

- Department of Ortho-Spine Surgery Sir Ganga Ram Hospital, New Delhi, India.
- Department of Anesthesiology, Sir Ganga Ram Hospital, New Delhi, India.
Correspondence Address:
Nitin Adsul
Department of Ortho-Spine Surgery Sir Ganga Ram Hospital, New Delhi, India.
DOI:10.25259/SNI_745_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Arth Patel1, Nitin Adsul1, Shvet Mahajan2, R. S. Chahal1, K. L. Kalra1, Shankar Acharya1. Incidental unintentional breakage of epidural catheter in supralaminar area: A case report. 30-Mar-2021;12:129
How to cite this URL: Arth Patel1, Nitin Adsul1, Shvet Mahajan2, R. S. Chahal1, K. L. Kalra1, Shankar Acharya1. Incidental unintentional breakage of epidural catheter in supralaminar area: A case report. 30-Mar-2021;12:129. Available from: https://surgicalneurologyint.com/surgicalint-articles/10680/
Date of Submission
20-Oct-2020
Date of Acceptance
05-Feb-2021
Date of Web Publication
30-Mar-2021
Abstract
Background: Among some of the known complications, breakage of epidural catheter, though is extremely rare, is a well-established entity. Visualization of retained catheter is difficult even with current radiological imaging techniques, and active surgical intervention might be necessary for removal of catheter fragment. We report such a case of breakage of an epidural catheter during its insertion which led to surgical intervention.
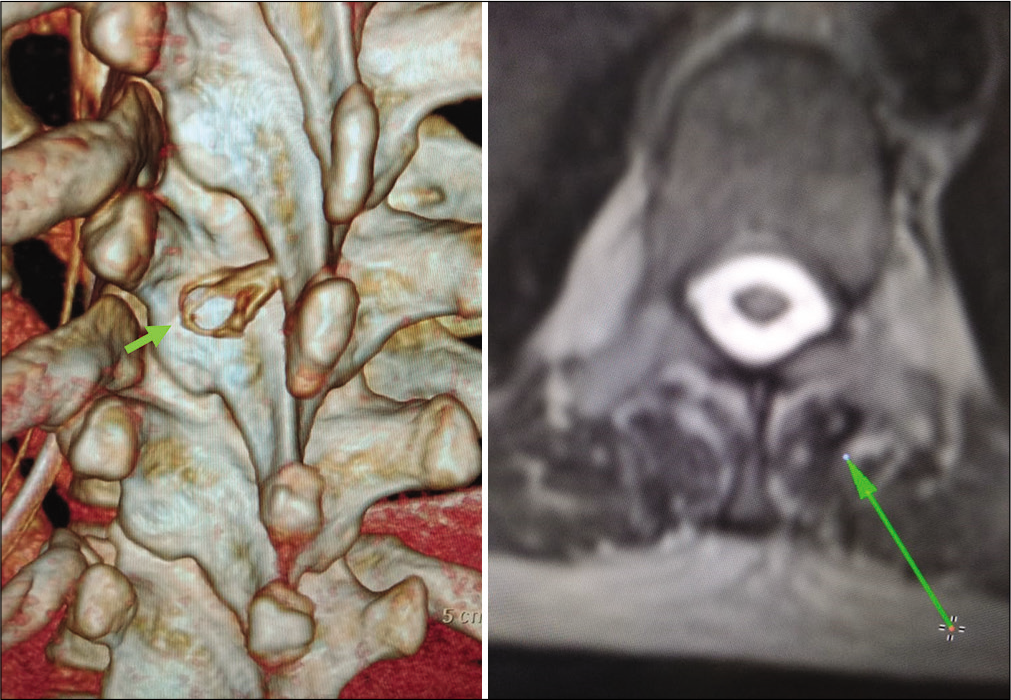
Case Description: A 52-year-old, an 18G radiopaque epidural catheter was inserted through an 18G Tuohy needle into the epidural space at T8-T9 interspace in left lateral position. Resistance was encountered. While the catheter was being removed with gentle traction along with Tuohy needle, it sheared off at 12 cm mark. After informing the operating surgeon and the patient, immediately an magnetic resonance imaging and computed tomography (CT) scan were done. CT scan with sagittal and coronal reconstruction was done. Epidural catheter was visualized at D9 lamina-spinous process junction who was removed by surgical intervention.
Conclusion: Leaving of epidural catheter puts the anesthetist in a dilemma. To evade such an event, it is important to stick to the traditional guiding principle for epidural insertion and removal. In spite of safety measures, if event occurs, the patient should be informed about it. Surgery is reserved for symptomatic patients or asymptomatic patients to avoid future complications.
Keywords: Catheter breakage, Catheter fragment, Epidural catheter
INTRODUCTION
Epidural catheter placement in epidural space is a common practice for providing anesthesia in many of the surgical procedures.[
CASE REPORT
A 52-year-old, 75 kg female, was admitted for liver transplant donor, a thoracic epidural was planned to provide intra-operative pain relief and improve hemodynamic stability as well as to provide postoperative analgesia. Using the loss-of-resistance technique, an 18G radiopaque epidural catheter (Perifix® Mini Set - B. Braun) was inserted through an 18G Tuohy needle into the epidural space at T8-T9 interspace in left lateral position in two attempts. Epidural space was encountered at 6 cm at the skin and catheter was inserted 17 cm at the hub of the needle. Resistance was encountered while giving test dose and therefore it was decided to relocate the epidural space. While the catheter was being removed with gentle traction along with Tuohy needle, it sheared off at 12 cm mark. After informing the operating surgeon and the patient, immediately an magnetic resonance imaging (MRI) and computed tomography (CT) scan were done. CT scan with sagittal and coronal reconstruction was done. Epidural catheter was visualized at D9 lamina-spinous process junction [
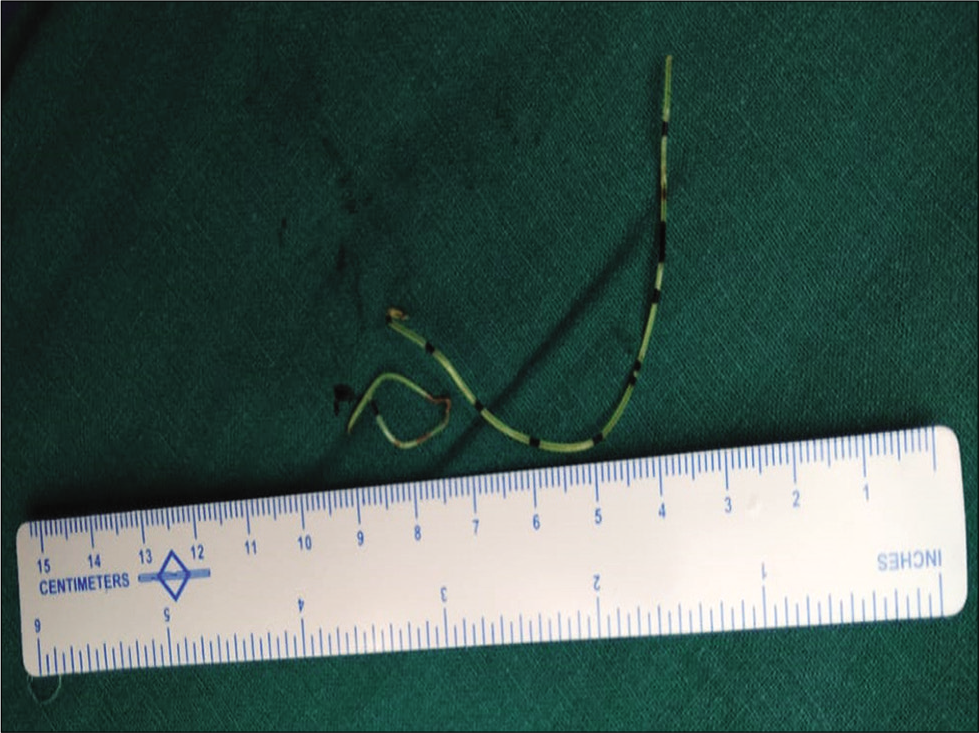
Urgent spine surgeon’s opinion was taken for removal of broken catheter. The patient and his relatives were well informed and counseled regarding the complication. A 3 cm incision was taken at the site of insertion of epidural catheter (D8-D9 space). The surgeons gently removed the epidural catheter after dissecting through the subperiosteal plane, and catheter was found lying at D9 lamina-spinous process junction. Hemostasis achieved and closure done in layers. A total length of 12 cm of epidural catheter was retrieved [
DISCUSSION
Epidural catheterization is a harmless procedure and is associated with low complication rate. Rupture of the epidural catheter during insertion or removal in the epidural space is a rare complication, and only few cases have been documented.[
All patients with retained epidural catheter piece should undergo suitable imaging studies to know its precise location. It is also necessary for documentation purposes and asymptomatic patients for timely follow-up so that early possible diagnosis of symptoms can be done. Of these radiographies, CT, ultrasonography, and MRI all have been used.[
However, radiological imaging tests are not very helpful in locating the free catheter even though the catheter is radiopaque. The reason may be slight thickness of the epidural catheter and the fact that surrounding tissue is very radiodense,[
If the epidural catheter breaks during removal, the presence of free catheter fragment should be properly documented and should also be conveyed to the surgical team as well as to the patient. The patient must be assured that occurrence of neurological sequel is rare and must be informed about treatment options available in such cases.[
Neurological consequences of a broken catheter are rare, surgical intervention is indicated only in complicated cases such as leaking CSF through the catheter[
CONCLUSION
Leaving of epidural catheter puts the anesthetist in a dilemma. To evade such an event, it is important to stick to the traditional guiding principle for epidural insertion and removal. In spite of safety measures, if event occurs, the patient should be educated about it. Surgery is reserved for symptomatic patient. Asymptomatic case is managed conservative which consists of imaging studies to document the position of the shattered fragment and close follow-up to recognize the complications which may progress in future.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Blanchard N, Clabeau JJ, Ossart M, Dekens J, Legars D, Tchaoussoff J. Radicular pain due to a retained fragment of epidural catheter. Anesthesiology. 1997. 87: 1567-9
2. de Souza Hobaika AB. Breakage of epidural catheters: Etiology, prevention, and management. Rev Bras Anestesiol. 2008. 58: 227-33
3. Hippalgaonkar AV, Kudalkar AG, Gaikwad SM, Modak S, Gupta HB, Tendolkar BA. Successful management of a broken epidural catheter!!!. Saudi J Anaesth. 2017. 11: 228-31
4. Lee YH, Hwang HY, Sim WS, Yang M, Lee CJ. Breakage of a thoracic epidural catheter during its removal-a case report. Korean J Anesthesiol. 2010. 58: 569-72
5. Mitra R, Fleischmann K. Management of the sheared epidural catheter: Is surgical extraction really necessary?. J Clin Anesth. 2007. 19: 310-4
6. Pant D, Jain P, Kanthed P, Sood J. Epidural catheter breakage: A dilemma. Indian J Anaesth. 2007. 51: 434-7
7. Staats P, Stinson S, Lee R. Lumbar stenosis complicating retained epidural catheter tip. Anesthesiology. 1995. 83: 1115-8
8. Ugboma S, Au-Truong X, Kranzler LI, Rifai SH, Joseph NJ, Salem MR. The breaking of an intrathecally-placed epidural catheter during extraction. Anesth Analg. 2002. 95: 1087-9

