

- Department of Carle Illinois College of Medicine, University of Illinois Urbana-Champaign, Urbana, Illinois, United States,
- Department of Pathology and Laboratory Medicine, Carle Foundation Hospital, Urbana, Illinois, United States,
- Department of Bioengineering, University of Illinois Urbana-Champaign, Urbana, Illinois, United States,
- Department of Neurosurgery, Carle Foundation Hospital, Urbana, Illinois, United States.
Correspondence Address:
Paul M. Arnold, Department of Neurosurgery, Carle Foundation Hospital, Urbana, Illinois, United States.
DOI:10.25259/SNI_1167_2022
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Tarika Deepak Patel1, Ikechukwu Uzoaru2, Bradley P. Sutton3, Paul M. Arnold4. Myeloid sarcoma of the thoracic spine: A case report. 27-Jan-2023;14:35
How to cite this URL: Tarika Deepak Patel1, Ikechukwu Uzoaru2, Bradley P. Sutton3, Paul M. Arnold4. Myeloid sarcoma of the thoracic spine: A case report. 27-Jan-2023;14:35. Available from: https://surgicalneurologyint.com/surgicalint-articles/12121/
Date of Submission
29-Dec-2022
Date of Acceptance
18-Jan-2023
Date of Web Publication
27-Jan-2023
Abstract
Background: Myeloid sarcoma is an uncommon malignant neoplasm that typically arises at extramedullary sites and is associated with a diagnosis of acute myeloid leukemia. While myeloid sarcoma can involve any organ, central nervous system involvement is rare, particularly in the adult population.
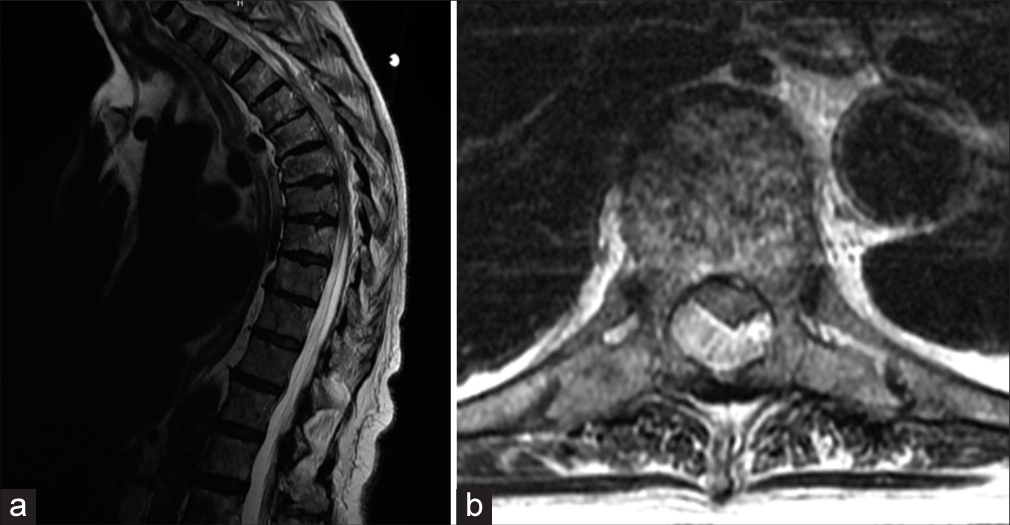
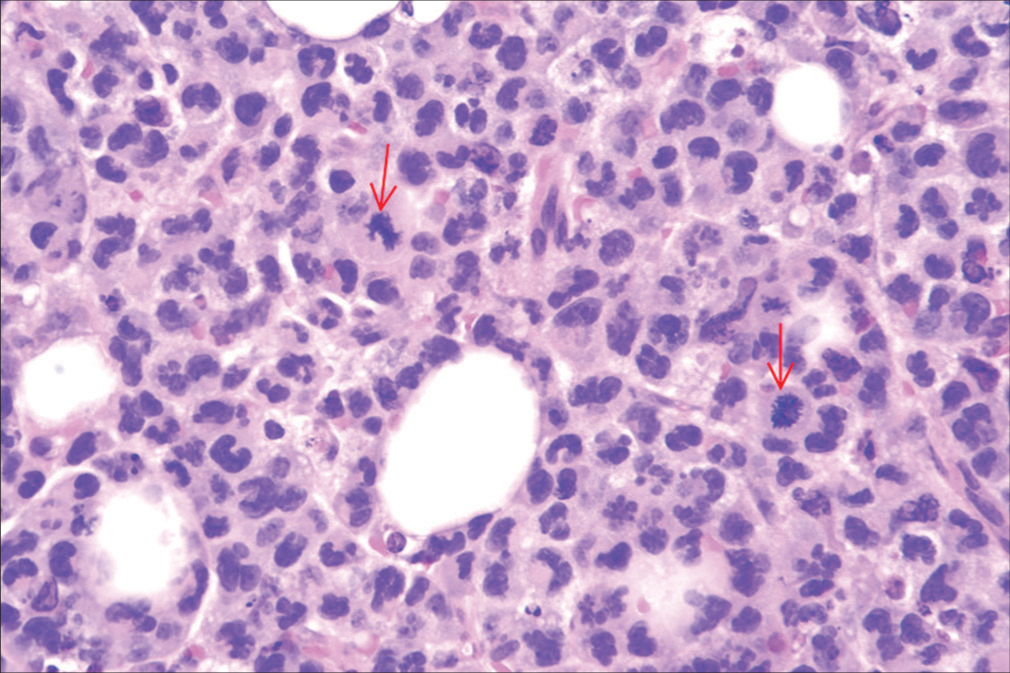
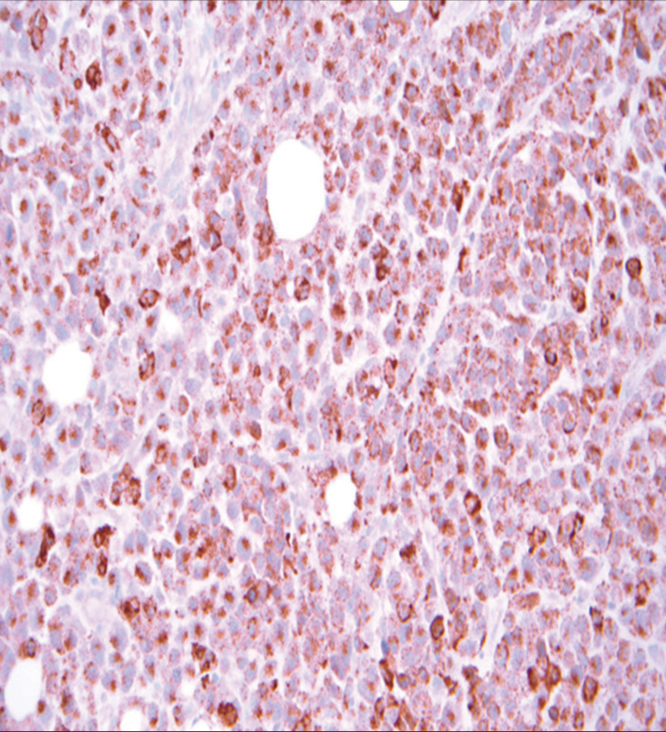
Case Description: An 87-year-old female presented with progressive paraparesis of 5 days’ duration. The magnetic resonance imaging (MRI) revealed an epidural tumor from T4 to T7 with cord compression. When she underwent a laminectomy for tumor resection, the pathology revealed a myeloid sarcoma with monocytic differentiation. Although she improved postoperatively, she elected to pursue hospice care and expired 4 months later.
Conclusion: Myeloid sarcoma is an uncommon malignant spinal neoplasm rarely seen in adults. For this 87-year-old female, MRI-documented cord compression warranted decompressive surgery. Although this patient did not opt for adjuvant therapy, other patients with such lesions may undergo additional chemotherapy or radiation therapy. Nevertheless, optimal management for such malignant tumor is still undefined.
Keywords: Chloroma, Cord compression, Granulocytic sarcoma, Myeloid sarcoma
INTRODUCTION
Myeloid sarcoma, also known as “granulocytic sarcoma” and “chloroma,” is a malignant neoplasm of hematopoietic origin that arises at extramedullary sites.[
CASE REPORT
An 87-year-old female presented with progressive paraparesis (i.e., left leg 3/5 and right leg 2/5) of 5 days’ duration. The patient was started on Rocephin for a urinary tract infection, but computed tomography angiogram of the head and neck and magnetic resonance imaging of the thoracic spine showed extensive bony metastatic disease with an epidural tumor at T4–T7 with severe cord compression [
DISCUSSION
Myeloid sarcoma is an uncommon, extramedullary neoplasm derived from malignant myeloid cell precursors.[
CONCLUSION
Myeloid sarcoma rarely presents in the extra-axial spine and although the optimal management for these lesions is not well-defined, surgical excision followed by chemotherapy or radiotherapy would most likely be considered.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Bai CR, Li X, Wang JS, Li JJ, Liu N, Fei Q. Diagnosis and surgical treatment of primary isolated aggressive lumbar myeloid sarcoma: A rare case report and review of the literatures. BMC Musculoskelet Disord. 2021. 22: 220
2. Bhandohal JS, Moosavi L, Garcia-Pacheco I, Yakoub G, Polineni RD, Cobos E. Isolated myeloid sarcoma of lumbar spine without bone marrow involvement: A rare case report and treatment dilemma. AME Case Rep. 2021. 5: 27
3. Chamberlain MC, Tredway TL, Born D, Fink J. Teaching NeuroImages: Sacral spine chloroma. Neurology. 2013. 81: e87
4. Joseph JR, Wilkinson DA, Bailey NG, Lieberman AP, Tsien CI, Orringer DA. Aggressive myeloid sarcoma causing recurrent spinal cord compression. World Neurosurg. 2015. 84: 866.e7-10
5. Lama S, Lui S, Xiao Y, Zhang H, Karki M, Gong Q. Sacral myeloid sarcoma involving multiple metastases to the brain: A case report. Exp Ther Med. 2015. 9: 1429-32
6. Landis DM, Aboulafia DM. Granulocytic sarcoma: An unusual complication of aleukemic myeloid leukemia causing spinal cord compression. A case report and literature review. Leuk Lymphoma. 2003. 44: 1753-60
7. Olar A, Lapadat R, Davidson CJ, Stein TD, Dahiya S, Perry A. Central nervous system involvement by myeloid sarcoma: A report of 12 cases and review of the literature. Clin Neuropathol. 2016. 35: 314-25
8. Shah K, Panchal H, Patel A. Spine myeloid sarcoma: A case series with review of literature. South Asian J Cancer. 2021. 10: 251-4
9. Slouma M, Rahmouni S, Dhahri R, Khayati Y, Zriba S, Amorri W. Epidural myeloid sarcoma as the presenting symptom of chronic myeloid leukemia blast crisis. Clin Rheumatol. 2020. 39: 2453-9
10. Smith TR, Slimack N, McClendon J, Wong A, Fessler RG. Low back pain and lumbar radiculopathy as harbingers of acute myeloid leukemia recurrence in a patient with myeloid sarcoma. J Clin Neurosci. 2012. 19: 1040-1

