

- Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India.
- Department of Spine Surgery, Apollo Hospital, Guwahati, Assam, India.
Correspondence Address:
Nitin Adsul, Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India.
DOI:10.25259/SNI_417_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shankar Acharya1, Manoj Kumar1, Jay Deep Ghosh2, Nitin Adsul1, R. S. Chahal1, K. L. Kalra1. Morphometric parameters of the odontoid process of C2 vertebrae, in Indian population, a CT evaluation. 30-Sep-2021;12:494
How to cite this URL: Shankar Acharya1, Manoj Kumar1, Jay Deep Ghosh2, Nitin Adsul1, R. S. Chahal1, K. L. Kalra1. Morphometric parameters of the odontoid process of C2 vertebrae, in Indian population, a CT evaluation. 30-Sep-2021;12:494. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11133
Date of Submission
26-Apr-2021
Date of Acceptance
30-Aug-2021
Date of Web Publication
30-Sep-2021
Abstract
Background: Osteosynthesis of odontoid fractures, especially for type II odontoid fractures, is often achieved by the placement of screws. Here, utilizing CT, we evaluated the normal anatomy of the odontoid process in an Indian population to determine whether one or two screws could be anatomically accommodated to achieve fixation.
Methods: CT-based morphometric parameters of the odontoid process were assessed in 200 normal Indian patients (2018–2020).
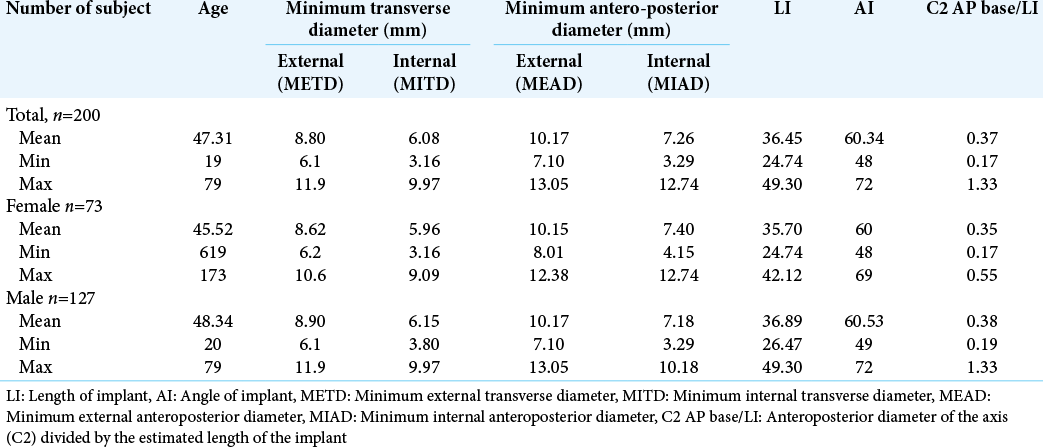
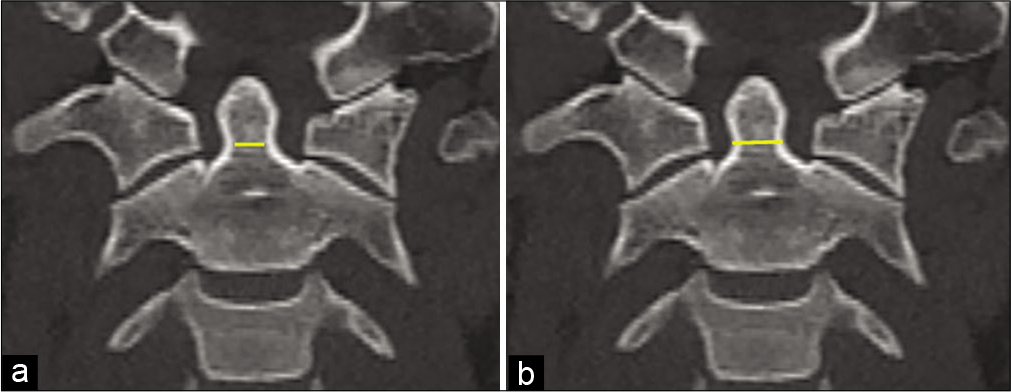
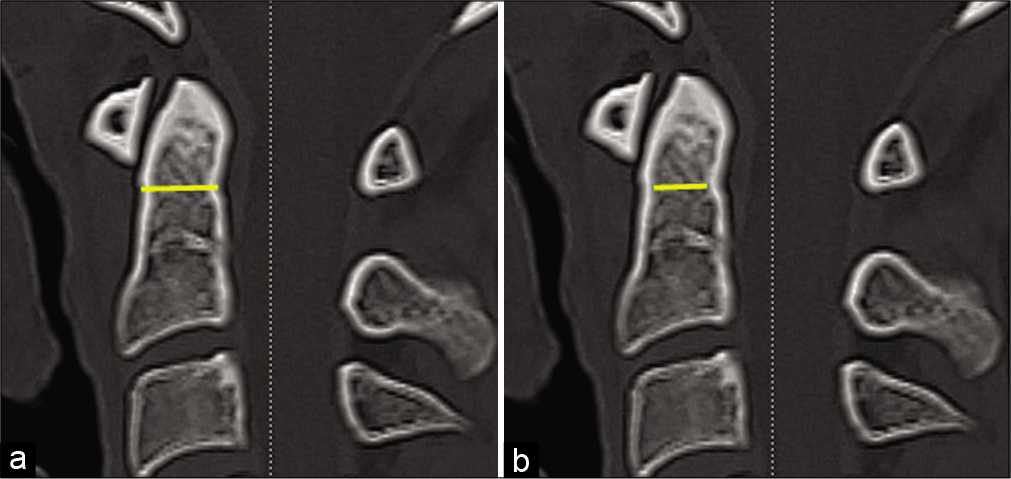
Results: Of 200 patients, 127 were male, and 73 were female. The mean minimum external transverse diameter (METD) was 8.80 mm (range 6.1–11.9 mm). Six (3%) patients had a minimum internal transverse diameter (TD) of >8.0 mm that would allow for the insertion of two 3.5-mm cortical screws without tapping, while 10 (5%) patients had TDs of
Conclusion: About two-thirds (59%) of the 200 subjects in our study had a METD of
Keywords: Indian odontoid, Normal morphometric dimensions, Screw fixation of odontoid
INTRODUCTION
The accurate radiological evaluation and assessment of the morphometric parameters of the odontoid are critical in achieving stable fixation and fusion of odontoid fractures.[
MATERIALS AND METHODS
This is a retrospective analysis of the CT studies of the odontoid process performed in 200 asymptomatic adults (2018–2020). The measurements were performed by a single observer.
The CT scans were randomly collected from our hospital radiology archives along with relevant variables; there were multiple inclusion and exclusion criteria [
Statistical analysis
Statistical comparisons between variables within gender were tested using the Student’s t-test after verifying that the distribution of the variables was normal (P < 0.05 is significant). The Fisher’s exact test was used to examine the significance of the association between sex and minimum external transverse diameter (METD) smaller than 9 mm (Statistical Package for Social Sciences – Version 11.0).
RESULTS
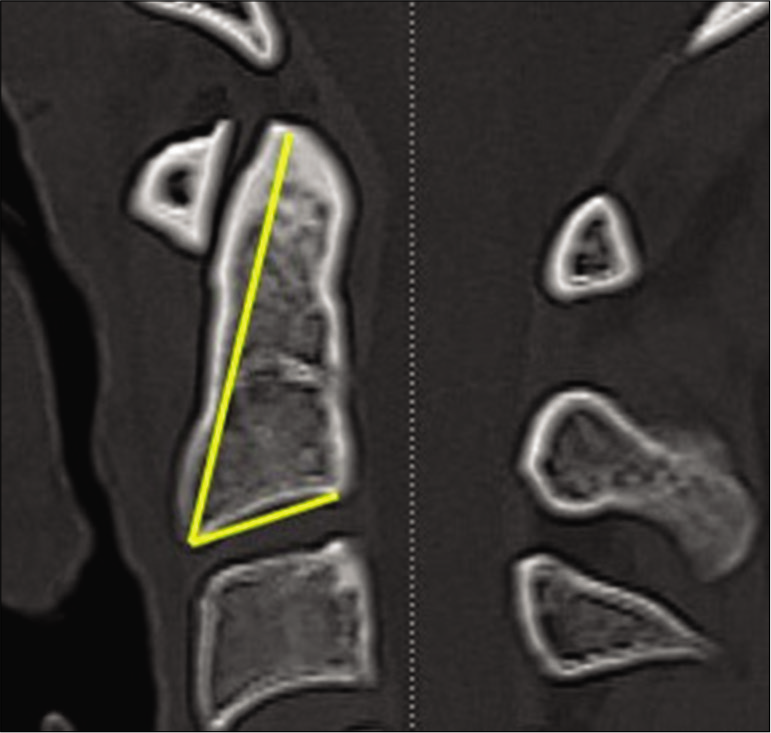
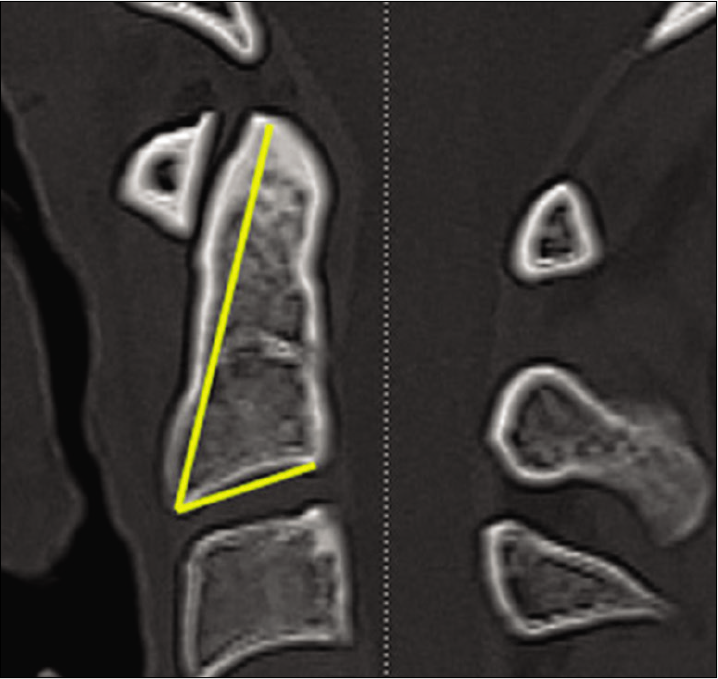
There were 200 CT studies of odontoid processes. Ten (5%) patients had transverse diameter (TD) <7.4 mm, while none of the patients had diameters of <5.5 mm. The mean minimal external antero-posterior (AP) diameter of the entire population was 10.17 mm (range 7.10– 13.05 mm, SD 1.09 mm), while the mean length of the implant was 36.45 mm. The mean angle of screw insertion was 60.34° [
DISCUSSION
In this study, we evaluated the morphology of the odontoid process using an accurate and reliable CT-based measurement method. The external CT measurements correlated well with calliper-derived data.[
Several studies evaluated the size of the odontoid process
Kulkarni et al.,[

Angle of screw insertion
The mean angle of screw insertion was 60.34° (60° on average in females and 60.53° average in males). In Tun et al.,[
Pros for 2 screw fixation
There are considerably higher rates of union with dual screw osteosynthesis.[
Pros for single Herbert screw placement
For TD measurements of the dens <5.5 mm, only a single 4.5 mm Herbert screw can be safely used. Notably, Lee and Sung reported a good union rate and no implant failures using single 4.5 mm Herbert screws.[
Use of CT to calculate appropriate screw length and diameter
CT reconstructed images make it possible to calculate the diameter and length of the odontoid process and to estimate the quality of bone and size of the odontoid for the safety/ efficacy of anticipated one to two screw fixation.
CONCLUSION
About two-thirds (59%) of the subject in our Indian population had a METD of the odontoid process of <9 mm. This meant that only one screw could be safely placed in an odontoid process for these individuals.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chadha M, Balain B, Maini L, Dhaon B. Pedicle morphology of the lower thoracic, lumbar, and S1 vertebrae: An Indian perspective. Spine (Phila Pa 1976). 2003. 28: 744-9
2. Daher MT, Daher S, Defino HL. Tomographic evaluation of odontoid parameters related to its internal fixation. Coluna Columna. 2010. 9: 322-7
3. Dailey AT, Hart D, Finn MA, Schmidt MH, Apfelbaum RI. Anterior fixation of odontoid fractures in an elderly population. J Neurosurg Spine. 2010. 12: 1-8
4. Heller J, Alson M, Schaffler M, Garfin S. Quantitative internal dens morphology. Spine (Phila Pa 1976). 1992. 17: 861-6
5. Kulkarni AG, Shah SM, Marwah RA, Hanagandi PB, Talwar IR. CT based evaluation of odontoid morphology in the Indian population. Indian J Orthop. 2013. 47: 250-4
6. Laurer H, Sander A, Maier B, Marzi I. Fractures of the cervical spine. The orthopedist. 2010. 39: 237-46
7. Lee SH, Sung JK. Anterior odontoid fixation using a 4.5-mm Herbert screw: The first report of 20 consecutive cases with odontoid fracture. Surg Neurol. 2006. 66: 361-6
8. Nourbakhsh A, Patil S, Vannemreddy P, Ogden A, Mukherjee D, Nanda A. The use of bioabsorbable screws to fix Type II odontoid fractures: A biomechanical study. J Neurosurg Spine. 2011. 15: 361-6
9. Nucci RC, Seigal S, Merola AA, Gorup J, Mroczek KJ, Dryer J. Computed tomographic evaluation of the normal adult odontoid: Implications for internal fixation. Spine (Phila Pa 1976). 1995. 20: 264-70
10. Puchwein P, Jester B, Freytag B, Tanzer K, Maizen C, Gumpert R. The three-dimensional morphometry of the odontoid peg and its impact on ventral screw osteosynthesis. Bone Joint J. 2013. 95: 536-42
11. Tun K, Kaptanoglu E, Cemil B, Yorubulut M, Karahan ST, Tekdemir I. Anatomical study of axis for odontoid screw thickness, length, and angle. Eur Spine J. 2009. 18: 271-5
12. Yusof M, Yusof A, Abdullah M, Hussin T. Computed tomographic evaluation of the odontoid process for two-screw fixation in Type-II fracture: A Malaysian perspective. J Orthop Surg. 2007. 15: 67-72

