

- Department of Surgery, Chiang Mai University, Chiang Mai, Thailand.
- Department of Radiology, Mahidol University, Bangkok, Thailand.
- Department of Surgery, Mahidol University, Bangkok, Thailand.
Correspondence Address:
Jirapong Vongsfak, Department of Surgery, Chiang Mai University, Chiang Mai, Thailand.
DOI:10.25259/SNI_905_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jirapong Vongsfak1,2, Jarudetch Wichaitum2, Thaweesak Aurboonyawat2,3. Infundibular dilatation perforating vessel of anterior communicating artery. 11-Nov-2022;13:525
How to cite this URL: Jirapong Vongsfak1,2, Jarudetch Wichaitum2, Thaweesak Aurboonyawat2,3. Infundibular dilatation perforating vessel of anterior communicating artery. 11-Nov-2022;13:525. Available from: https://surgicalneurologyint.com/surgicalint-articles/11991/
Date of Submission
01-Oct-2022
Date of Acceptance
01-Nov-2022
Date of Web Publication
11-Nov-2022
Abstract
Background: Infundibular dilatation at cerebral arteries is primary located at the posterior communicating artery. This report describes a rare case of infundibular dilatation perforating the branch of an anterior communication artery (AcomA) which mimicked an AcomA aneurysm.
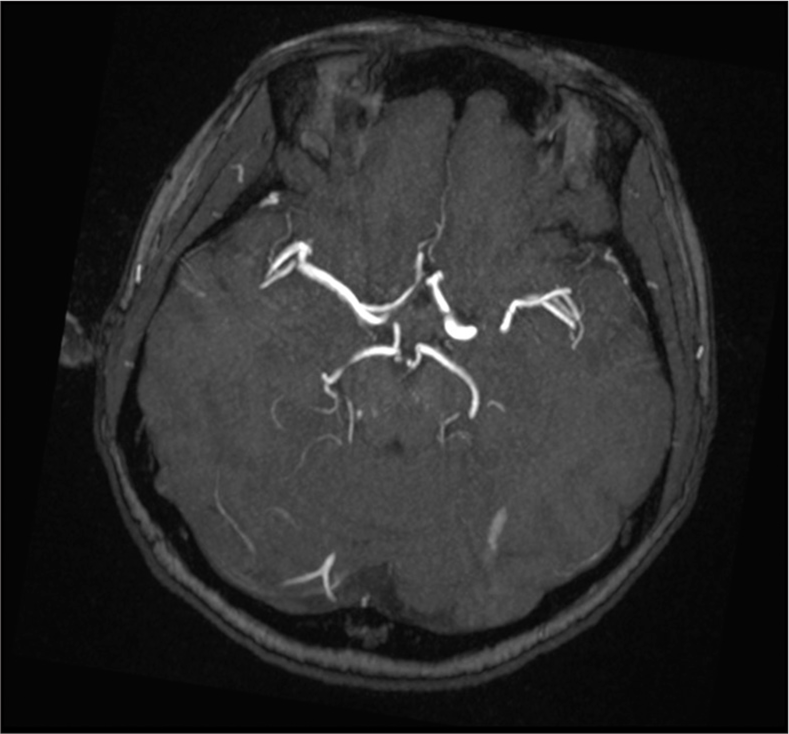
Case Description: The 54-year-old female presented with acute headache in the left temporal area with the right hemianesthesia. The magnetic resonance imaging and magnetic resonance angiography of the brain revealed a small outpouching lesion arising from the medial wall of the proximal A2 of the left ACA presenting as a suspected AcomA aneurysm. The cerebral angiogram showed a funnel-shaped dilatation of the anterior communicating artery with a single perforating branch arising from a dome size 1.4 × 1.1 mm, compatible with an infundibular dilatation perforating a branch of the AcomA.
Conclusion: The infundibular dilatation perforating vessel of AcomA is a rare condition and can mimic an AcomA aneurysm. Three-dimensional angiography helps to evaluate differentiation of the characteristics enabling accurate diagnosis.
Keywords: Anterior communicating artery, Cerebral aneurysm, Infundibular, Perforating branch
INTRODUCTION
An infundibular dilatation is defined as funnel or conical shaped widening at the origin of a cerebral artery. The infundibular origin is most commonly found at the origin of the posterior communicating artery (7–25%).[
In this paper, we are reporting on a rare case of infundibular perforating branch of anterior communicating aneurysm that was misinterpreted as a cerebral aneurysm.
CASE PRESENTATION
A 54-year-old female with dyslipidemia presented with acute right hemianesthesia with headache in the left temporal area. The physical examination revealed impaired sensation of the left side of the face (ophthalmic branch of the trigeminal nerve). The patient was sent for an magnetic resonance imaging (MRI) scan of the brain (May 26, 2022). The brain MRI showed a small outpouching lesion arising from the medial wall of the proximal A2 of the left ACA, pointing in the superomedial direction and measuring about 2 mm in neck width and height, and presenting as a suspected saccular aneurysm [
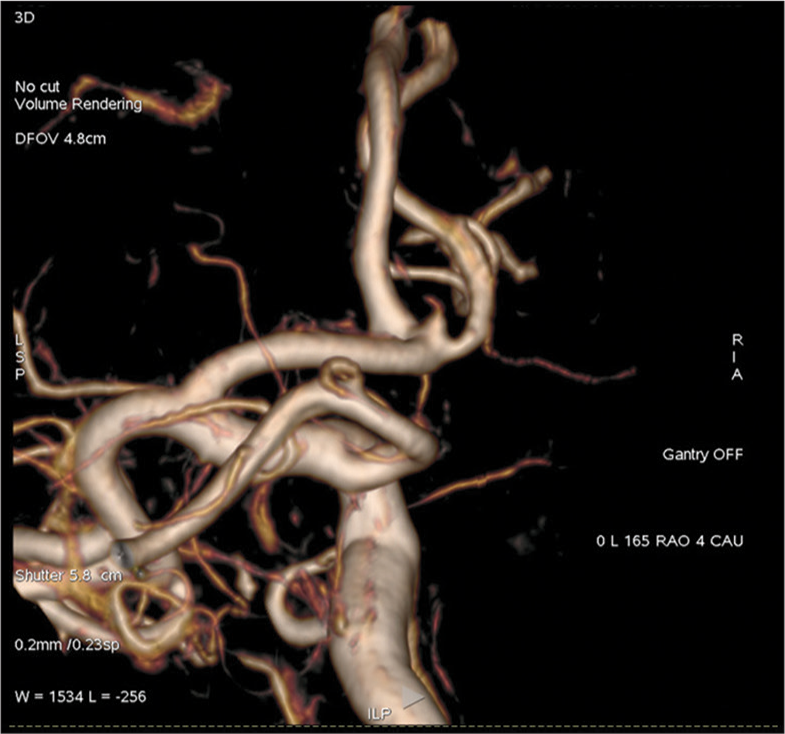
A four vessels cerebral angiogram was performed on July 6, 2022 and revealed a funnel-shaped dilatation of the anterior communicating artery with a single perforating branch arising from a dome sized 1.4 × 1.1 mm. The images from the three-dimension angiography are shown in
DISCUSSION
Infundibular dilatation of cerebral arteries presents as a conical, round dilated shape, <3 mm in size with a vessel arising from apex of the dome. An infundibulum is found in 5–25% of cerebral angiograms.[
An infundibular dilatation can also be found at the origins of the anterior choroidal artery and ophthalmic artery.[
Human cadaveric studies have demonstrated branches of the AComA that divide into small and large branches. The small branches supply the lamina terminalis and the hypothalamus at the preoptic region. The large branches are the medial artery of the corpus callosum and subcallosal artery. In our study, the perforating artery that arose from the infundibular dilatation of the AComA was suspected to be the subcallosal artery due to the shorter segment supply in the medial hemispheric surface shown by the three-dimension angiography.[
The natural history of the infundibular dilatation has been considered to be an anatomical variant which is not associated with pathological significance. However, there are reports of infundibular dilatation developing in aneurysms in the posterior communicating artery and subsequently rupturing.[
CONCLUSION
The occurrence of infundibular perforating vessel of AcomA is a rare condition and as described above can mimic an AcomA aneurysm. Three-dimensional angiography needs to be performed to evaluate the lesion and enable differentiation of the characteristics enabling accurate diagnosis. However, the natural history of these lesions is still not well understood and there is a need for more detailed follow-up and more reports in the future.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Epstein F, Ransohoff J, Budzilovich GN. The clinical significance of junctional dilatation of the posterior communicating artery. J Neurosurg. 1970. 33: 529-31
2. Karekezi C, Boutarbouch M, Djoubairou B, Melhaoui A, Arkha Y, El Ouahabi A. Are infundibular dilatations at risk of further transformation? Ten-year progression of a prior documented infundibulum into a saccular aneurysm and rupture: Case report and a review of the literature. Neurochirurgie. 2014. 60: 307-11
3. Kihira S, Fifi JT, Doshi AH, Xuan D, Belani P. Infundibulum at the origin of an accessory middle cerebral artery. Clin Imaging. 2021. 72: 19-21
4. Marinković S, Milisavljević M, Marinković Z. Branches of the anterior communicating artery. Acta Neurochir (Wien). 1990. 106: 78-85
5. Morris P, editors. Practical Neuroangiography. United States: Lippincott Williams and Wilkins; 2007. p.
6. Narducci A, Ronchetti G, Nannucci F, Vaudano GP, Griva F. Infundibulum of accessory anterior cerebral artery: Rare, likely benign malformation of anterior communicating artery complex to keep in mind. World Neurosurg. 2019. 132: 399-402
7. Park J, Kang DH. Infundibular widening mimicking anterior communicating artery aneurysm: Report of 2 cases. J Neurosurg. 2013. 119: 243-6

