

- Department of Neurosurgery, Warren Alpert School of Medicine, Brown University, Providence, Rhode Island, United States.
DOI:10.25259/SNI_232_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Rahul Amrutur Sastry, Jared Fridley, Albert Telfeian, Ziya Gokaslan, Adetokunbo Oyelese. Image-guided resection of lumbar monostotic fibrous dysplasia: A case report and technical note. 21-Oct-2020;11:346
How to cite this URL: Rahul Amrutur Sastry, Jared Fridley, Albert Telfeian, Ziya Gokaslan, Adetokunbo Oyelese. Image-guided resection of lumbar monostotic fibrous dysplasia: A case report and technical note. 21-Oct-2020;11:346. Available from: https://surgicalneurologyint.com/surgicalint-articles/10349/
Date of Submission
29-Apr-2020
Date of Acceptance
23-Jun-2020
Date of Web Publication
21-Oct-2020
Abstract
Background: Monostotic fibrous dysplasia rarely involves the lumbar spine. Although its optimal surgical management is unknown, some recommend complete resection to decrease the likelihood of future recurrence.
Case Description: A 41-year-old female presented with fibrous dysplasia involving the right L4 lamina and spinous process. Following image-guided en bloc resection, the patient remained asymptomatic without evidence of recurrence 8 months later.
Conclusion: Image-guided excision of monostotic fibrous dysplasia involving the right L4 lamina and spinous process was successfully performed without clinical or radiographic evidence of recurrence within 8 postoperative months.
Keywords: Fibrous dysplasia, Intraoperative computed tomography, Navigation, Spine
INTRODUCTION
Monostotic or polyostotic fibrous dysplasia (i.e., involving single or multiple bones) is an abnormality of bone development resulting in dysplastic fibrous tissue localized to the bony trabeculae in the absence of appropriate mineralization. It compromises approximately 5% of all benign bony tumors and is commonly discovered incidentally in the ribs, femur, tibia, and maxilla[
Although the optimal surgical management of these lesions is unclear, some recommend en bloc resection to reduce the risk of recurrence.[
CASE REPORT
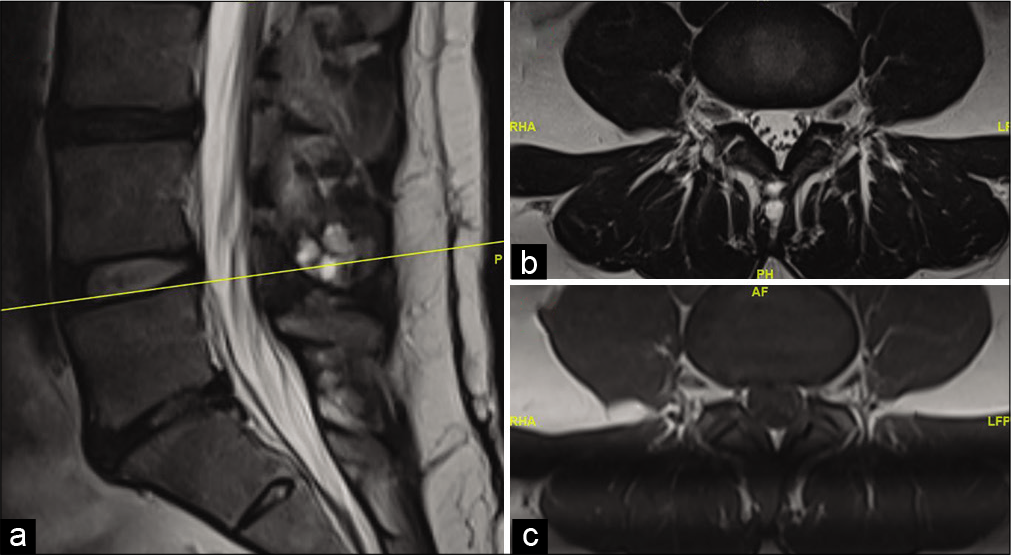
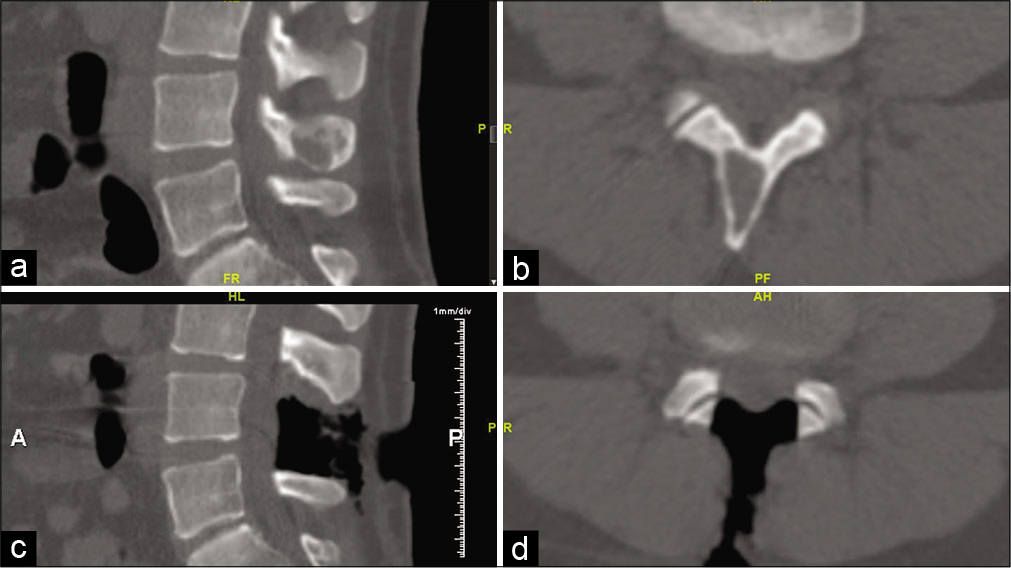
A 41-year-old female presented with a one year history of low back and intermittent right leg pain that was worse at night. MRI revealed a T1-hypointense and T2-hyperintense cystic lesion involving the right L4 spinous process and lamina (measuring 11 mm by 21 mm) [
DISCUSSION
Fibrous dysplasia is a common benign skeletal lesion. In the monostotic form, lesions tend to enlarge with bony growth and senesce with skeletal maturity.[
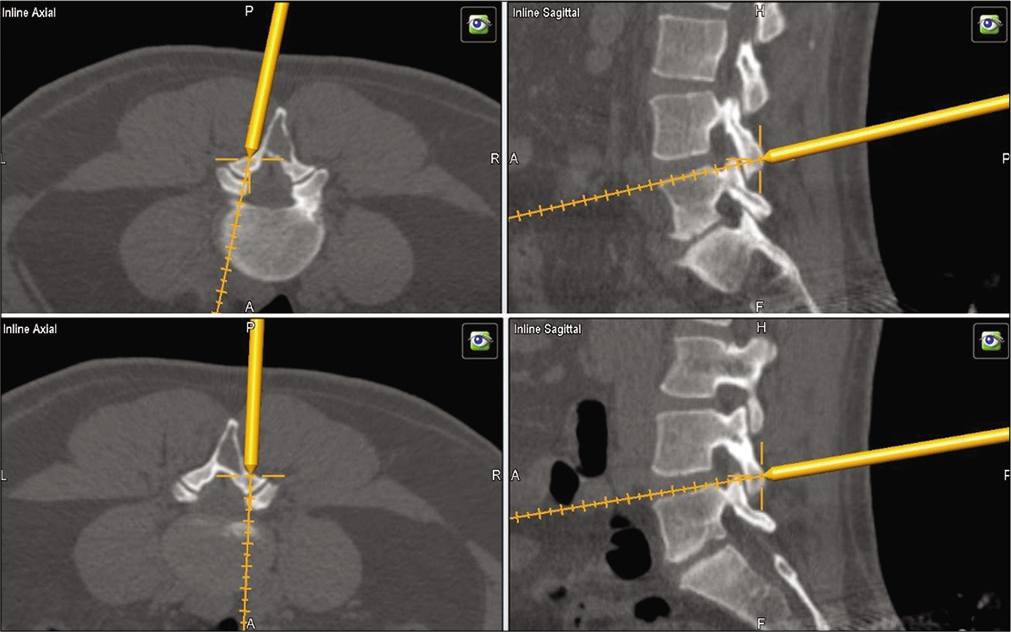
Here, we described a 41-year-old female who presented with a right-sided cystic lesion involving the L4 spinous process and lamina who underwent open en bloc resection utilizing iCT/MRI guidance. She has remained asymptomatic without evidence of recurrence 8 months postoperatively.
Literature review of lumbar monostotic fibrous dysplasia
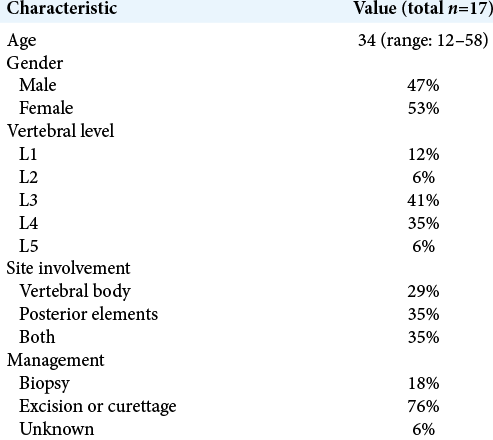
There are 17 previously reported cases of monostotic fibrous dysplasia involving the lumbar spine [
CONCLUSION
A 41-year-old female with lumbar monostotic fibrous dysplasia involving the right L4 lamina and spinous process successfully underwent en bloc resection with L4 right-sided laminectomy and spinous process resection facilitated by intraoperative CT navigation fused with preoperative MRI.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Dasenbrock HH, Clarke MJ, Bydon A, McGirt MJ, Witham TF, Sciubba DM. En bloc resection of sacral chordomas aided by frameless stereotactic image guidance: A technical note. Neurosurgery. 2012. 70: 82-7
2. DiCaprio MR, Enneking WF. Fibrous dysplasia, Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am. 2005. 87: 1848-64
3. Drazin D, Bhamb N, Al-Khouja LT, Kappel AD, Kim TT, Johnson JP. Image-guided resection of aggressive sacral tumors. Neurosurg Focus. 2017. 42: E15
4. Edgerton MT, Persing JA, Jane JA. The surgical treatment of fibrous dysplasia. With emphasis on recent contributions from cranio-maxillo-facial surgery. Ann Surg. 1985. 202: 459-79
5. Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum?. Bone Joint J. 2013. 95B: 1417-24
6. Konakondla S, Albers JA, Li X, Barber SM, Nakhla J, Houghton CE. Maximizing sacral chordoma resection by precise 3-dimensional tumor modeling in the operating room using intraoperative computed tomography registration with preoperative magnetic resonance imaging fusion and intraoperative neuronavigation: A case series. World Neurosurg. 2019. 125: e1125-31
7. Meredith DS, Healey JH. Twenty-year follow-up of monostotic fibrous dysplasia of the second cervical vertebra: A case report and review of the literature. J Bone Joint Surg Am. 2011. 93: e74
8. Nasser R, Drazin D, Nakhla J, Al-Khouja L, Brien E, Baron EM. Resection of spinal column tumors utilizing image-guided navigation: A multicenter analysis. Neurosurg Focus. 2016. 41: E15
9. Ruggieri P, Sim FH, Bond JR, Unni KK. Malignancies in fibrous dysplasia. Cancer. 1994. 73: 1411-24
10. Valentini V, Cassoni A, Marianetti TM, Terenzi V, Fadda MT, Iannetti G. Craniomaxillofacial fibrous dysplasia: Conservative treatment or radical surgery? A retrospective study on 68 patients. Plast Reconstr Surg. 2009. 123: 653-60
11. Yang C, Zhu B, Chen A. Imaging diagnosis of monostotic fibrous dysplasia in thoracic and lumbar spine vertebrae. J Huazhong Univ Sci Technol Med Sci. 2007. 27: 684-6

