

- Department of Orthopedic Surgery, Noshiro Kosei Medical Center, Noshiro, Japan.
- Department of Orthopedic Surgery, Akita University Graduate School of Medicine, Hondo, Akita, Japan.
Correspondence Address:
Jumpei Iida
Department of Orthopedic Surgery, Akita University Graduate School of Medicine, Hondo, Akita, Japan.
DOI:10.25259/SNI_893_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jumpei Iida1, Naohisa Miyakoshi2, Michio Hongo2, Hiroshi Sasaki1, Hiroki Ito1, Hitoshi Kubota1, Takeshi Sato1, Yoichi Shimada2. Herniation of the cauda equina into the facet joint through a pseudomeningocele: A case report and literature review. 20-Jan-2021;12:30
How to cite this URL: Jumpei Iida1, Naohisa Miyakoshi2, Michio Hongo2, Hiroshi Sasaki1, Hiroki Ito1, Hitoshi Kubota1, Takeshi Sato1, Yoichi Shimada2. Herniation of the cauda equina into the facet joint through a pseudomeningocele: A case report and literature review. 20-Jan-2021;12:30. Available from: https://surgicalneurologyint.com/surgicalint-articles/10529/
Date of Submission
10-Dec-2020
Date of Acceptance
25-Dec-2020
Date of Web Publication
20-Jan-2021
Abstract
Background: Incidental durotomy is a well-known complication of spinal surgery. It can lead to persistent cerebrospinal fluid leakage resulting in significant secondary complications. Here, we present a case in which the cauda equina herniated into a pseudomeningocele that penetrated a facet joint, leading to lower extremity radiculopathy warranting surgical correction.
Case Description: One year ago, a 67-year-old male underwent a partial left L4-L5 laminectomy. At surgery, a durotomy was repaired with a nylon suture and reinforced with a fat patch. He subsequently presented with severe left lower extremity radiculopathy and a partial cauda equina syndrome. On MR, the cauda equina had herniated into a pseudomeningocele that penetrated the left facet joint. Once the defect was repaired at surgery, the patient’s symptoms improved.
Conclusion: It is critical to correctly repair an intraoperative durotomy to avoid further neurological deficits that may include cauda equina herniation into pseudomeningoceles penetrating facet joints.
Keywords: Cauda equina, Incidental durotomy, Posterior spinal fixation, Pseudomeningocele
INTRODUCTION
Incidental durotomy occurs in 0.5–18% of spinal operations.[
CASE PRESENTATION
Clinical findings
A year ago, a 67-year-old male presented with the acute onset of left-sided low back, hip, and left lower extremity pain for which he underwent a left-sided L4-L5 laminectomy. During surgery, there was a 2 mm left-sided durotomy that was repaired with a nylon suture and a fat patch graft. The subsequent MR examinations documented a persistent CSF leak that spontaneously resolved 3 months later. However, the patient again presented a year later with recurrent left-sided radiculopathy characterized by SLR 10 degrees, 3–4 motor function involving the iliopsoas, tibialis anterior, and extensor hallucis longus muscle distributions, and decreased left patellar and Achilles responses.
Radiological findings
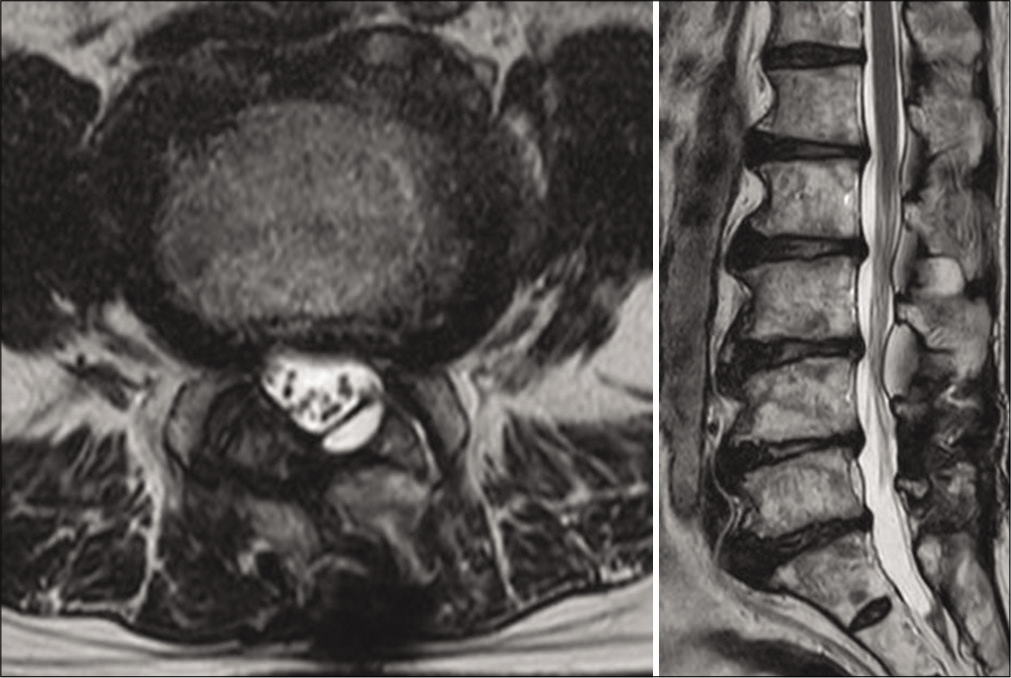
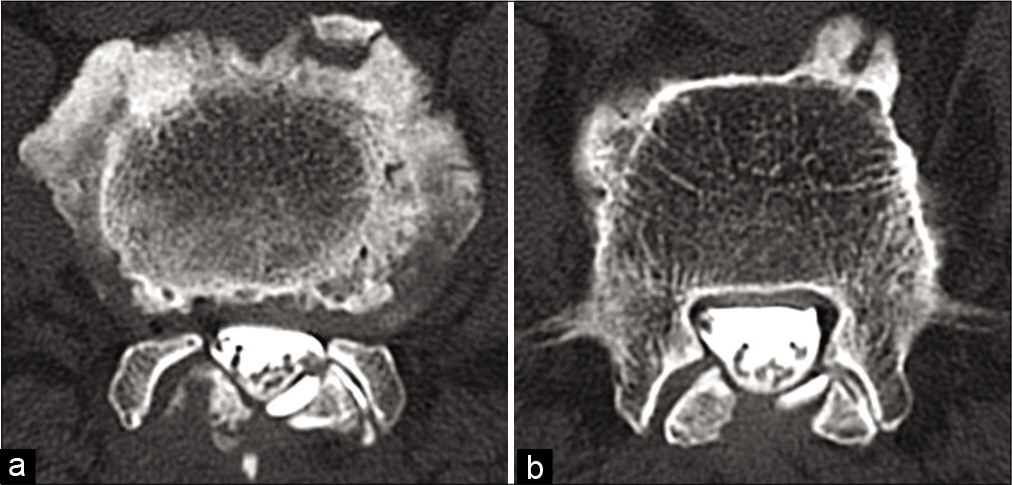
The lumbar X-ray showed the prior operative defect at the L4–L5 level, while the MR documented a left-sided pseudomeningocele extending into the left L4–L5 facet joint [
Secondary surgery
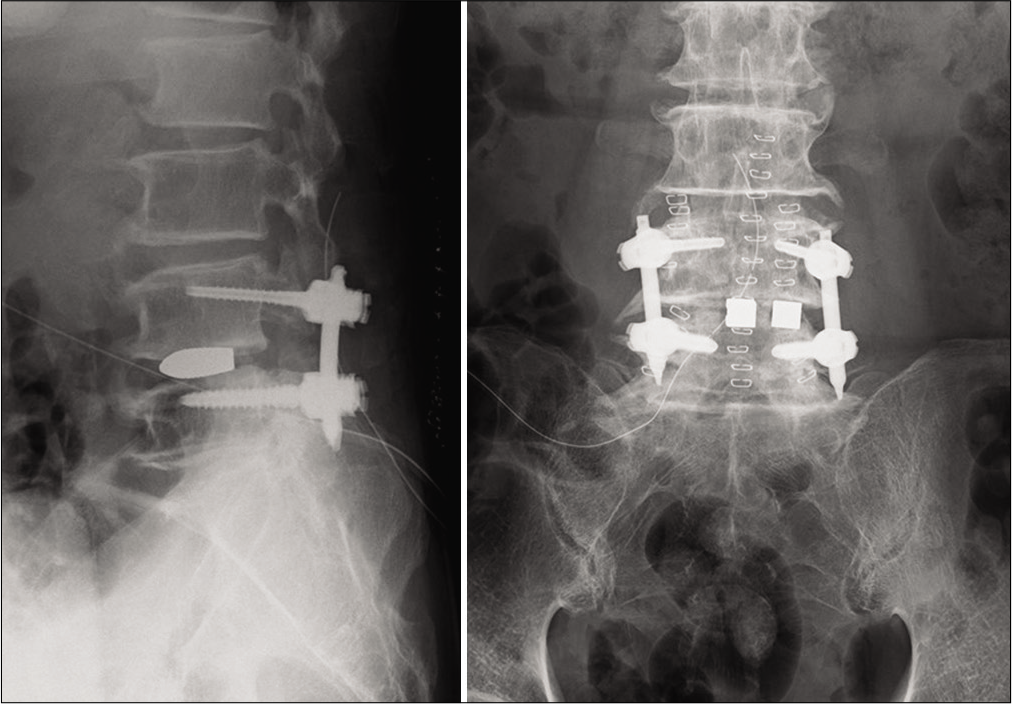
The patient underwent a secondary procedure 7 days later consisting of a L4–L5 facetectomy with posterior L4–L5 lumbar interbody fusion [
DISCUSSION
Patients who experience traumatic intraoperative dural tears during lumbar surgery may develop postoperative recurrent/persistent radiculopathy and/or cauda equina syndromes attributed to herniation of neural tissues into pseudomeningoceles.
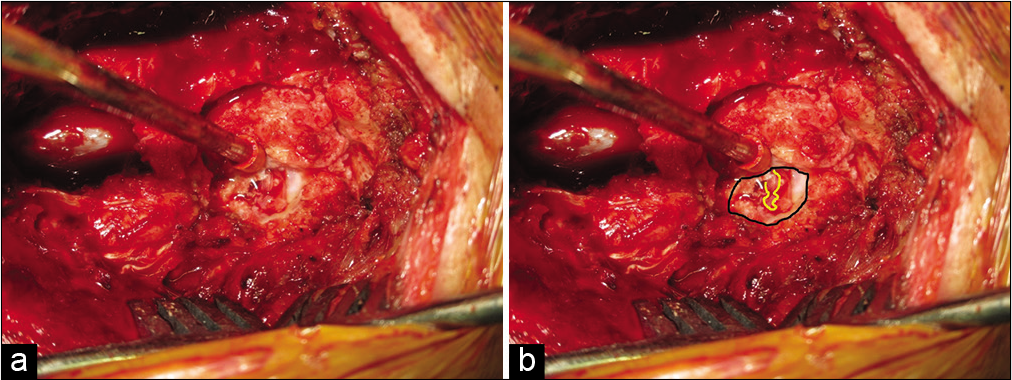
In this case, the cauda equina herniated into a pseudomeningocele that extended into the left L4–L5 facet joint. Other authors have reported herniation of nerve roots/ cauda equina through dural defects attribute to similar lumbar surgery (e.g., transdural cauda equina incarceration after microlumbar discectomy),[
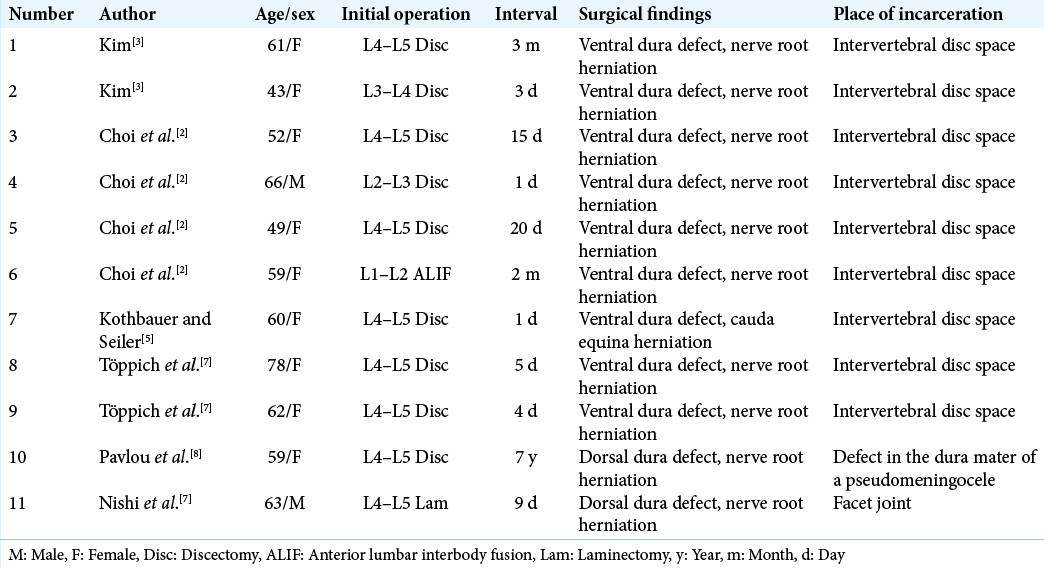
However, only rarely has the nerve root herniated into a pseudomeningocele that then extended into a facet joint (e.g., in Nishi et al. the nerve root herniated into a large pseudomeningocele [
Here, a pseudomeningocele developed due to an inadequately repaired dural tear during a lumbar discectomy and resulted in cauda equina herniation into the resultant pseudomeningocele that then extended into the facet joint. In the future, such dural repairs should avoid nylon sutures; rather, it is best to 7-0 Gore-Tex sutures or its equivalent where the needle is smaller than the suture itself, and the suture/knot will not “unfurl.” Further, it muscle patch grafts not fat grafts should supplement dural closures, as a fat graft shrink/resorb, thus failing to maintain occlusion the leakage site.
CONCLUSION
During a left L4–L5 laminectomy, a durotomy resulted in the cauda equina herniation into a left-sided L4–L5 pseudomeningocele with extension into the left L4–L5 facet joint. Once the pseudomeningocele was repaired, the patient’s recurrent radiculopathy/cauda equina syndrome was repaired.
Ethical approval
This study was approved by the Medical Ethics Board of Noshiro Kosei Medical Center (approval number YD-057).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alshameeri ZA, El-Mubarak A, Kim E, Jasani V. A systematic review and meta-analysis on the management of accidental dural tears in spinal surgery: Drowning in information but thirsty for a clear message. Eur Spine J. 2020. 29: 1671-85
2. Choi JH, Kim J, Jang J, Lee DY. Transdural nerve rootlet entrapment in the intervertebral disc space through minimal dural tear: Report of 4 cases. J Korean Neurosurg Soc. 2013. 53: 52-6
3. Kim YJ. Incarceration of spinal nerve root through incidental durotomy as a cause of sciatica. Korean J Spine. 2017. 14: 103-5
4. Kogias E, Klingler JH, Jimenez PF, Vasilikos I, Sircar R, Scholz C. Incidental durotomy in open versus tubular revision microdiscectomy: A retrospective controlled study on incidence, management, and outcome. Clin Spine Surg. 2017. 30: E1333-7
5. Kothbauer KF, Seiler RW. Transdural cauda equina incarceration after microsurgical lumbar discectomy: Case report. Neurosurgery. 2000. 47: 1449-51
6. McMahon P, Dididze M, Levi AD. Incidental durotomy after spinal surgery: A prospective study in an academic institution. J Neurosurg Spine. 2012. 17: 30-6
7. Nishi S, Hashimoto N, Takagi Y, Tsukahara T. Herniation and entrapment of a nerve root secondary to an unrepaired small dural laceration at lumbar hemilaminectomies. Spine (Phila Pa 1976). 1995. 20: 2576-9
8. Pavlou G, Bucur SD, van Hille PT. Entrapped spinal nerve roots in a pseudomeningocoele as a complication of previous spinal surgery. Acta Neurochir (Wien). 2006. 148: 215-9
9. Töppich HG, Feldmann H, Sandvoss G, Meyer F. Intervertebral space nerve root entrapment after lumbar disc surgery, Two cases. Spine (Phila Pa 1976). 1994. 19: 249-50
10. Tsutsumimoto T, Yui M, Uehara M, Ohta H, Kosaku H, Misawa H. A prospective study of the incidence and outcomes of incidental dural tears in microendoscopic lumbar decompressive surgery. Bone Joint J. 2014. 96: 641-5

