

Intractable hiccups and neck pain due to left C4 radiculopathy decreased with posterior foraminotomy
- Department of Neurosurgery, Hikone Chuo Hospital, Hikone, Japan.
- Department of Neurosurgery, Otsu City Hospital, Otsu, Japan.
Correspondence Address:
Yoshinori Maki, Department of Neurosurgery, Hikone Chuo Hospital, Hikone, Japan.
DOI:10.25259/SNI_119_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yoshinori Maki1, Toshinari Kawasaki2, Motohiro Takayama2. Intractable hiccups and neck pain due to left C4 radiculopathy decreased with posterior foraminotomy. 25-Feb-2022;13:74
How to cite this URL: Yoshinori Maki1, Toshinari Kawasaki2, Motohiro Takayama2. Intractable hiccups and neck pain due to left C4 radiculopathy decreased with posterior foraminotomy. 25-Feb-2022;13:74. Available from: https://surgicalneurologyint.com/surgicalint-articles/11407/
Date of Submission
28-Jan-2022
Date of Acceptance
08-Feb-2022
Date of Web Publication
25-Feb-2022
Abstract
Background: Intractable hiccups can last for more than 1–2 months and can occur, as shown in this case study, due to cervical nerve root compression.
Case Description: A 76-year-old male presented with intractable hiccups and neck pain of 7 months’ duration. The patient underwent magnetic resonance imaging studies of the entire neuraxis. The only abnormality found was on the cervical magnetic resonance images that demonstrated left C4 nerve root compression due to the C3– C4 lateral/foraminal osteophyte. Following a left-sided C3–C4 laminoforaminotomy, the hiccups and the neck pain improved.
Conclusion: A 76-year-old male presented with intractable hiccups and neck pain attributed to a left C3/C4 lateral/foraminal spondylotic ridge. Following a left C3–C4 laminoforaminotomy, the frequency of hiccup attacks remained the same, but their duration was markedly shortened to 30 s, while the neck pain improved.
Keywords: C4 nerve root, Intractable hiccups, Laminoforaminotomy, Neck pain, Radiculopathy
INTRODUCTION
Persistent hiccups and intractable hiccups are, respectively, defined based on their duration: more than 24–48 h and more than 1-2 months.[
CASE PRESENTATION
A 76-year-old male presented neurologically intact, but with neck pain of 9 months duration, and 7 months of intractable hiccups. Notably, the hiccup attacks occurred 20–80 times/day, each lasting approximately 15 min. Upper endoscopy and abdominal computed tomography studies were negative. The patient underwent magnetic resonance imaging (MRI) studies of the entire neuraxis. When the cervical MRI revealed left C4 foraminal nerve root-osteophytic compression, left C3–C4 laminoforaminotomy was performed [
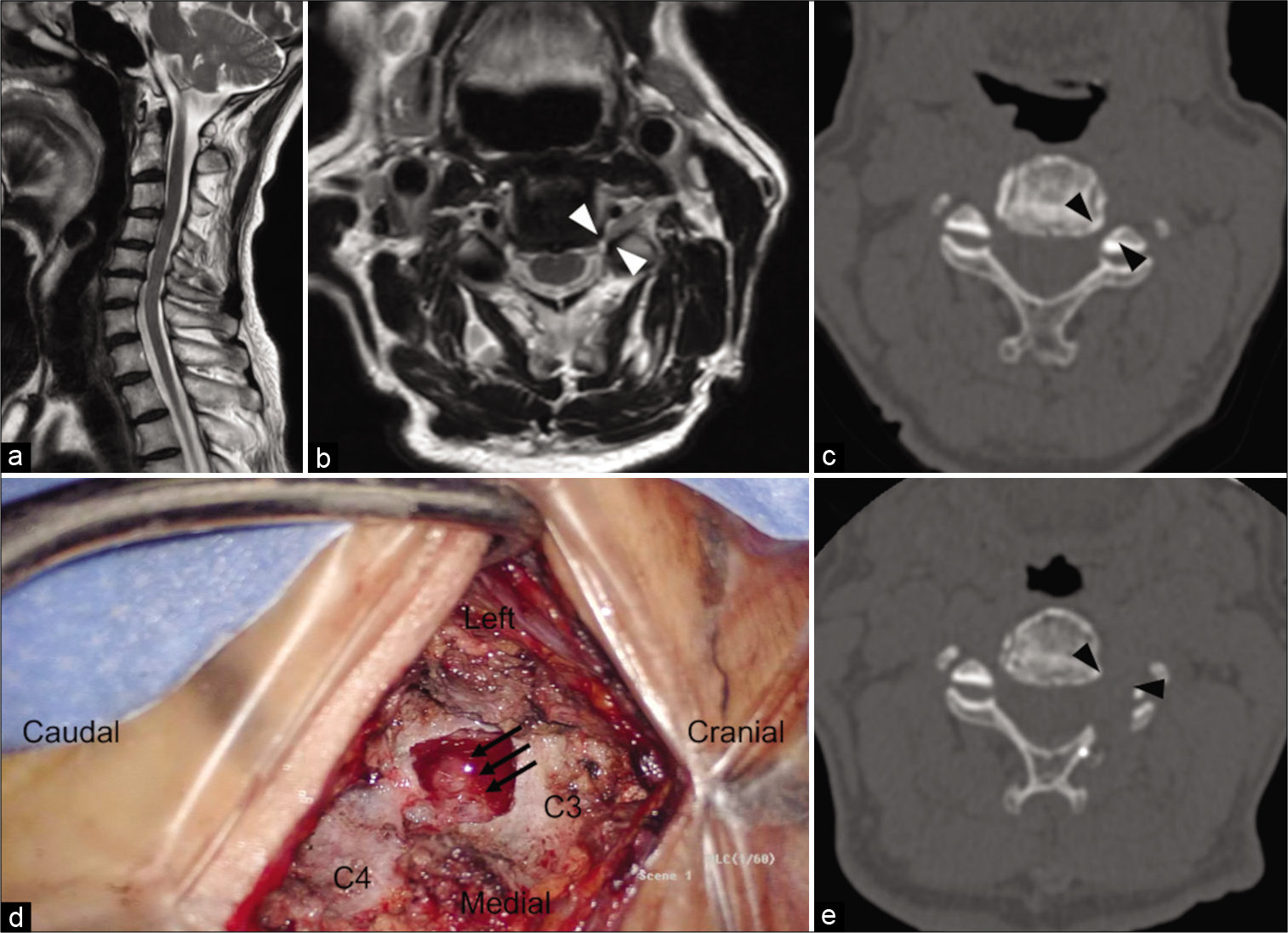
Figure 1:
(a) Preoperative sagittal magnetic resonance image (MRI). Apparent cervical spinal cord stenosis is not observed. (b) An axial MRI at the level of the bilateral C4 nerve roots. Left foramen stenosis of the C4 nerve root is visible (white arrow heads). (c) A computed tomography image showing osteophytes causing left foramen stenosis of the C4 nerve root. The ventral and dorsal roots of C4 are compressed (black arrow heads). (d) The left C4 nerve root is posteriorly decompressed (triple arrows). (e) A postoperative computed tomography image showing release of the left C4 nerve root (black arrow heads).
DISCUSSION
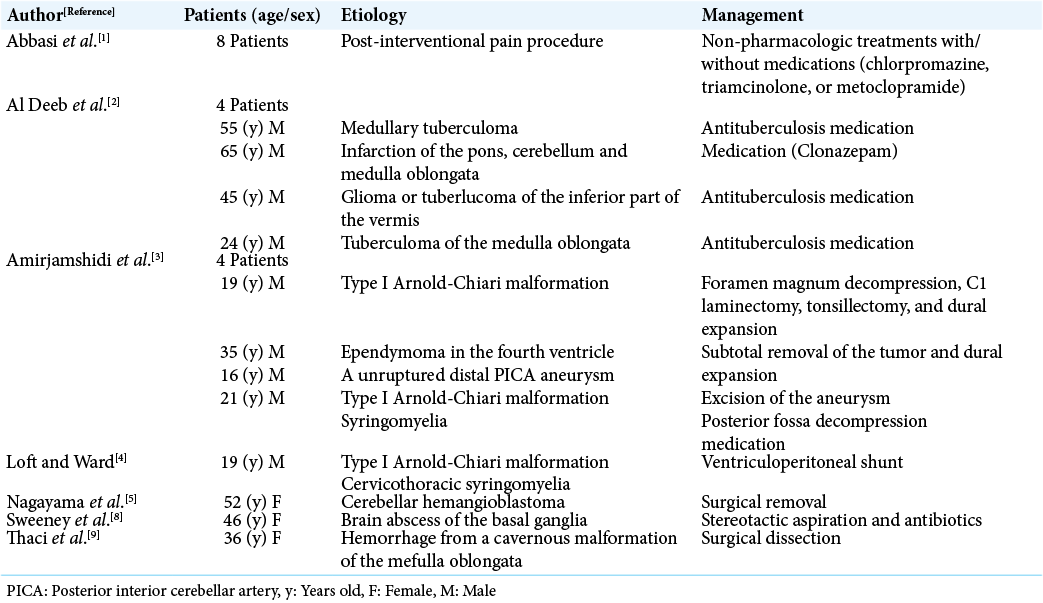
Lesions that continuously irritate the afferent, central, and efferent pathways of the hiccup reflex may result in intractable hiccups [
CONCLUSION
A 76-year-old male with intractable hiccups/neck pain attributed to a left C4 root compression/C3–C4 osteophyte formation, experienced marked improvement in his hiccups (i.e., attacks markedly shortened to 30 s), and radiculopathy following a left C3–C4 laminoforaminotomy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abbasi A, Roque-Dang CM, Malhotra G. Persistent hiccups after interventional pain procedures: A case series and review. PM R. 2012. 4: 144-51
2. Al Deeb SM, Sharif H, Al Moutaery K, Biary N. Intractable hiccup induced by brainstem lesion. J Neurol Sci. 1991. 103: 144-50
3. Amirjamshidi A, Abbassioun K, Parsa K. Hiccup and neurosurgeons: A report of 4 rare dorsal medullary compressive pathologies and review of the literature. Surg Neurol. 2007. 67: 395-402
4. Loft LM, Ward RF. Hiccups. A case presentation and etiologic review. Arch Otolaryngol Head Neck Surg. 1992. 118: 1115-9
5. Nagayama T, Kaji M, Hirano H, Niiro M, Kuratsu J. Intractable hiccups as a presenting symptom of cerebellar hemangioblastoma. Case report. J Neurosurg. 2004. 100: 1107-10
6. Padmanaban V, Payne R, Corbani K, Corl S, Rizk EB. Phrenic nerve stimulator placement via the cervical approach: Technique and anatomic considerations. Oper Neurosurg. 2021. 21: E215-20
7. Prates AG, Vasques LC, Bordoni LS. Anatomical variations of the phrenic nerve: An actualized review. J Morphol Sci. 2015. 32: 53-6
8. Sweeney J, Bodman A, Hall WA. Brain abscess of basal ganglia presenting with persistent hiccups. World Neurosurg. 2018. 112: 182-5
9. Thaci B, Burns JD, Delalle I, Vu T, Davies KG. Intractable hiccups resolved after resection of a cavernous malformation of the medulla oblongata. Clin Neurol Neurosurg. 2013. 115: 2247-50

