

- Department of Neurosurgery, Sina Hospital, Tehran University of Medical Sciences, Tehran, Iran
Correspondence Address:
Abbas Amirjamshidi
Department of Neurosurgery, Sina Hospital, Tehran University of Medical Sciences, Tehran, Iran
DOI:10.4103/sni.sni_446_16
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ahmad Pourrashidi Boshrabadi, Ali Naiem, Seyed Shahab Ghazi Mirsaeid, Kourosh Karimi Yarandi, Abbas Amirjamshidi. Hydrocephalus as the sole presentation of primary diffuse large B-cell lymphoma of the brain: Report of a case and review of literature. 01-Aug-2017;8:165
How to cite this URL: Ahmad Pourrashidi Boshrabadi, Ali Naiem, Seyed Shahab Ghazi Mirsaeid, Kourosh Karimi Yarandi, Abbas Amirjamshidi. Hydrocephalus as the sole presentation of primary diffuse large B-cell lymphoma of the brain: Report of a case and review of literature. 01-Aug-2017;8:165. Available from: http://surgicalneurologyint.com/surgicalint-articles/hydrocephalus-as-the-sole-presentation-of-primary-diffuse-large-b%e2%80%91cell-lymphoma-of-the-brain-report-of-a-case-and-review-of-literature/
Date of Submission
11-Nov-2016
Date of Acceptance
18-May-2017
Date of Web Publication
01-Aug-2017
Abstract
Background:The most common lymphoid malignancy in adults is diffuse large B-cell lymphoma (DLBCL). The median age of occurrence of DLBCL is between 6th and 7th decade of life, although some other types of aggressive non-Hodgkin’s lymphomas (NHL) are present in younger age. Primary central nervous system lymphoma (PCNSL) is an uncommon type of extranodal NHL, which is either more prevalent or is diagnosed more often than before.
Case Description:A 22-year-old man with ventriculoperitoneal shunt (VPS) performed at another center was referred with manifestations of shunt malfunction, unusual behavior, dysphasia, and hallucination. The shunt malfunction was handled appropriately several times and exploration of the enhancing cystic temporal lesion confirmed the diagnosis of DLBCL.
Conclusion:In this communication, we intend to highlight the issue that hydrocephalus refractory to several interventions can be the sole manifestation of PCNSL and needs special clinical considerations.
Keywords: Diffuse large B-cell lymphoma, hydrocephalus, shunt malfunction
INTRODUCTION
The most common lymphoid malignancy in adults is diffuse large B-cell lymphoma (DLBCL). The incidence of non-Hodgkin’s lymphomas (NHL) is estimated to be 15–20 cases/100,000 annually.[
PCNL can involve brain parenchyma, spinal cord, leptomeninges, and eyes.[
The purpose of this communication is to highlight a possible strange clinical presentation of PCNL with hydrocephalus resistant to current therapies.
CASE REPORT
A 22-year-old man was referred to this hospital with manifestations of shunt malfunction and history of ventriculoperitoneal shunt (VPS) at another center. The symptoms of increased intracranial pressure appeared the previous year with unusual behavior, speech disturbance, and hallucination before admission in the previous center. His symptoms improved with shunting but recurred after 4 months. Shunt revision was performed and he was discharged with modified Rankin Scale (mRS) 2. The symptoms recurred 2 months later. He had no adenopathy and bone marrow aspiration was negative. Full paraclinical evaluations and all laboratory tests were highly suspicious of histiocytosis even though CD1 test was negative. Cerebrospinal fluid (CSF) analysis was normal (WBC: 4, RBC: 668, Glc: 5, Pro: 54), and CSF culture and cytology was negative. He was treated with corticosteroids and another shunt was placed in the contralateral ventricle under antibiotic coverage. The reports of magnetic resonance imaging (MRI) provided from the previous hospital denoted a communicating hydrocephalus and no space occupying lesion all along the brain and spinal cord. After 3 months, he was admitted in our hospital. The mentioned information was all the data that were delivered from the previous center to our hospital.
In physical examination, he was conscious and awake but hardly cooperative and sometimes even unresponsive to painful stimuli. Brain computed tomography (CT) scan showed cystic dilatation of left temporal horn surrounded by perilesional edema [
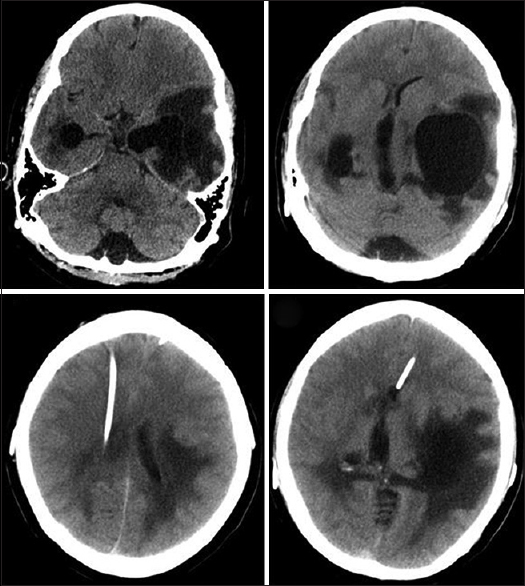
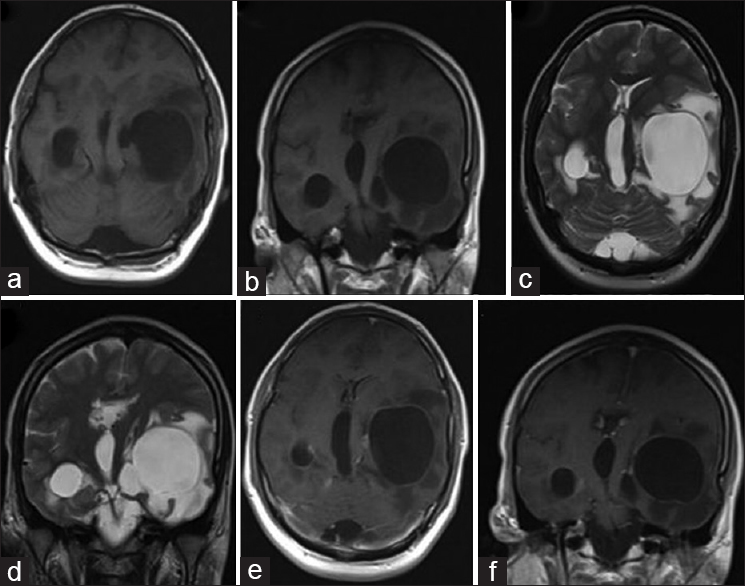
Figure 2
Hypointense cystic lesion in axial and coronal T1 weighted MRI (a and b); hyperintense cystic lesion with massive edema in axial and coronal T2 weighted MRI (c and d); rim enhancing lesion in axial and coronal contrast-T1 weighted MRI (e and f). (Sagittal views not included due to bad quality)
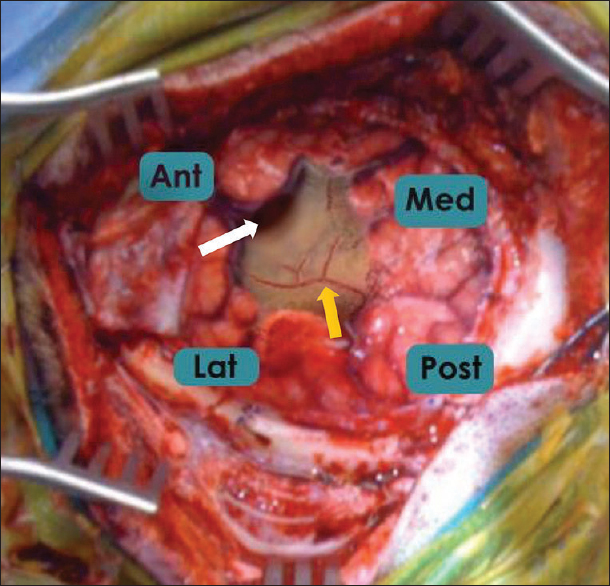
He underwent craniotomy to explore the presumably dilated temporal horn. There was no abnormality in the extradural and subdural region in the exposed area of the temporal region. The arachnoid was shiny and no granulomatous change or focal thickening of the arachnoid was visible. Trans sulcal approach in between the middle and low temporal gyri preformed to enter the cystic/expanded lesion. Entering the dilated/isolated temporal horn, nests of shiny debris infiltrating the ependymal layer of the dilated horn could be stripped off and removed as much as possible [
DISCUSSION
PCNSL has a highly fulminant course and misdiagnosis or late diagnosis may lead to early mortality.[
The predisposing and etiological factors for DLBCL include agents producing molecular aberrations,[
PCNSL is characterized by nonspecific neurologic symptoms which is in contrary to the clinical presentation of the systemic “B” type of lymphoma usually presenting with fever, weight loss, and night sweats. The incidence of focal neurological deficits and global neurological deterioration due to PCNSL are the same; that is why the authors have not been able to define typical clinical manifestations for it.[
The neuropsychological features are highly associated with involvement of the periventricular white matter or the corpus callosum by the tumor.[
The present case demonstrates that PCNSL can involve ventricular system and lead to hydrocephalus. A refractory or recurrent case of hydrocephalus after shunting needs to be evaluated for an underlying disease such as DLBCL.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bataille B, Delwail V, Menet E, Vandermarcq P, Ingrand P, Wager M. Primary intracerebral malignant lymphoma: Report of 248 cases. J Neurosurg. 2000. 92: 261-6
2. Chen HS, Shen MC, Tien HF, Su IJ, Wang CH. Leptomeningeal seeding with acute hydrocephalus—unusual central nervous system presentation during chemotherapy in Ki-1-positive anaplastic large-cell lymphoma. Acta Haematol. 1996. 95: 135-9
3. Cohen Y, Paltiel O, Amir G, Da’as N, Engelhard D, Polliack A. Unusual cytomegalovirus complications after autologous stem cell transplantation for large B cell lymphoma: Massive gastrointestinal hemorrhage followed by a communicating hydrocephalus. Bone Marrow Transplant. 2002. 29: 715-6
4. Eichler AF, Batchelor TT. Primary central nervous system lymphoma: Presentation, diagnosis and staging. Neurosurg Focus. 2006. 21: E15-
5. Ferreri AJ, Marturano E. Primary CNS lymphoma. Best Pract Res Clin Haematol. 2012. 25: 119-30
6. Ferreri AJ. How I treat primary CNS lymphoma. Blood. 2011. 118: 510-22
7. Gallop-Evans E. Primary central nervous system lymphoma. Clin Oncol. 2012. 24: 329-38
8. Gelabert González M, Castro Bouzas D, SerramitoGarcía R, Frieiro Dantas C, Aran Echabe E. Primary central nervous system lymphoma. Neurologia. 2013. 28: 283-93
9. Gocmen S, Gamsizkan M, Onguru O, Sefali M, Erdogan E. Primary dural lymphoma mimicking a subdural hematoma. J Clin Neurosci. 2010. 17: 380-2
10. Hoeller S, Tzankov A, Pileri SA, Went P, Dirnhofer S. Epstein–Barr virus-positive diffuse large B-cell lymphoma in elderly patients is rare in Western populations. Human Pathol. 2010. 41: 352-7
11. Ishizaki T, Mitsui T, Uchiyama Y, Ogawa Y, Koiso H, Takizawa M. Primary leptomeningeal B-cell lymphoma with normal pressure hydrocephalus at diagnosis. Rinsho Ketsueki. 2015. 56: 2441-6
12. Kim JH, Kang JK, Lee SA. Hydrocephalus and hyponatremia as the presenting manifestations of primary CNS lymphoma. Eur Neurol. 2006. 55: 39-41
13. Kondoh T, Tamaki N, Nagashima T, Kokunai T, Matsumoto S, Ogawa R. A case of primary malignant lymphoma of the brain associated with acute hydrocephalus. No Shinkei Geka. 1989. 17: 683-6
14. Kridel R, Dietrich PY. Prevention of CNS relapse in diffuse large B-cell lymphoma. Lancet Oncol. 2011. 12: 1258-66
15. Liao CH, Lin SC, Hung SC, Hsu SP, Ho DM, Shih YH. Primary large B-cell lymphoma of the fourth ventricle. J Clin Neurosci. 2014. 21: 180-3
16. Lim T, Kim SJ, Kim K, Lee J, Lim DH, Lee DJ, Baek KK. Primary CNS lymphoma other than DLBCL: A descriptive analysis of clinical features and treatment outcomes. Ann Hematol. 2011. 90: 1391-8
17. Melinz K, Bonelli RM, Niederwieser G, Kenner L, Reisecker F. Primary high grade B cell lymphoma of the CNS. Case report and review of the literature. Nervenarzt. 2002. 73: 779-84
18. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013. 63: 11-30
19. Zucca E, Conconi A, Mughal TI, Sarris AH, Seymour JF, Vitolo U. Patterns of outcome and prognostic factors in primary large-cell lymphoma of the testis in a survey by the International Extranodal Lymphoma Study Group. J Clin Oncol. 2003. 21: 20-7

