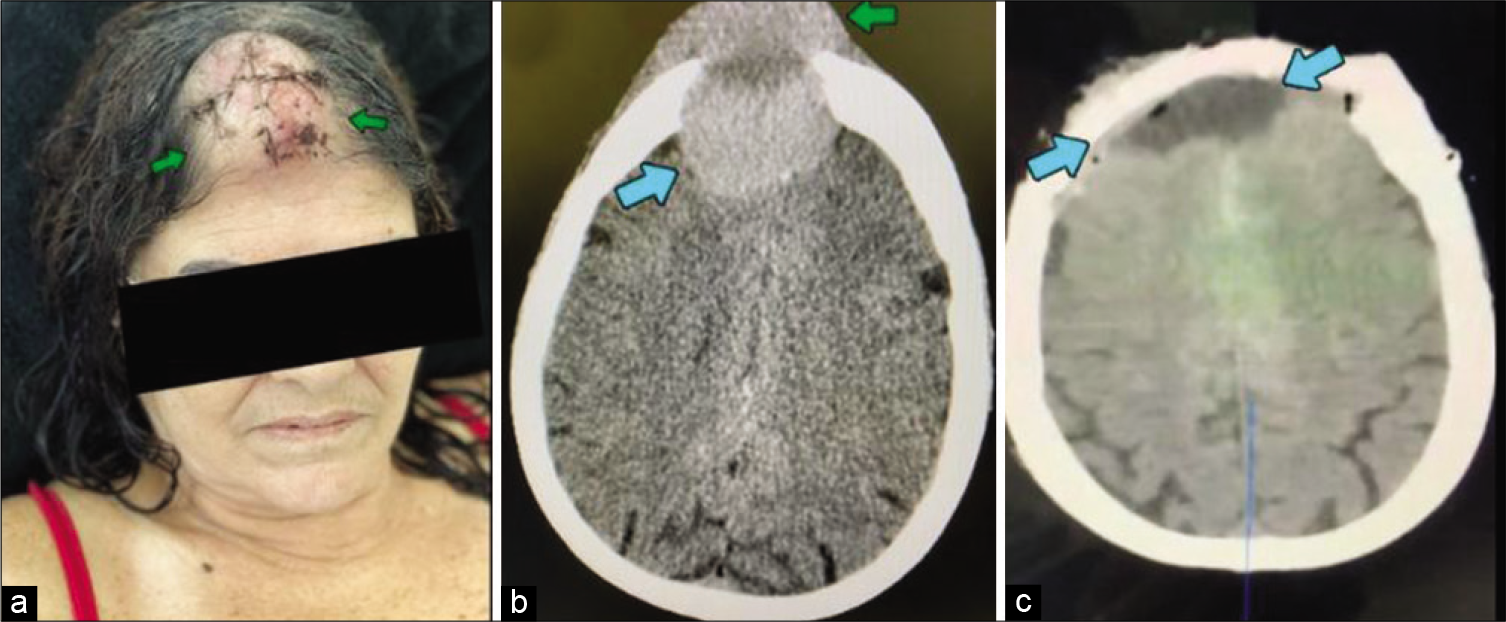
Figure 1:
Patient’s incision aspect after first approach (a) without prior imaging. Preoperative CT scan (b) showing intracranial (blue arrow) and extracranial (green arrow) components of the tumor. Postoperative imaging (c) showing no residual intra or extracranial lesions after evacuation (blue arrows).
Recently in low-income and middle-income contexts, intraoperative ultrasound is shown to be a cost-effective and widely available tool for both diagnostic and neuronavigation/ surgical planning purposes, allowing multiple derivations of both intraoperative and preoperative usages.[
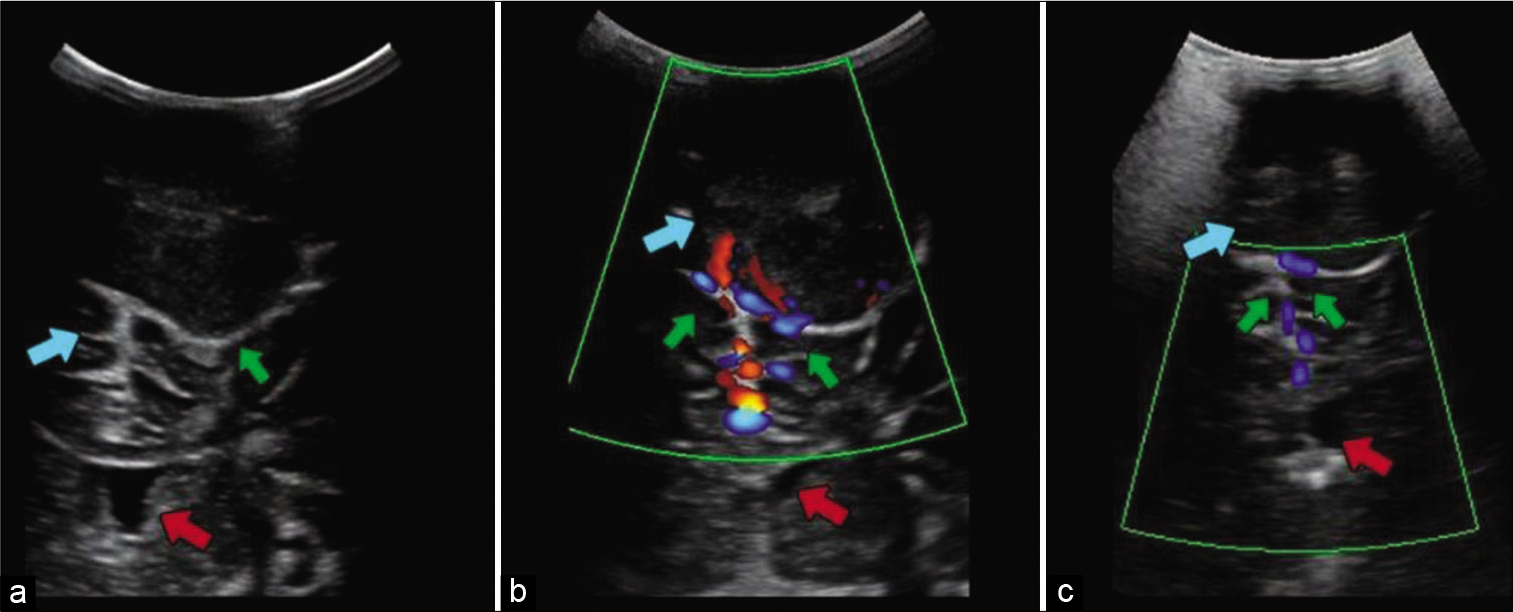
Figure 2:
Ultrasound image (a) showing the exophytic lesion (green arrow) in direct contact with the cerebral parenchyma (blue arrow). Bone erosion created a window in the frontal bone through which even the lateral ventricles (red arrow) are visible. Doppler ultrasound performed before embolization (b) showing vascularity of the tumor (green arrows) and after embolization (c) showing reduced blood flow (green arrows). In these images, the lesion (green arrow and blue arrows, a and b image respectively) and the lateral ventricles (red arrows) surrounded by brain parenchyma are still seen.
Declaration of patients consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no Conflict of Interest.
Declaration of patients consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no Conflict of Interest.
References
1. Abdi A, Armijo E, Seif D, Kang T. Man with a forehead mass: Detection of a forehead pseudoaneurysm with bedside ultrasonography. Case Rep Emerg Med. 2014. 2014: 647175
2. Brown JM, Cherry AP. Subcutaneous meningioma. Med J Aust. 1971. 2: 1072-3
3. Buerki RA, Horbinski CM, Kruser T, Horowitz PM, James CD, Lukas RV. An overview of meningiomas. Future Oncol. 2018. 14: 2161-77
4. Kaale AJ, Rutabasibwa N, Mchome LL, Lillehei KO, Honce JM, Kahamba J. The use of intraoperative neurosurgical ultrasound for surgical navigation in low-and middle-income countries: The initial experience in Tanzania. J Neurosurg. 2020. 134: 630-7
5. Neches SK, Parcells AL, Feintisch AM, Granick MS. Submuscular lipoma of the forehead. Eplasty. 2015. 15: ic17
6. Sewell LD, Adams DC, Marks VJ. Subcutaneous forehead nodules: Attention to the button osteoma and frontalis-associated lipoma. Dermatol Surg. 2008. 34: 791-8

