

- Department of Neurosurgery, Hospital de Santa Maria, Lisbon,
- Department of Neurosurgery, CUF Cascais Hospital, Cascais, Portugal.
Correspondence Address:
José Hipólito-Reis, Department of Neurosurgery, Hospital de Santa Maria, Lisbon, Portugal.
DOI:10.25259/SNI_141_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: José Hipólito-Reis1, Diogo Roque1, Joaquim Cruz Teixeira2. Lumbar paraspinal intramuscular myxoma: A case report. 10-Mar-2023;14:86
How to cite this URL: José Hipólito-Reis1, Diogo Roque1, Joaquim Cruz Teixeira2. Lumbar paraspinal intramuscular myxoma: A case report. 10-Mar-2023;14:86. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12183
Date of Submission
10-Feb-2023
Date of Acceptance
24-Feb-2023
Date of Web Publication
10-Mar-2023
Abstract
Background: With an estimated incidence of about 1 case/million patients, paravertebral intramuscular myxomas represent a rare cause of lumbar pain. Rather, they typically occur in the heart and in bone tissues.
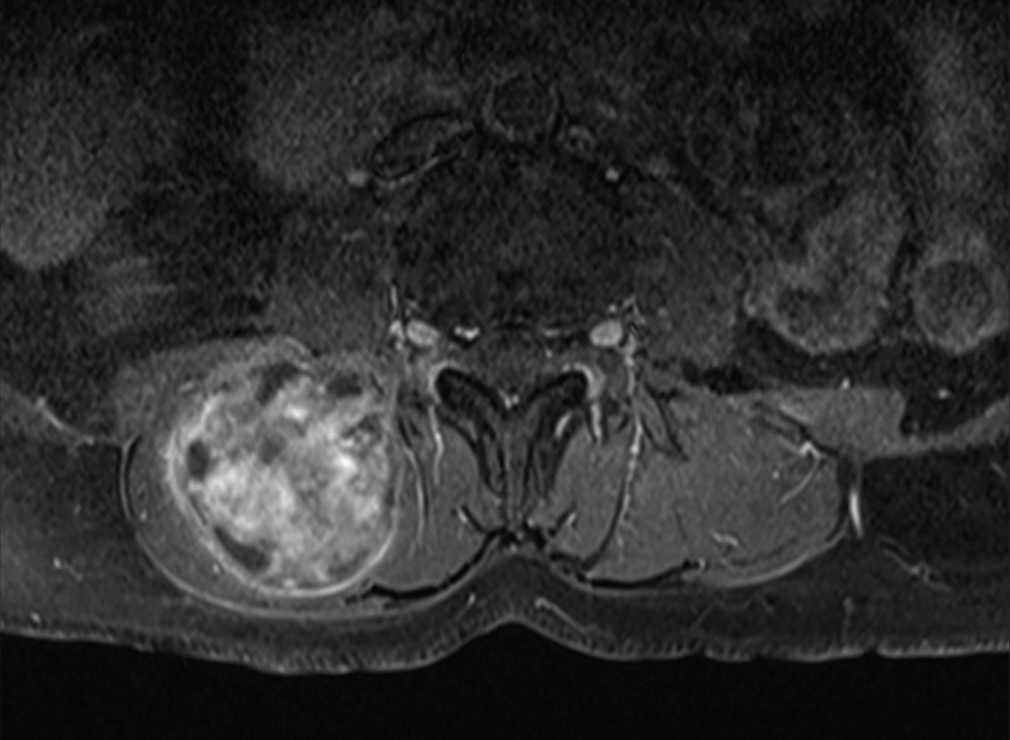
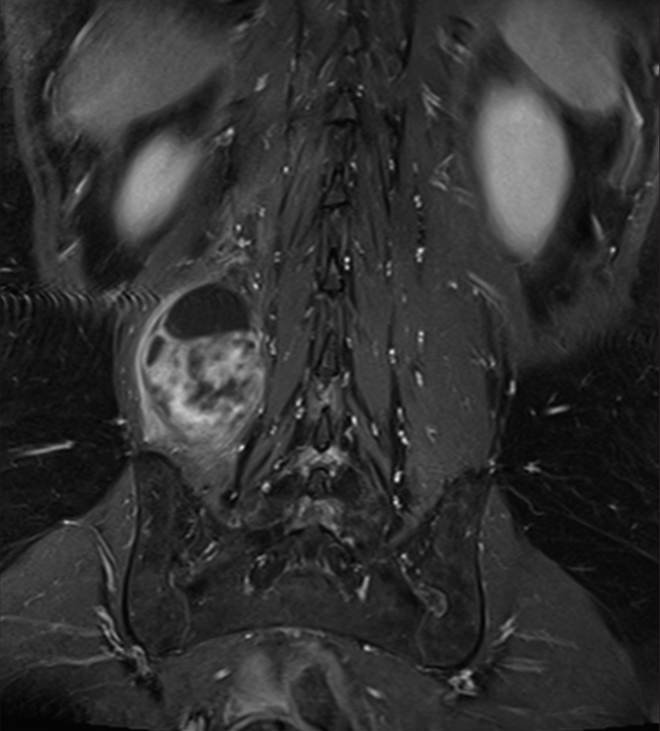
Case Description: A 64-year-old female presented with a protracted course of nocturnal lumbar pain that radiated to the anterior aspect of the right thigh accompanied by numbness. She reported a slow-growing right paramedian lumbar mass in the previous months. The magnetic resonance (MR) showed a right lumbar paravertebral intramuscular mass at the L3 level (i.e., 70 × 50 mm) that had well-defined margins, and markedly enhanced with gadolinium. Following gross total “en bloc” tumor resection, the patient fully recovered. Pathologically, the myofibroblastic lesion proved to be an intramuscular myxoma without malignant changes.
Conclusion: A 64-year-old female presented with a slow-growing MR-documented right paramedian lumbar L3 mass responsible for proximal right-thigh numbness. Following “en bloc” gross total removal of the benign intramuscular myxoma, the patient was asymptomatic.
Keywords: Intramuscular myxoma, Lumbar pain, Paraspinal tumors
INTRODUCTION
Intramuscular myxomas are a rare cause of low back pain that occur with a frequency of 1 in a million patients.[
CASE
Over the last few months, a 64-year-old female had noted a slow-growing right paramedian lumbar mass that was painful to deep palpation, but remained grossly mobile. She had accompanying persistent nocturnal lumbar pain with numbness in the anterior right thigh without any neurological deficits. The lumbar magnetic resonance (MR) showed an ovoid intramuscular L3 paravertebral right-sided mass (i.e. 70 × 50 mm longitudinal X anterior-posterior axes) that was hypointense on T1, and hyperintense on T2-weighted images; it had well-defined margins, and markedly enhanced with gadolinium (i.e., T1-weighted fat-suppression sequences) [

DISCUSSION
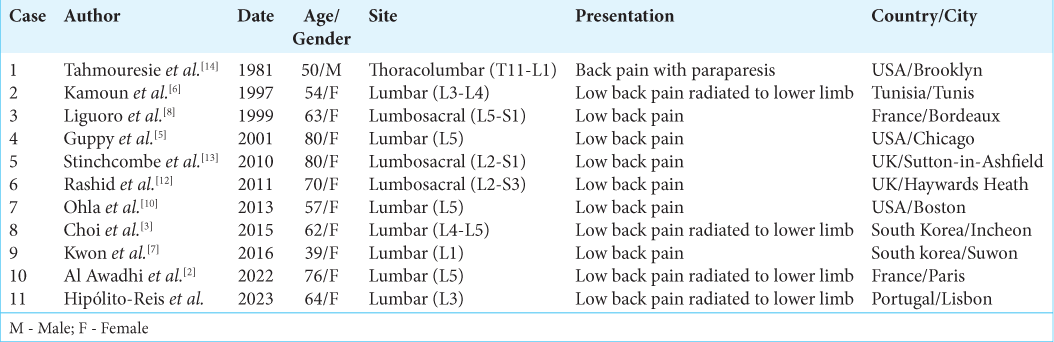
Intramuscular myxomas are rarely found in the lumbar paraspinal region.[
CONCLUSION
The most uncommon types of benign soft-tissue myxomas are found in the paraspinal musculature. Here, we presented a 64-year-old female who presented with a slow-growing right-sided L3 paraspinal intramuscular mass responsible for the right thigh pain/numbness that, once removed “en bloc,” resulted in complete symptom resolution.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Al Abdulsalam A, Al Safi S, Aldaoud S, Al-Shadidi N, Dhar PM. Intramuscular myxoma of the left thigh: A case report. Int J Surg Case Rep. 2022. 100: 107710
2. Al Awadhi A, Benichi S, Lot G, Rogers A. A case of intramuscular lumbar myxoma: Uncertainty in the preoperative diagnosis of a spinal soft tissue tumour. Neurochirurgie. 2022. 68: 530-4
3. Choi DY, Kim JT, Kim J, Lee HJ. Atypical Intramuscular myxoma of the lumbosacral paraspinal muscle: The first case report in Asian. J Korean Neurosurg Soc. 2015. 58: 566-70
4. Falavigna A, Righesso O, Volquind D, Teles AR. Intramuscular myxoma of the cervical paraspinal muscle. Eur Spine J. 2009. 18: 245-9
5. Guppy KH, Wagner F, Tawk R, Gallagher L. Intramuscular myxoma causing lumbar radiculopathy. Case report and review of the literature. J Neurosurg. 2001. 95: 260-3
6. Kamoun N, Zouari M, Siala M, Karray S, Douik M, Litaiem T. Intramuscular myxoma. Apropos of two cases. Rev Chir Orthop Reparatrice Appar Mot. 1997. 83: 278-82
7. Kwon JY, Kim IS, Hong JT, Kim JY, Sung JH, Lee SW. Intramuscular myxoma of the lumbar paravertebral muscle. Spine J. 2016. 16: e451-2
8. Liguoro D, Viejo-Fuertes D, Vital A, San Galli F, Dautheribes M, Guerin J. Intramuscular myxoma. A case of myxoma of the spinal erector muscle. Neurochirurgie. 1999. 45: 54-7
9. Miettinen M, Höckerstedt K, Reitamo J, Tötterman S. Intramuscular myxoma-a clinicopathological study of twenty-three cases. Am J Clin Pathol. 1985. 84: 265-72
10. Ohla V, Ciarlini PD, Goldsmith JD, Kasper EM. Cellular myxoma of the lumbar spine. Surg Neurol Int. 2013. 4: 82
11. Patel S, Suji T, Pang G, Alg VS, Visagan R, Reisz Z. Spinal myxomas: Review of a rare entity. J Surg Case Rep. 2022. 2022: rjac221
12. Rashid A, Abdul-Jabar HB, Karmani S, Rezajooi K, Casey AT. Giant paravertebral myxoma. Eur Spine J. 2011. 20: S138-42
13. Stinchcombe S, Kochhar R, Malkan D. Intramuscular myxoma of the paraspinal musculature. J Med Cases. 2010. 1: 42-6
14. Tahmouresie A, Farmer PM, Stokes N. Paraspinal myxoma with spinal cord compression. Case report. J Neurosurg. 1981. 54: 542-4


Dr Safi Ur Rehman
Posted March 15, 2023, 9:05 pm
what was the preoperative , provisonal diagnosis.
Being very rare and benign condition, this is a wonderful and pratical addition to the lierature.