

- Department of Neurosurgery, Desert Regional Medical Center, Palm Springs, California, United States.
- Department of Neurosurgery, Banner – University Medical Center Phoenix, Phoenix, Arizona, United States.
- Department of Neurology, Redlands Community Hospital, Redlands, California, United States.
- Department of Neurosurgery, University of Washington, Seattle, Washington, United States.
- College of Osteopathic Medicine, William Carey University, Hattiesburg, Mississippi, United States.
- Department of Neurosurgery, Redlands Community Hospital, Redlands, California, United States.
Correspondence Address:
Brian Fiani, D.O. Department of Neurosurgery, Desert Regional Medical Center, Palm Springs, California, United States.
DOI:10.25259/SNI_1195_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohammad Arshad1, Tiffany Odell2, Brian Fiani1, Hamid Hadi1, Eli Johnson3, Chao Li1, John Ogunlade4, Brian Musch5, Michael Schiraldi6. Intraoperative localization and “snowman” muscle pledget repair for ventral dural defect in a case of spontaneous intracranial hypotension. 04-Feb-2022;13:39
How to cite this URL: Mohammad Arshad1, Tiffany Odell2, Brian Fiani1, Hamid Hadi1, Eli Johnson3, Chao Li1, John Ogunlade4, Brian Musch5, Michael Schiraldi6. Intraoperative localization and “snowman” muscle pledget repair for ventral dural defect in a case of spontaneous intracranial hypotension. 04-Feb-2022;13:39. Available from: https://surgicalneurologyint.com/surgicalint-articles/11367/
Date of Submission
01-Dec-2021
Date of Acceptance
18-Jan-2022
Date of Web Publication
04-Feb-2022
Abstract
Background:
Case Description: Procedure took place in a hybrid biplane operating room so that simultaneous digital subtraction myelogram may also be performed for intraoperative localization. Dural defect was identified intraoperatively and repaired with thoracic laminectomy and “snowman” muscle pledget technique. Postoperatively, the patient did well with resolution of his symptoms.
Conclusion: The authors have proposed a grading scale to aid in the work up and management of intracranial hypotension. The use of a hybrid biplane operating room and “snowman” muscle pledget technique is a safe and effective technique to treat spontaneous spinal CSF leaks resulting from dural defects.
Keywords: Aliquorrhea, Calcified thoracic disc, Hybrid biplane operating room, Spontaneous intracranial hypotension, Spontaneous spinal CSF leak
INTRODUCTION
A 49-year-old male presented to hospital with 2 weeks of orthostatic headaches and diplopia without any history of blunt trauma. On arrival, the patient’s examination was significant for the right-sided abducens palsy without other neurological deficits. Workup included magnetic resonance imaging (MRI) brain with and without contrast demonstrated diffuse meningeal enhancement. Lumbar puncture was performed and opening pressure was noted to be 4 cm H2O. Intracranial hypotension was suspected and the patient underwent CT myelogram [
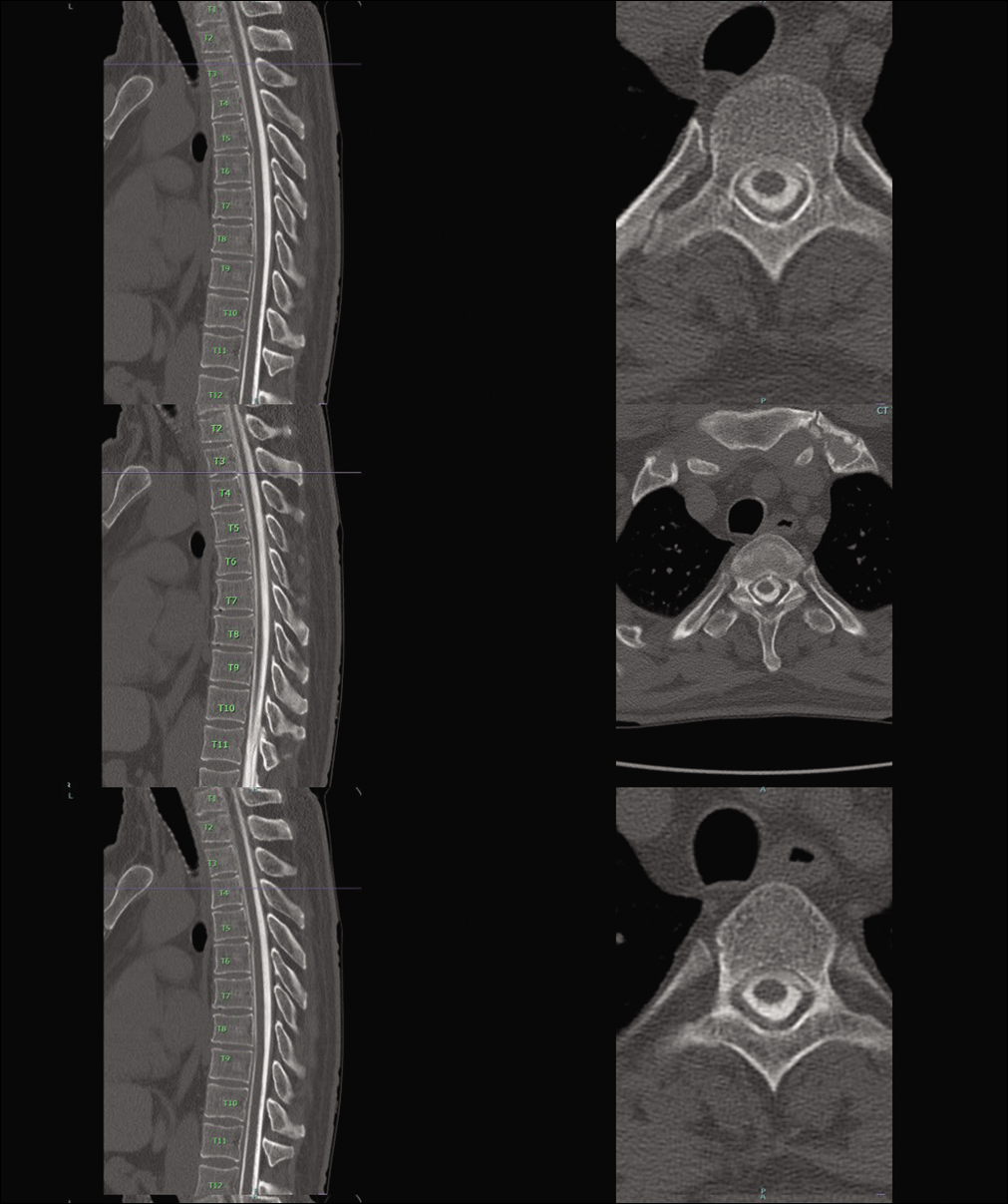
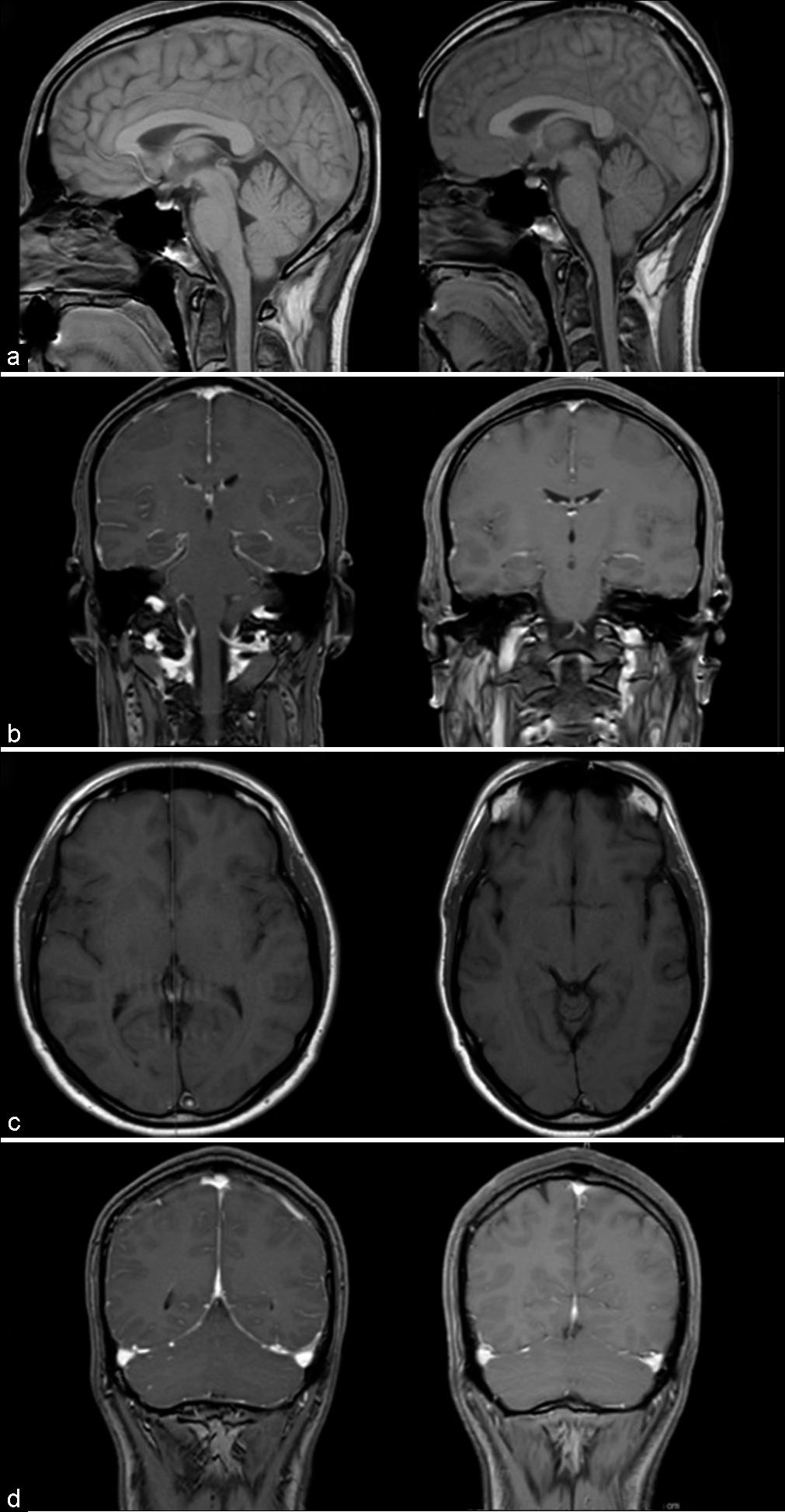
Figure 2:
Comparison of MRI findings of spontaneous intracranial hypotension preoperatively (left) and postoperatively (right). Cerebellar ectopia, elevated pontomamillary distance, and pituitary hyperemia all noted to trend toward resolution (a). Diffuse meningeal enhancement resolved postoperatively (b). Venous congestion noted by bulging circular superior sagittal sinus and transverse sinuses noted to decrease on postoperative imaging (c and d).
CASE DESCRIPTION
This is the first reported use of hybrid biplane operating room for intraoperative localization with DSM for treatment of SIH and also the first to describe the “snowman” pledget technique. The patient was positioned prone for a standard thoracic laminectomy. After exposure, DSM was completed to verify the site of spinal cerebrospinal fluid (CSF) leak (T3-4 disc space) [
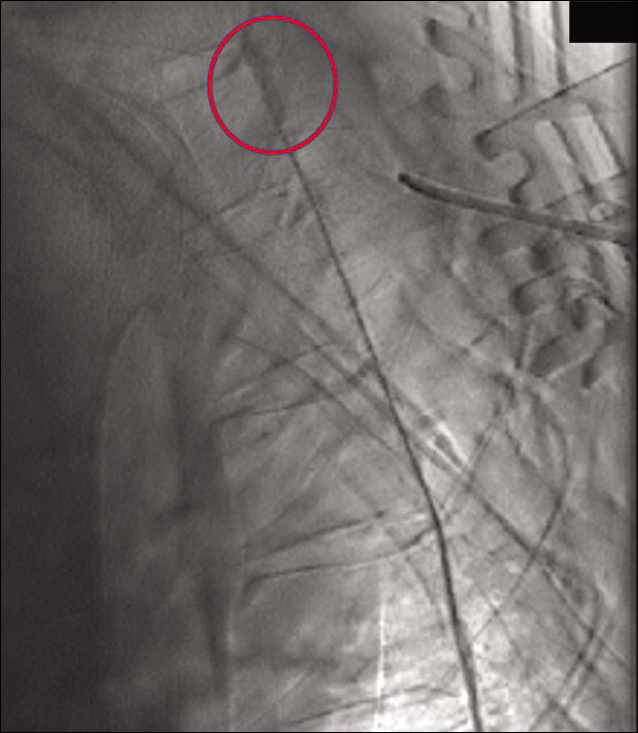
Figure 3:
Intraoperative digital subtraction myelography in operative biplane hybrid suite demonstrating contrast extravasation at T3-4 disc space (red). Penfield number 4 placed under lamina of T4 for localization. This technique allows real-time localization after dissection and exposure of posterior elements of vertebrae.
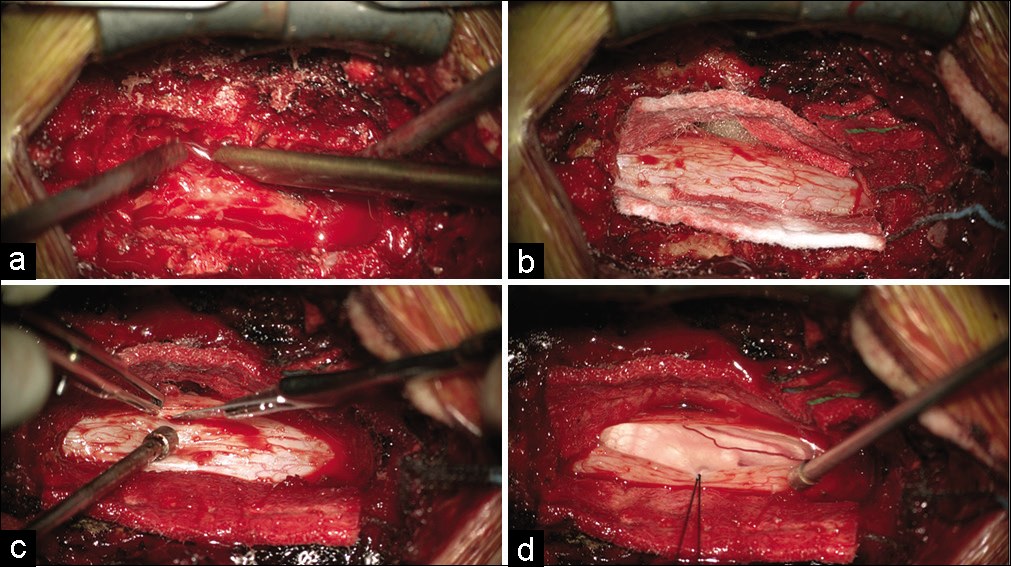
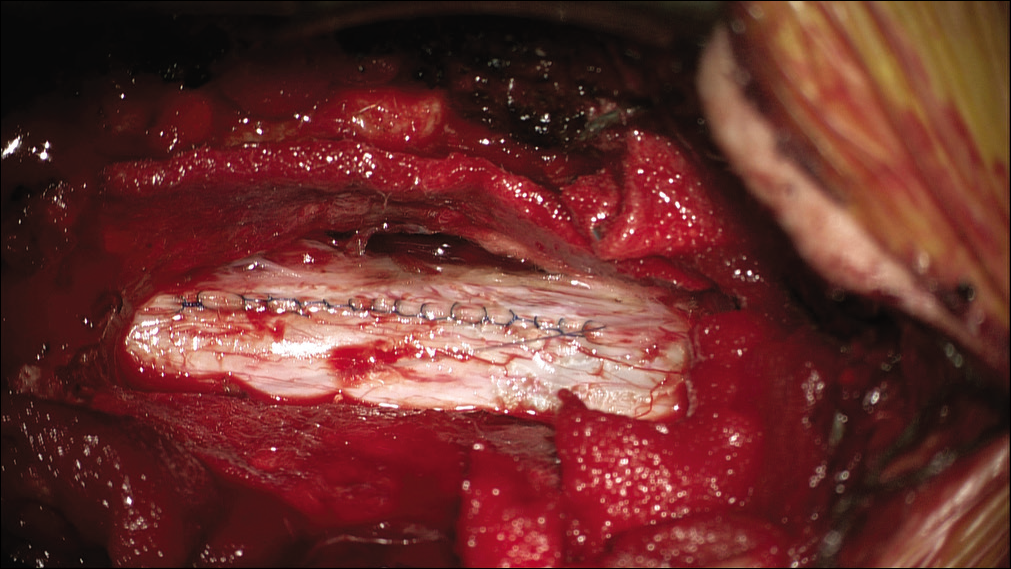
Figure 4:
Exposure and durotomy of thoracic spinal cord at level of cerebrospinal fluid leak. Partial pediculectomy of T4 completed so that there will be room to retract and work on ventral dural defect without manipulation of spinal cord. Also note pseudomembrane around thecal sac which may be mistaken as dura (a). Spinal cord exposed with hemostasis and adequate exposure laterally for dural retraction (b). Longitudinal posterior durotomy made with number 11 blade spanning along laminectomy (c). Dentate ligaments severed (not shown) and dura is tacked with silk for retraction (d).
A left paramedian durotomy along laminectomy defect was completed without compromising arachnoid. Once dura was opened, the neuromonitoring technician was requested to monitor motor evoked potentials every 2 min – with any change, the surgeon would immediately stop and respond. The dura was tented posterolaterally with suture and the dentate ligaments were released. The pediculectomy, laterality of durotomy. and release of dentate ligaments are key steps dural retraction and presentation of ventral dural tear without manipulation of the cord [
A paraspinal muscle graft was harvested to serve as a pledget. The graft was introduced intradurally and carefully pushed to the epidural space – providing a “snowman” effect. Care was taken to ensure no mass effect from pledget was exerted on the intradurally by visualization and neuromonitoring. Small amounts of dural sealant agent were then used on both intradural and epidural compartments to stabilize and reinforce seal around the pledget [
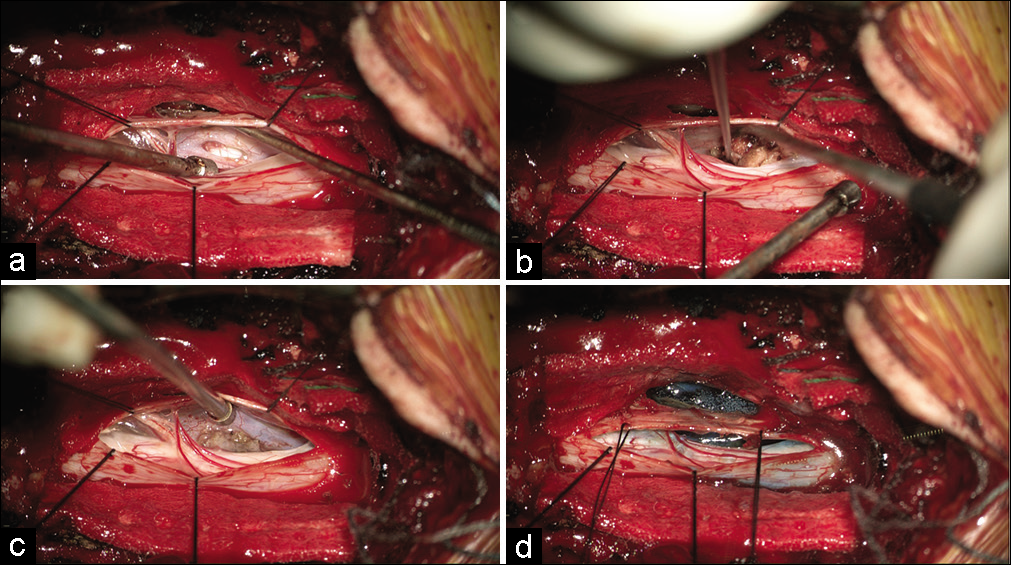
Figure 5:
Application of “snowman” muscle pledget technique. The ventral dural defect is appreciated with retraction of dura without manipulation of spinal cord (a). Muscle pledget is inserted into dural defect (b) and adjusted to a low intradural profile so that there is no mass effect on the spinal cord (c). Extradural and minimal intradural application of dural sealant is used to complete seal (d).
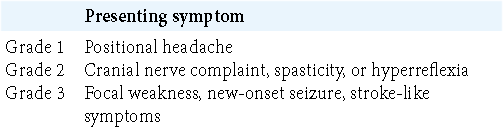
The authors have proposed a grading scale to aid in the work up and management of intracranial hypotension [
CONCLUSION
In this case, we localized a ventral dural defect with the assistance of intraoperative DSM then repaired the defect with the “snowman” pledget technique. This is the first report to illustrate this technique.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.

