

- Department of Neurosurgery, Louisiana State University of Health Sciences, Shreveport, Louisiana, USA
- Department of Aerospace Medicine, U.S. Navy Air Test and Evaluation Squadron Three Zero, Naval Air Station Point, Oxnard, CA, USA
Correspondence Address:
Richard P. Menger
Department of Neurosurgery, Louisiana State University of Health Sciences, Shreveport, Louisiana, USA
DOI:10.4103/2152-7806.163963
Copyright: © 2015 Menger RP. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Menger RP, Wolf ME, Kukreja S, Sin A, Nanda A. Medicare payment data for spine reimbursement; important but flawed data for evaluating utilization of resources. Surg Neurol Int 31-Aug-2015;6:
How to cite this URL: Menger RP, Wolf ME, Kukreja S, Sin A, Nanda A. Medicare payment data for spine reimbursement; important but flawed data for evaluating utilization of resources. Surg Neurol Int 31-Aug-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/medicare-payment-data-for-spine-reimbursement-important-but-flawed-data-for-evaluating-utilization-of-resources/
Abstract
Background:Medicare data showing physician-specific reimbursement for 2012 were recently made public in the mainstream media. Given the ongoing interest in containing healthcare costs, we analyze these data in the context of the delivery of spinal surgery.
Methods:Demographics of 206 leading surgeons were extracted including state, geographic area, residency training program, fellowship training, and academic affiliation. Using current procedural terminology (CPT) codes, information was evaluated regarding the number of lumbar laminectomies, lumbar fusions, add-on laminectomy levels, and anterior cervical fusions reimbursed by Medicare in 2012.
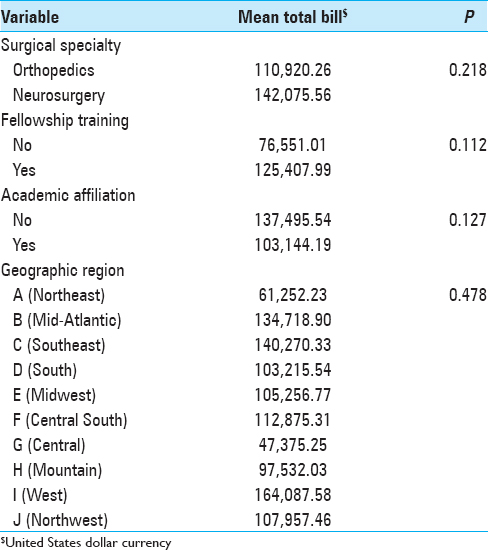
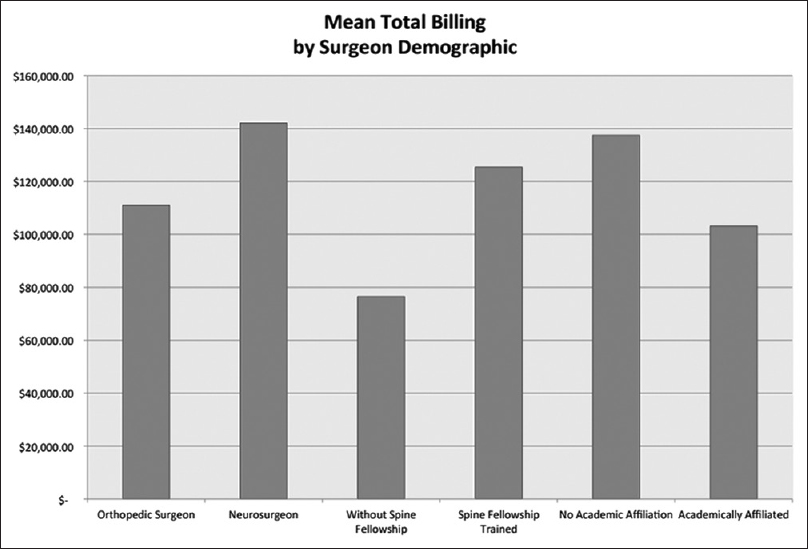
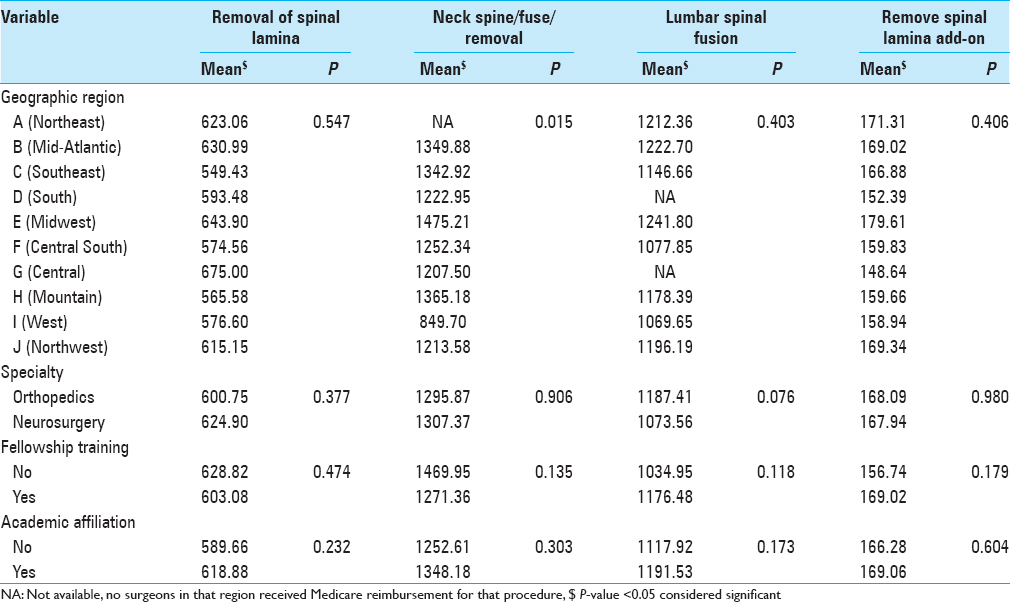
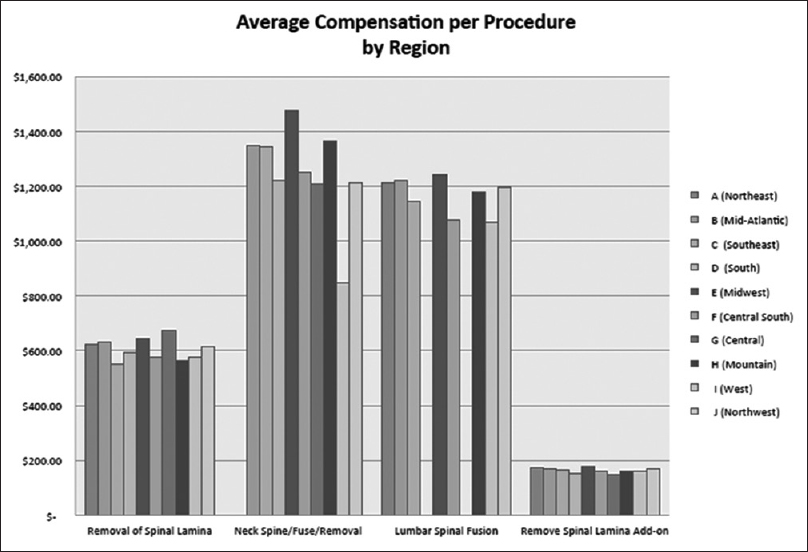
Results:In 2012 Medicare reimbursed the average neurosurgeon slightly more than an orthopedic surgeon for all procedures ($142,075 vs. $110,920), but this was not found to be statistically significant (P = 0.218). Orthopedic surgeons had a statistical trend illustrating increased reimbursement for lumbar fusions specifically, $1187 versus $1073 (P = 0.07). Fellowship trained spinal surgeons also, on average, received more from Medicare ($125,407 vs. $76,551), but again this was not statistically significant (P = 0.112). A surgeon in private practice, on average, was reimbursed $137,495 while their academic counterparts were reimbursed $103,144 (P = 0.127). Surgeons performing cervical fusions in the Centers for Disease Control West Region did receive statistically significantly less reimbursement for that procedure then those surgeons in other parts of the country (P = 0.015). Surgeons in the West were reimbursed on average $849 for CPT code 22,551 while those in the Midwest received $1475 per procedure.
Conclusion:Medicare reimbursement data are fundamentally flawed in determining healthcare expenditure as it shows a bias toward delivery of care in specific patient demographics. However, neurosurgeons, not just policy makers, must take ownership to analyze, investigate, and interpret these data as it will affect healthcare reimbursement and delivery moving forward.
Keywords: Healthcare economics, Medicare, reimbursement, spinal surgery
INTRODUCTION
Costs for healthcare delivery total $2.8 trillion, or about 18% of the US gross domestic product. The Affordable Care Act focuses on value in the medical arena.[
The dollar amount billed to Medicare physician was made public in 2012. Neurosurgeons must take ownership of the data regarding their perceived reimbursement. Medicare billing data show the physician-specific payments of 77 billion dollars across 880,000 medical providers.[
METHODS
Surgeons were enrolled into our analysis if they were listed in Becker's 2012 Spine Review “Spine Surgeons and Specialist to Know.”[
Spinal surgeons crossing the discipline of neurosurgery and orthopedic surgery were investigated for utilization of resources. Demographics of individual spine surgeons were extracted including state, geographic area, residency training program, fellowship training, and academic affiliation. Geographic area was split based on the Centers for Disease Control Prevention and Health Promotion map, carving the United States among 10 Department of Health and Human Services Regions.[
Residency program training information was retrieved from publically available information regarding surgeon biography. Fellowship training was considered only for the discipline of spinal surgery. No distinction was made between the type of spinal fellowship being orthopedic or neurosurgical. No distinction was made between the specific discipline of the fellowship; minimally invasive, scoliosis, degenerative, and spinal oncology were all considered. No distinction was made between “en-folded” neurosurgery fellowships and typical postresidency fellowships. Physicians were considered to have an academic affiliation if this information was listed in publically available information regarding the physician. There was no distinction made between academic title (e.g., Professor vs. Clinical Instructor). It was not possible, given the data, to separate between the physical location of surgery (e.g., community hospital, academic hospital, or surgery center).
No human subjects or patient specific information was used from this publically available data set thereby not requiring Internal Review Board approval.
Database
Medicare data were extracted from the Wall Street Journal search page for “Medicare Payments to Providers in 2012.”[
Information was also extracted regarding the number of lumbar laminectomies, the addition of another laminectomy level, lumbar fusions, and anterior cervical fusions performed by each surgeon. The average dollar amount for each surgery was calculated. The 2012 data described procedures per Medicare are based on current procedural terminology (CPT) codes.[
Statistical analysis
Appropriate descriptive statistics were obtained. Comparison between total utilization of resources as well as mean reimbursement per procedure type was obtained. Mean total or average payments among the two groups were compared using the independent t-test. ANOVA test was performed if such association was made between more than 2 groups. P < 0.05 was considered to have statistical significance. Analyses were performed using the SPSS software (v21, IBM Inc., IL, USA).
RESULTS
Descriptive findings
Two hundred and six physicians were reviewed for utilization of resources during the 2012 Medicare reimbursement period. Descriptive data are located in
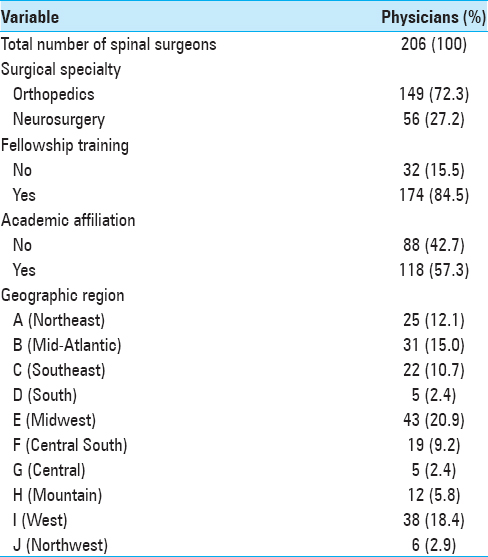
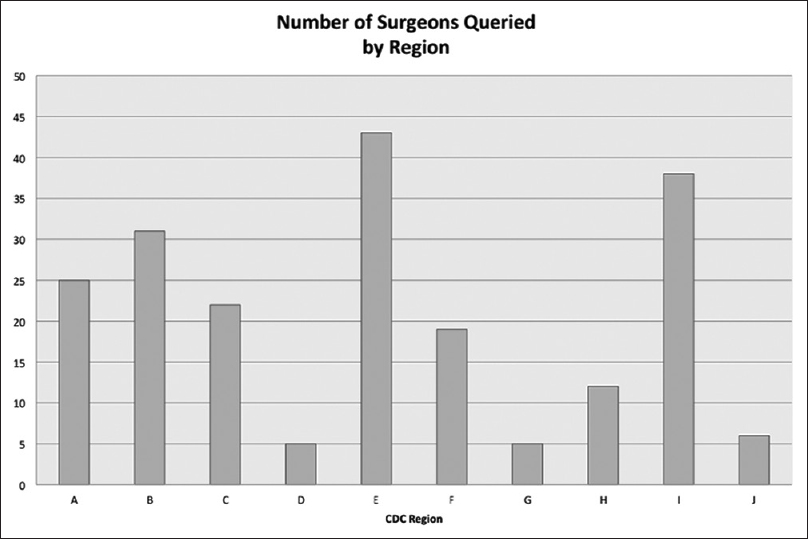
Geographically, Becker's List favored the major cities. Breakdown of geographic representation can be seen in
Total reimbursement
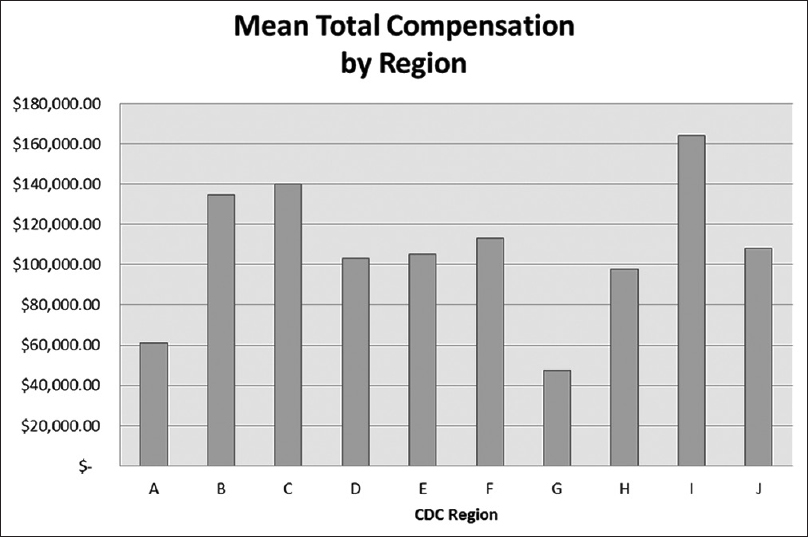
The comparisons of the total amount received from Medicare in 2012 per surgeon for all procedures are found in
Procedural reimbursement
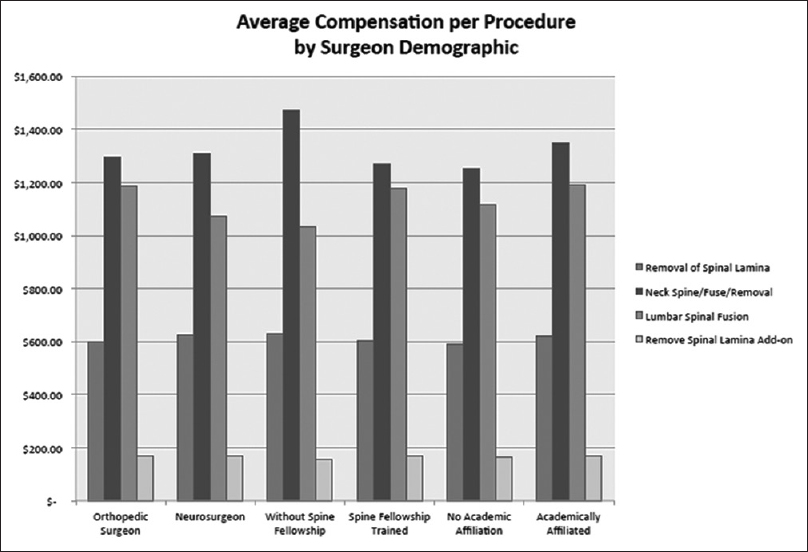
Comparison of per procedure reimbursement for common spinal operations is found in
Orthopedic surgeons had a statistical trend illustrating increased reimbursement for lumbar fusions compared to their neurosurgeon counterparts, $1187 versus $1073 (P = 0.07). Orthopedic and neurosurgeons received similar compensation across different procedure types: $600 versus $624 for lumbar laminectomy (P = 0.377), $1295 versus $1307 for cervical fusion (P = 0.9), and add-on level of laminectomy $168 versus $167. Fellowship training and academic affiliation did not illustrate any statistically significant difference between the amount of reimbursement per procedure type. Data affecting surgeon specific procedural reimbursement are represented in
DISCUSSION
Medicare data provide a snapshot of one fraction of total healthcare spending, representing only 21% of a total $2.8 trillion national healthcare expenditure in 2012.[
Orthopedic/neurosurgery comparison
In our study, orthopedic surgeons saw increased reimbursement for lumbar spinal fusions compared to their neurosurgeon counterparts, but these data may further represent a number of influences. In the future, continued emphasis will be placed on lumbar fusions given that Medicare's rate of spending for spinal surgery has doubled in the past decade.[
In 2014, Mroz et al. compared different approaches to single and recurrent lumbar disc herniations. According to Mroz, orthopedic and neurosurgeons did not show a statistically significant difference in selection of revision microdiscectomy, revision microdiscectomy with posterolateral fusion using pedicle screws, revision microdiscectomy with posterior lumbar interbody fusion/transforaminal lumbar interbody fusion, or anterior lumbar interbody fusion for management of this pathology. Furthermore, Mroz found no statistically significant difference based on region, fellowship training, or practice type; they did, however, find that more senior surgeons (which were defined as a surgeon practicing >15 years) were more likely to offer revision discectomy without supplemental fusion.[
Regional variation
Regional variations do exist in the application of healthcare that extends beyond simple reimbursement to the physician. Bederman et al., in 2011, noted significant regional variation in spine surgery. In Bederman's study, counties with higher rates of surgery had, among other factors, demographic differences in the patient population (older male patients and lower income) and the increased presence of magnetic resonance imaging scanners as compared to counties with lower surgical rates.[
The American Board of Orthopedic Surgeons (AAOS) reports the overall prevalence of cervical fusion procedures has increased 41% from 1999 to 2008, while anterior cervical plating increased between 1999 and 2008 from 39% to 79% of cases performed. Meanwhile, the use of allograft also skyrocketed from 14% to 59% in this time period as well. Cervical fusion as a procedure did show some regional preferences within AAOS data with the Southwest being most likely to use interbody devices while the Midwest region was more likely to use allograft. The Southeast was also more likely to use anterior cervical plating then the Midwest region demonstrated.[
The US government does make Medicare program data available to the public through the Centers for Medicare and Medicaid Services, and information available does show regional differences in per capita Medicare spending. Gottlieb, et al., in 2010, demonstrated that the regions containing New York and Florida utilize more resources and require greater spending than is compensated by increased costs of goods and services within those regions or account for localized inflation. From 1992 to 2006, for example, Miami boasted a 5.0% per capita inflation adjusted yearly spending increase as compared to 2.3% in Salem, Oregon,[
Physician data
Furthermore, focused analysis of healthcare spending upon the utilization of physician resources presents a warped picture of the problems facing healthcare in the United States. Physician services account for approximately 20% of healthcare billing in the US and even then, there is a great divergence of reimbursement between different medical and surgical specialties.[
Limitations
Our data have a number of limitations in application. The list of spinal surgeons used is intended to sample leadership in the field of spine surgery as viewed by the public. Becker's list is a socioeconomic publication, and it heavily favored orthopedic surgeons (70.9% of those listed). A significant limitation to this data analysis is that, in querying only the Medicare data, it specifically excludes all other payer sources. This disproportionally illustrates higher spending by surgeons performing operations for degenerative conditions and serving in those areas with lower socioeconomic indicators or more elderly populations. Medicare data largely ignore pediatric population, and reimbursements by experts within this field are minimally represented within our results since they did not perform common spinal procedures billed to Medicare.
CONCLUSION
Regardless of the data's shortcomings, these are the data the public is seeing, Congress is politicizing, and lawyers are analyzing. Neurosurgeons must appreciate these data in the context of spinal surgery. Neurosurgeons, not just public policy makers, must take ownership to analyze, investigate, and interpret these data as it will affect policy moving forward.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in the study or the findings specified in this paper. The views expressed in this study are the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the US Government.
References
1. Last accessed on 2014 Apr 18. Available from: http://www.beckersspine.com/lists/item/11019-200-spine-surgeons-specialists-to-know.
2. Allain JM, Lurie J, Olson P, Bronner K, Fisher E. United States’ trends and regional variations in lumbar spine surgery: 1992-2003. Spine. 2006. 1: 2707-14
3. Bederman SS, Coyte PC, Kreder HJ, Mahomed NN, McIsaac WJ, Wright JG. Who's in the driver's seat? The influence of patient and physician enthusiasm on regional variation in degenerative lumbar spinal surgery: A population-based study. Spine (Phila Pa 1976). 2011. 36: 481-9
4. Last accessed on 2014 Apr 18. Available from: https://www.mail-attachment.googleusercontent.com/attachment/u/0/?ui=2 and ik=8f9a077fe4 and view=att and th=14563795dd122790 and attid=0.1 and disp=safe and realattid=file2 and zw and saduie=AG9B_P8vWwgtRyW_YRvJFvE09b9P and sadet=1397849354992 and sads=gm_HNUvwisn4_YsDOWuhap_tnOY.
5. Cohen JT, Neumann PJ, Weinstein MC. Does preventive care save money? Health economics and the presidential candidates. N Engl J Med. 2008. 358: 661-3
6. Cook C, Santos GC, Lima R, Pietrobon R, Jacobs DO, Richardson W. Geographic variation in lumbar fusion for degenerative disorders: 1990 to 2000. Spine J. 2007. 7: 552-7
7. Last accessed on 2014 Apr 18. Available from: http://www.washingtonpost.com/business/economy/data-uncover-nations-top-medicare -billers/2014/04/08/9101a77e-bf39-11e3-b574-f8748871856a_story.html.
8. Gottlieb DJ, Zhou W, Song Y, Andrews KG, Skinner JS, Sutherland JM. Prices don’t drive regional medicare spending variations. Health Aff (Millwood). 2010. 29: 537-43
9. Lad SP, Babu R, Baker AA, Ugiliweneza B, Kong M, Bagley CA. Complications, reoperation rates, and health-care cost following surgical treatment of lumbar spondylolisthesis. J Bone Joint Surg Am. 2013. p. 95-e162
10. McCarthy IM, Hostin RA, Ames CP, Kim HJ, Smith JS, Boachie-Adjei O. Total hospital costs of surgical treatment for adult spinal deformity: An extended follow-up study. Spine J. 2014. 14: 2326-33
11. McGuire KJ, Harrast J, Herkowitz H, Weinstein JN. Geographic variation in the surgical treatment of degenerative cervical disc disease: American Board of Orthopedic Surgery (ABOS) quality improvement initiative; part II candidates. Spine. 2012. 37: 57-66
12. Medicare CLast accessed on 2014 Jul 04. Available from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Research/ResearchGenInfo/CMSStatistics.html.
13. Medicare CLast accessed on 2014 Apr 18. Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Physician-and-Other-Supplier.html.
14. Last accessed on 2015 Mar 01. Available from: http://graphics.wsj.com/medicare-billing/.
15. Mroz TE, Lubelski D, Williams SK, O'Rourke C, Obuchowski NA, Wang JC. Differences in the surgical treatment of recurrent lumbar disc herniation among spine surgeons in the United States. Spine J. 2014. 14: 2334-43
16. Patel KK, Nadel J. Improving the quality and lowering the cost of health care: Medicare reforms from the National Commission on Physician Payment Reform. J Gen Intern Med. 2014. 29: 703-4
17. Last accessed on 2014 Apr 18. Available from: http://www.online.wsj.com/news/articles/SB10001424052702303456104579490043350808268.
18. Ugiliweneza B, Kong M, Nosova K, Huang KT, Babu R, Lad SP. Spinal surgery: Variations in health care costs and implications for episode-based bundled payments. Spine (Phila Pa 1976). 2014. 39: 1235-42
19. Last accessed on 2014 May 23. Available from: http://www.bloomberg.com/infographics/2014-04-09/which-medical-specialties-cost-medicare-the-most.html.
20. Whoriskey PLast accessed on 2015 Mar 01. Available from: http://wwww.washingtonpost.com/business/economy/spinal-fusions-serve-as-case-study-for-debate-over-when-certain-surgeries-are-necessary/2013/10/27/5f015efa-25ff-11e3-b3e9-d97fb087acd6_story.html.

