

- Department of Neuroscience and Reproductive and Odontostomatological Sciences, University of Naples Federico II, Via Sergio Pansini, Naples, Bologna, Italy.
- Department of Biomedical and Neuromotor Sciences, Alma Mater Studiorum University of Bologna, Bologna, Italy.
- Department of Neurological Surgery, IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy.
- Department of ENT, Ospedale Bellaria, Bologna, Italy.
Correspondence Address:
Giovanni Miccoli
Department of Neurological Surgery, IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy.
DOI:10.25259/SNI_225_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Giovanni Miccoli, Emanuele La Corte, Ernesto Pasquini, Giorgio Palandri. Life-threatening delayed arterial hemorrhage following anterior cervical spine surgery: A case report and literature review. 23-May-2020;11:124
How to cite this URL: Giovanni Miccoli, Emanuele La Corte, Ernesto Pasquini, Giorgio Palandri. Life-threatening delayed arterial hemorrhage following anterior cervical spine surgery: A case report and literature review. 23-May-2020;11:124. Available from: https://surgicalneurologyint.com/surgicalint-articles/10043/
Date of Submission
27-Apr-2020
Date of Acceptance
07-May-2020
Date of Web Publication
23-May-2020
Abstract
Background: One of the most serious and potentially life-threatening adverse events associated with anterior cervical spine surgery is postoperative hematoma with acute airway obstruction. The causes of unpredicted delayed bleeding are, however, not fully elucidated. Here, we report a case of delayed arterial bleeding and sudden airway obstruction following a two-level ACDF.
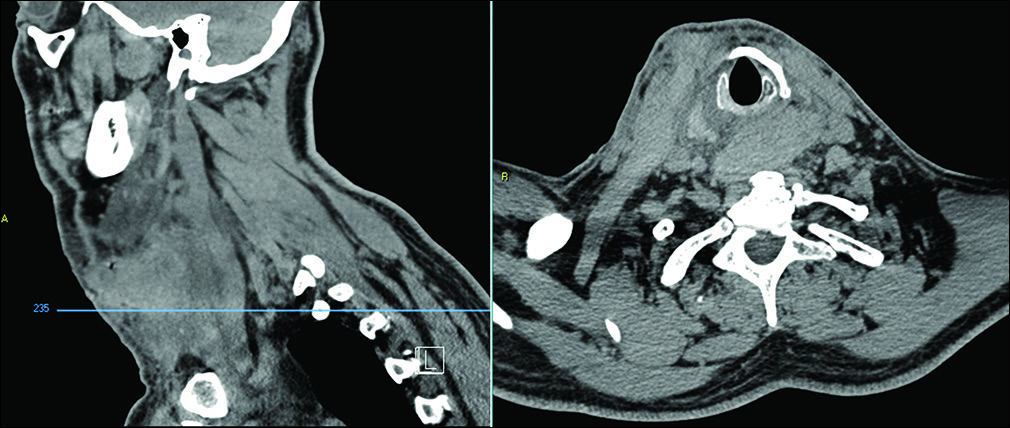
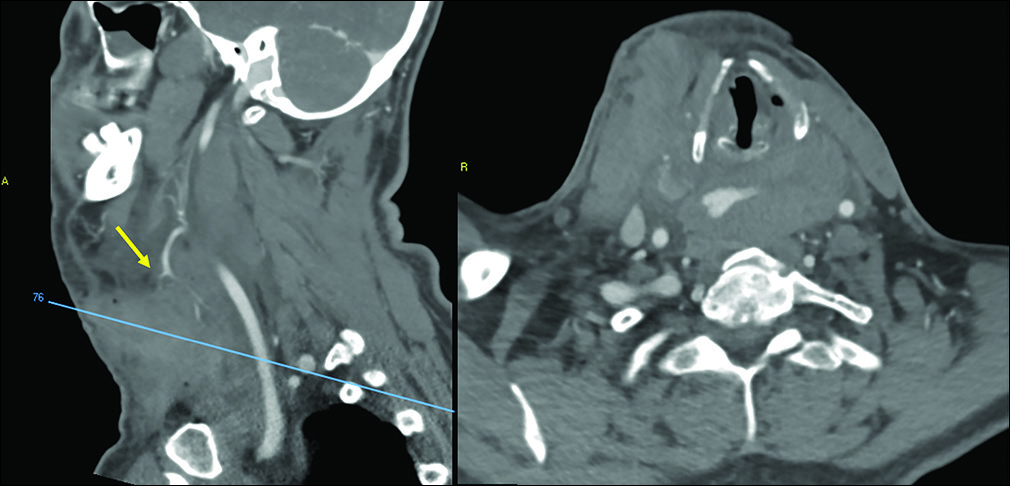
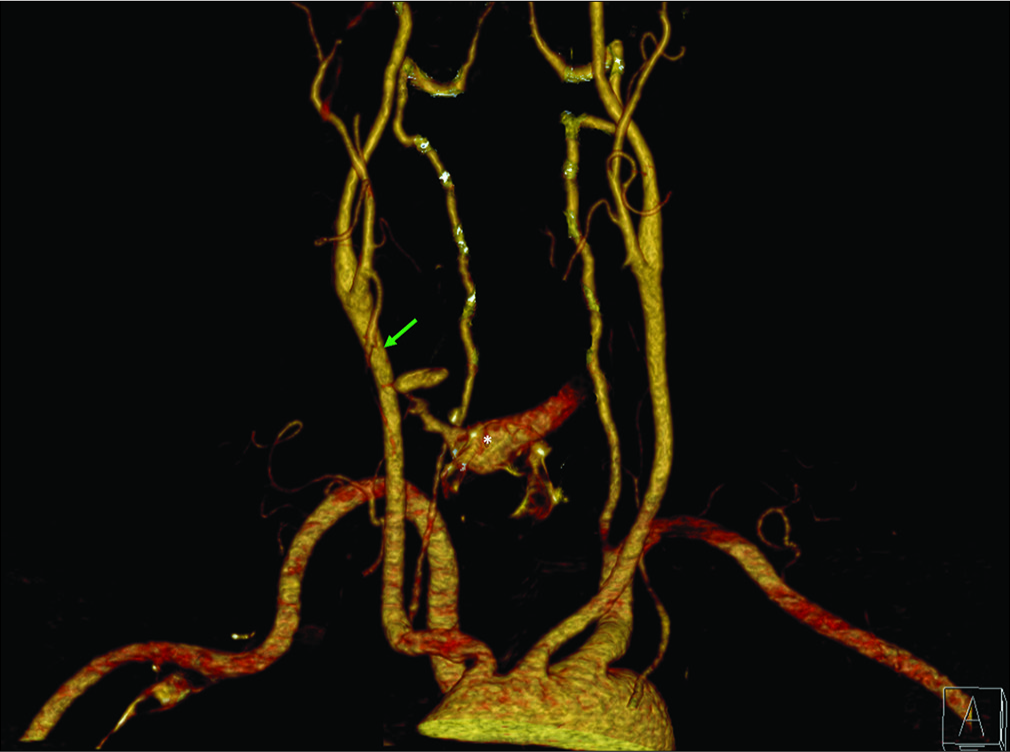
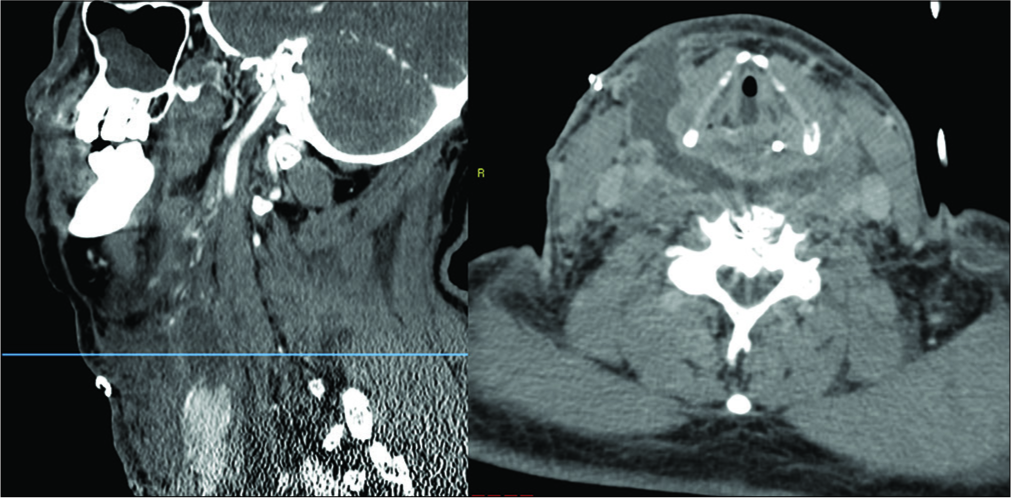
Case Description: A 52-year-old male presented with the right paracentral disc herniations at the C4–C5 and C5–C6 levels. A two-level ACDF was performed. Notably, on the 5th postoperative day, the patient developed an acute respiratory distress due to a large right lateral retrotracheal hematoma requiring emergency evacuation at the bedside. This was followed by formal ligation of a branch of the right superior thyroid artery in the operating room. In addition, an emergency tracheotomy was performed. By postoperative day 15, the tracheotomy was removed, and the patient was neurologically intact.
Conclusion: A superior thyroid artery hemorrhage should be suspected if a patient develops delayed neck swelling with or without respiratory decompensation several days to weeks following an ACDF. Notably, these hematomas should be immediately recognized and treated (i.e., decompression starting at the bedside and completed in the operating room) to prevent catastrophic morbidity or mortality.
Keywords: Anterior cervical discectomy and fusion, Delayed hemorrhage, Superior thyroid artery
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spinal operations.[
MATERIALS AND METHODS
Scopus and PubMed databases were queried using individual keywords and MeSH terms for identifying postoperative ACDF hematomas due to superior thyroid artery branch dissections.
CASE DESCRIPTION
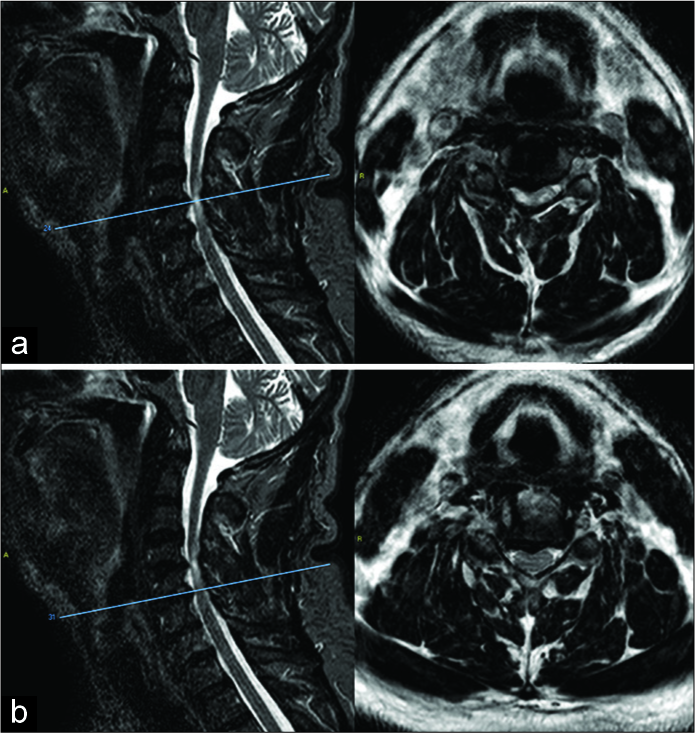
A 52-year-old male presented with bilateral cervicobrachialgia, bilateral arm paresthesias, and tetraparesis. The magnetic resonance imaging showed the right paracentral disc herniations at the C4–C5 [
DISCUSSION
Anterior cervical spine operations are among the most commonly performed procedures among spine surgeons and have low complication rates.[
Etiology of superior thyroid artery dissection
The etiology of superior thyroid artery dissection in our case remained unclear. Yu et al.[
Time of onset of postoperative hematomas due to ACDF
Most vascular arterial complications of ACDF are detected intraoperatively or in the early postoperative period.[
Delayed arterial bleeding leading to postoperative ACDF hematomas
Few cases report delayed arterial postoperative hematomas after ACDF. In our patient, the postoperative hemorrhage from a branch of superior thyroid artery was encountered on the 5th postoperative day. One report in the literature cited a hemorrhage following a C34/C45 ACDF as occurring 16 days postoperatively; it too was due to a superior thyroid artery dissection.[
CONCLUSION
Retropharyngeal hematomas are rare following anterior cervical surgery. They typically present acutely, within 6–12 postoperative hours, and occasionally from 3 to 7 days to up to 1 month postoperatively. Here, we presented a patient with a retrotracheal hematoma occurring 5 days following a C45/56 ACDF attributed to a hemorrhage from a branch of the superior thyroid artery.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Almefty RO, Albuquerque FC, Spetzler RF, Turner JD. Direct repair of iatrogenic vertebral artery injury associated with anterior cervical corpectomy: 2-dimensional operative video. Oper Neurosurg (Hagerstown). 2020. 18: E47-8
2. Badhiwala JH, Ellenbogen Y, Khan O, Nouri A, Jiang F, Wilson JR. Comparison of the inpatient complications and health care costs of anterior versus posterior cervical decompression and fusion in patients with multilevel degenerative cervical myelopathy: A retrospective propensity score-matched analysis. World Neurosurg. 2020. 134: e112-9
3. Bovonratwet P, Fu MC, Tyagi V, Bohl DD, Ondeck NT, Albert TJ. Incidence, risk factors, and clinical implications of postoperative hematoma requiring reoperation following anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 2019. 44: 543-9
4. Debkowska MP, Butterworth JF, Moore JE, Kang S, Appelbaum EN, Zuelzer WA. Acute post-operative airway complications following anterior cervical spine surgery and the role for cricothyrotomy. J Spine Surg. 2019. 5: 142-54
5. Dobies-Krześniak B, Tarnacka B. Vertebral artery dissection following cervical spine injury as a diagnostic challenge. Case study. Ortop Traumatol Rehabil. 2019. 21: 369-78
6. Guan Q, Chen L, Long Y, Xiang Z. Iatrogenic vertebral artery injury during anterior cervical spine surgery: A systematic review. World Neurosurg. 2017. 106: 715-22
7. Kashkoush A, Mehta A, Agarwal N, Nwachuku EL, Fields DP, Alan N. Perioperative neurological complications following anterior cervical discectomy and fusion: Clinical impact on 317,789 patients from the national inpatient sample. World Neurosurg. 2019. 128: e107-15
8. Lied B, Sundseth J, Helseth E. Immediate (0-6 h), early (6-72 h) and late (>72 h) complications after anterior cervical discectomy with fusion for cervical disc degeneration; discharge six hours after operation is feasible. Acta Neurochir (Wien). 2008. 150: 111-8
9. Lo WB, Nagaraja S, Saxena A. Delayed hemorrhage from an iatrogenic vertebral artery injury during anterior cervical discectomy and successful endovascular treatment-report of a rare case and literature review. World Neurosurg. 2017. 99: 811.e811-8
10. McGirt MJ, Rossi V, Peters D, Dyer H, Coric D, Asher AL. Anterior cervical discectomy and fusion in the outpatient ambulatory surgery setting: Analysis of 2000 consecutive cases. Neurosurgery. 2020. 86: E310-5
11. O’Neill KR, Neuman B, Peters C, Riew KD. Risk factors for postoperative retropharyngeal hematoma after anterior cervical spine surgery. Spine (Phila Pa 1976). 2014. 39: E246-52
12. Palumbo MA, Aidlen JP, Daniels AH, Bianco A, Caiati JM. Airway compromise due to laryngopharyngeal edema after anterior cervical spine surgery. J Clin Anesth. 2013. 25: 66-72
13. Patel DV, Yoo JS, Haws BE, Khechen B, Lamoutte EH, Karmarkar SS. Comparative analysis of anterior cervical discectomy and fusion in the inpatient versus outpatient surgical setting. J Neurosurg Spine. 2019. 26: 1-6
14. Ren H, Wang J, Yu L. Retropharyngeal hematoma following anterior cervical spine surgery: Lessons from a case report (CARE-compliant). Medicine (Baltimore). 2019. 98: e17247-
15. Sethi R, Tandon MS, Ganjoo P. Neck hematoma causing acute airway and hemodynamic compromise after anterior cervical spine surgery. J Neurosurg Anesthesiol. 2008. 20: 69-70
16. Song KJ, Choi BW, Lee DH, Lim DJ, Oh SY, Kim SS. Acute airway obstruction due to postoperative retropharyngeal hematoma after anterior cervical fusion: A retrospective analysis. J Orthop Surg Res. 2017. 12: 19-
17. Thakur NA, McDonnell M, Paller D, Palumbo M. Wound hematoma after anterior cervical spine surgery: In vitro study of the pathophysiology of airway obstruction. Am J Orthop (Belle Mead NJ). 2013. 42: E35-7
18. Wilson LA, Zubizarreta N, Bekeris J, Poeran J, Liu J, Fiasconaro M. Risk factors for reintubation after anterior cervical discectomy and fusion surgery: Evaluation of three observational data sets. Can J Anaesth. 2020. 67: 42-56
19. Yu NH, Jahng TA, Kim CH, Chung CK. Life-threatening late hemorrhage due to superior thyroid artery dissection after anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 2010. 35: E739-42

