

- Department of Neuroscience, Winthrop University Hospital, Mineola, NY, USA
Correspondence Address:
Nancy E. Epstein
Department of Neuroscience, Winthrop University Hospital, Mineola, NY, USA
DOI:10.4103/2152-7806.166874
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Epstein NE. Incidence and management of cerebrospinal fluid fistulas in 336 multilevel laminectomies with noninstrumented fusions. Surg Neurol Int 08-Oct-2015;6:
How to cite this URL: Epstein NE. Incidence and management of cerebrospinal fluid fistulas in 336 multilevel laminectomies with noninstrumented fusions. Surg Neurol Int 08-Oct-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/incidence-and-management-of-cerebrospinal-fluid-fistulas-in/
Abstract
Background:The incidence (e.g., 3–27%) and the types of cerebrospinal fluid (CSF) fistulas occurring during multilevel lumbar laminectomy with noninstrumented spinal fusions varies.
Methods:From 2000 to 2015, we retrospectively evaluated the incidence/etiologies of CSF fistulas occurring for 336 patients undergoing average 4.7 laminectomies with average 1.4 level noninstrumented fusions over a 15 year period. The varied etiologies of CSF leaks included; ossification of the yellow ligament (OYL) extending through the dura, postoperative surgical scar, iatrogenic traumatic leak, epidural steroid injections (ESI), resection of synovial cysts, and the removal of intradural tumors. Techniques for primary repairs included combinations of; 7-0 Gore-Tex (Newark, Delaware, USA) sutures, micro-dural staples, muscle patch/other (e.g., bovine pericardial) grafts, fibrin sealants/glues (e.g., Tisseel; Baxter International Inc., Westlake Village, CA, USA), and Duragen (Integra LifeSciences, Hawthorne, NY, USA) including both the thin and suturable types.
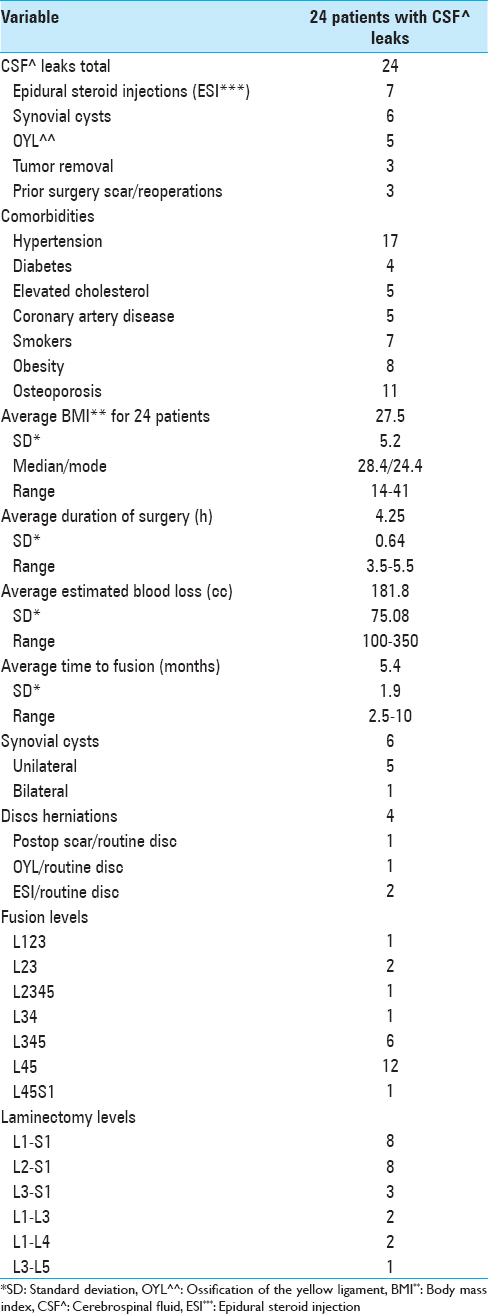
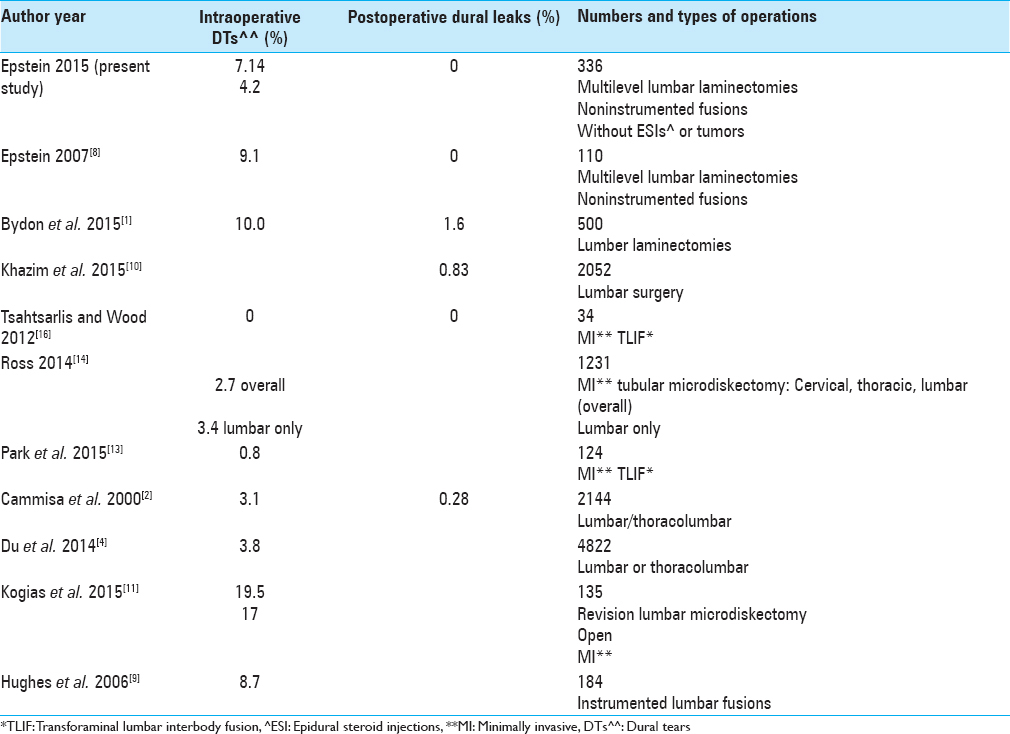
Results:The etiologies of CSF fistulas in descending order included: Epidural spinal injections (ESI) (7 patients), synovial cysts (6 patients), OYL (5 patients), and equally for postoperative scar and intradural tumors (3 patients). CSF fistulas occurred in 24 (7.14%) of 336 patients; this frequency was reduced to 4.2% when ESI and intradural tumors were excluded.
Conclusion:CSF fistulas occurred in 7.14% of 336 patients undergoing average 4.7 multilevel laminectomies with average 1.4 level noninstrumented fusions attributed to a lumbar stenosis with mild/moderate instability. The dural repair addressed seven prior ESI, six synovial cysts, five OYL, and operative scarring and intradural tumors (three apiece). Knowing the pathologies contributing to CSF fistulas should help the surgeon to better anticipate and treat these fistulas.
Keywords: Cerebrospinal fluid fistulas, epidural steroid injections, lumbar stenosis, multilevel laminectomy, noninstrumented fusion, ossified yellow ligament, postoperative scar, synovial cysts
INTRODUCTION
The incidence/type of cerebrospinal fluid (CSF) fistulas for patients undergoing multilevel laminectomies with noninstrumented fusions varies from 3% to 27% in the literature.[
MATERIALS AND METHODS
Clinical background
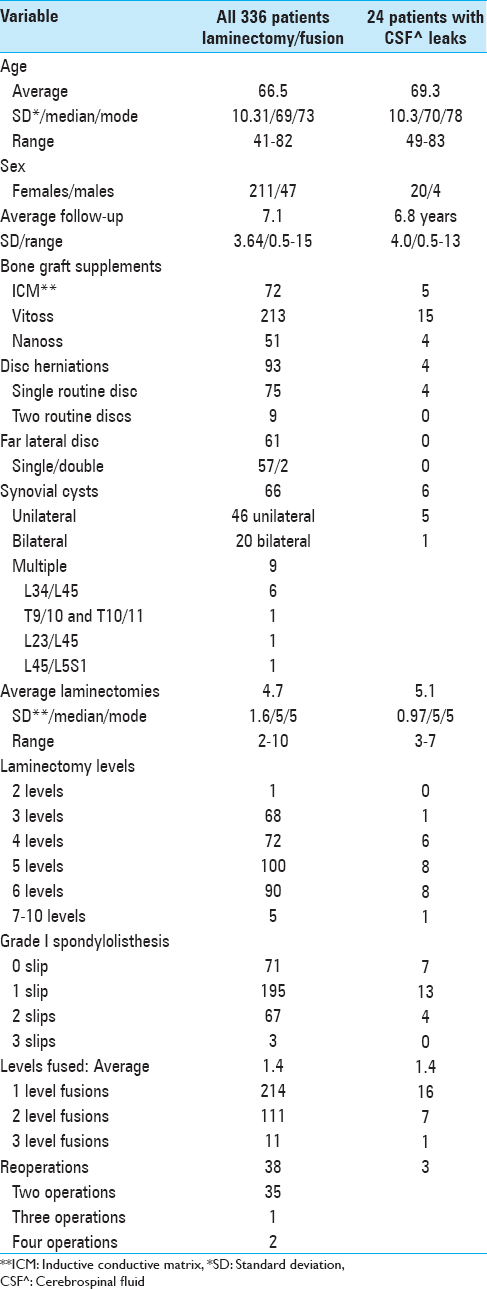
The 336 patients averaged 66.5 years of age, included 211 females and 47 males, and were followed for an average of 7.1 years [
Incidence of cerebrospinal fluid fistulas
The frequency of CSF fistulas was retrospectively assessed for all 336 patients. Direct primary repair required combinations of: 7-0 Gore-Tex (Newark, Delaware, USA) sutures, micro-dural staples, muscle patch grafts, or other grafts (e.g., bovine pericardium), a fibrin sealant (we used Tisseel: Baxter International Inc., Westlake Village, CA, USA), and Duragen (Integra LifeSciences, Hawthorne, NY, USA) utilizing thin and/or sutureable variants.
RESULTS
Clinical parameters for the total of 24 patients who developed dural tears (DTs) revealed: they were slightly older, had more synovial cysts, included a comparable number with prior surgery, showed slighlty more average laminectomy levels, but included identical average levels of noninstrumented fusions [Tables
Seven epidural steroid injections: the leading etiology of intraoperative cerebrospinal fluid fistulas
Although we did not have accurate data regarding the total number of ESI performed for all 336 patients, we did encounter 7 patients with intraoperative punctate CSF fistulas secondary to ESI requiring direct dural repair; these were predominantly recognized in patients undergoing the most recent surgery. All 7 had undergone at least one ESI within 5 weeks of surgery; 5 patients had undergone 3 ESI, 1 patient had over 6 ESI performed over the prior 2 years, and another patient had over 12 injections over the last 4 years.
Six synovial cysts leading to cerebrospinal fluid fistulas
Sixty-six of 336 patients in the series had synovial cysts; 46 were unilateral while 20 were bilateral [
Five cerebrospinal fluid fistulas with ossification of the yellow ligament extending to/through the dura
All 336 patients in this series had OYL in conjunction with lumbar spinal stenosis; 5 (1.5%) of these patients developed CSF fistulas due to OYL extending to/through the dura [Tables
Three cases of cerebrospinal fluid fistulas following prior surgery
There were 38 patients in this series who had prior lumbar surgery; 35 patients had two, one had three, and two had a total of four prior operations [Tables
Three cerebrospinal fluid fistulas due to intradural tumor removal (neurofibromas)
Three (7.9%) patients required removal of intradural extramedullary neurofibromas in conjunction with decompression of stenosis [
Subset of disc herniations with dural tears attributed to postoperative scar, ossification of the yellow ligament, and epidural steroid injections
Four of the 24 patients with intraoperative DT also exhibited routine disc herniations in conjunction with the previously noted: prior operative scar (1 patients), OYL (1 patient), and ESI (1 patient) [Tables
Incidence of postoperative recurrence of cerebrospinal fluid fistulas
Utilizing combinations of complex intraoperative repair techniques under an operating microscope, including 7-0 Gore-Tex sutures, micro-dural staples, muscle patch grafts, Duragen (soft/suturable-2 types), and Tisseel, no patients developed recurrent postoperative CSF fistulas.
DISCUSSION
Anticipated incidence of durotomy
Many quote an overall 3–27% incidence of intraoperative DT occurring during lumbar spinal surgery, while others cite additional smaller frequencies for postoperative dural fistulas [
Under-reported cerebrospinal fluid leaks for minimally invasive lumbar surgery
Although the studies quoted below cite extremely low frequencies of DT with minimally invasive (MIS or MI) lumbar surgery, the medicolegal system indicates a much higher incidence of DT in the hands of others’ not publishing their untoward experiences including major paralyses [
Rate of cerebrospinal fluid leaks for lumbar reoperations
Spine surgeons know that intraoperative DT's are more frequent with reoperations [
Risks of cerebrospinal fluid fistulas with synovial cysts
In 2012, Epstein discussed the “pros” of open surgical management of synovial cysts (success rates of up to 92.5%) versus the high incidence of DT and other complications with MIS or percutaneous techniques.[
Epidural steroid injections contribute to intraoperative cerebrospinal fluid fistulas
In 2014, Epstein noted that despite no documented long-term efficacy for ESI in spinal stenosis, ESI are typically administered in multiples of 3 to older patients, and increasingly result in intraoperative punctate DT.[
Treatment strategies for repairing cerebrospinal fluid fistulas
In 2015, Clajus et al. found that of 109 neurosurgical departments in Germany treating CSF fistulas, 65.1% utilized combinations of techniques; 28 (25.7%) used suture alone, 7 (6.4%) used fibrin-coated fleeces alone, 2 used (1.8%) muscle patch alone, and 1 (0.9%) used fibrin glue alone.[
Fibrin glues to strengthen dural repair
In 2013, Epstein reviewed the various techniques for direct primary repair of operatively recognized CSF fistulas.[
Computed tomography-guided epidural patching of postoperative cerebrospinal fluid fistulas
In 2014, Mihlon et al. evaluated the efficacy of repairing postoperative CSF fistulas utilizing MI, percutaneous CT-guided epidural patching.[
Prolonged Jackson-Pratt drainage for cerebrospinal fluid leaks following instrumented fusions
As an example of what not to do, I would offer the study by Hughes et al. in which they utilized prolonged Jackson-Pratt (JP) drainage to treat lumbar CSF leaks.[
CONCLUSION
Although DT may occur during any lumbar surgery, their frequency is greater with: recently preoperatively performed ESI (e.g., within the last 5 weeks), synovial cysts, severe OYL, prior surgery, and of course, electively opening the dura (e.g. a direct requisite for resection of intradural tumors). For all of these patients, the routine use of the operating microscope should help limit the frequency of DT, along with greater anticipation and vigilance at the levels of the most severe pathology. The recent over-use/abuse of ESI should also be taken into account, as patients with recent ESI should be counseled that resulting DT newly documented intraoperatively may require repair.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bydon M, Macki M, Abt NB, Sciubba DM, Wolinsky JP, Witham TF. Clinical and surgical outcomes after lumbar laminectomy: An analysis of 500 patients. Surg Neurol Int. 2015. 6: S190-3
2. Cammisa FP, Girardi FP, Sangani PK, Parvataneni HK, Cadag S, Sandhu HS. Incidental durotomy in spine surgery. Spine (Phila Pa 1976). 2000. 25: 2663-7
3. Clajus C, Stockhammer F, Rohde V. The intra- and postoperative management of accidental durotomy in lumbar spine surgery: Results of a German survey. Acta Neurochir (Wien). 2015. 157: 525-30
4. Du JY, Aichmair A, Kueper J, Lam C, Nguyen JT, Cammisa FP. Incidental durotomy during spinal surgery: A multivariate analysis for risk factors. Spine (Phila Pa 1976). 2014. 39: E1339-45
5. Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012. 3: S157-66
6. Epstein NE. A review article on the diagnosis and treatment of cerebrospinal fluid fistulas and dural tears occurring during spinal surgery. Surg Neurol Int. 2013. 4 Suppl 5: S301-17
7. Epstein NE. Commentary: Unnecessary preoperative epidural steroid injections lead to cerebrospinal fluid leaks confirmed during spinal stenosis surgery. Surg Neurol Int. 2014. 5: S325-8
8. Epstein NE. The frequency and etiology of intraoperative dural tears in 110 predominantly geriatric patients undergoing multilevel laminectomy with noninstrumented fusions. J Spinal Disord Tech. 2007. 20: 380-6
9. Hughes SA, Ozgur BM, German M, Taylor WR. Prolonged Jackson-Pratt drainage in the management of lumbar cerebrospinal fluid leaks. Surg Neurol. 2006. 65: 410-4
10. Khazim R, Dannawi Z, Spacey K, Khazim M, Lennon S, Reda A. Incidence and treatment of delayed symptoms of CSF leak following lumbar spinal surgery. Eur Spine J. 2015. p.
11. Kogias E, Klingler JH, Franco Jimenez P, Vasilikos I, Sircar R, Scholz C. Incidental durotomy in open versus tubular revision microdiscectomy: A retrospective controlled study on incidence, management and outcome. J Spinal Disord Tech. 2015. p.
12. Mihlon F, Kranz PG, Gafton AR, Gray L. Computed tomography-guided epidural patching of postoperative cerebrospinal fluid leaks. J Neurosurg Spine. 2014. 21: 805-10
13. Park Y, Lee SB, Seok SO, Jo BW, Ha JW. Perioperative surgical complications and learning curve associated with minimally invasive transforaminal lumbar interbody fusion: A single-institute experience. Clin Orthop Surg. 2015. 7: 91-6
14. Ross DA. Complications of minimally invasive, tubular access surgery for cervical, thoracic, and lumbar surgery. Minim Invasive Surg 2014. 2014. p.
15. Scholz C, Hubbe U, Kogias E, Klingler JH. Incomplete resection of lumbar synovial cysts – Evaluating the risk of recurrence. Clin Neurol Neurosurg. 2015. 136: 29-32
16. Tsahtsarlis A, Wood M. Minimally invasive transforaminal lumber interbody fusion and degenerative lumbar spine disease. Eur Spine J. 2012. 21: 2300-5

