

- Student Research Committe, Mashhad University of Medical Sciences, Mashhad, Iran,
- Department of Neurosurgery, Razavi Hospital, Mashhad, Iran,
- Department of Radiology, Mashhad University of Medical Sciences, Mashhad, Iran.
Correspondence Address:
Sajjad Saghebdoust, MD, MBA, Department of Neurosurgery, Razavi Hospital, Mashhad, Iran.
DOI:10.25259/SNI_1178_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohammad Moein Vakilzadeh1, Sajjad Saghebdoust2, Bita Abbasi3, Reza Zare2. Neglected alkaptonuric patient presented with low back pain and radiculopathy: A case report. 12-Jan-2022;13:15
How to cite this URL: Mohammad Moein Vakilzadeh1, Sajjad Saghebdoust2, Bita Abbasi3, Reza Zare2. Neglected alkaptonuric patient presented with low back pain and radiculopathy: A case report. 12-Jan-2022;13:15. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11337
Date of Submission
26-Nov-2021
Date of Acceptance
29-Dec-2021
Date of Web Publication
12-Jan-2022
Abstract
Background: Alkaptonuria (AKU) is a rare hereditary disorder in which excess homogentisic acid (HGA) deposits in connective tissues (ochronosis). Here, we report the unusual presentation of a lumbar disc herniation occurring in a patient with AKU warranting surgical intervention.
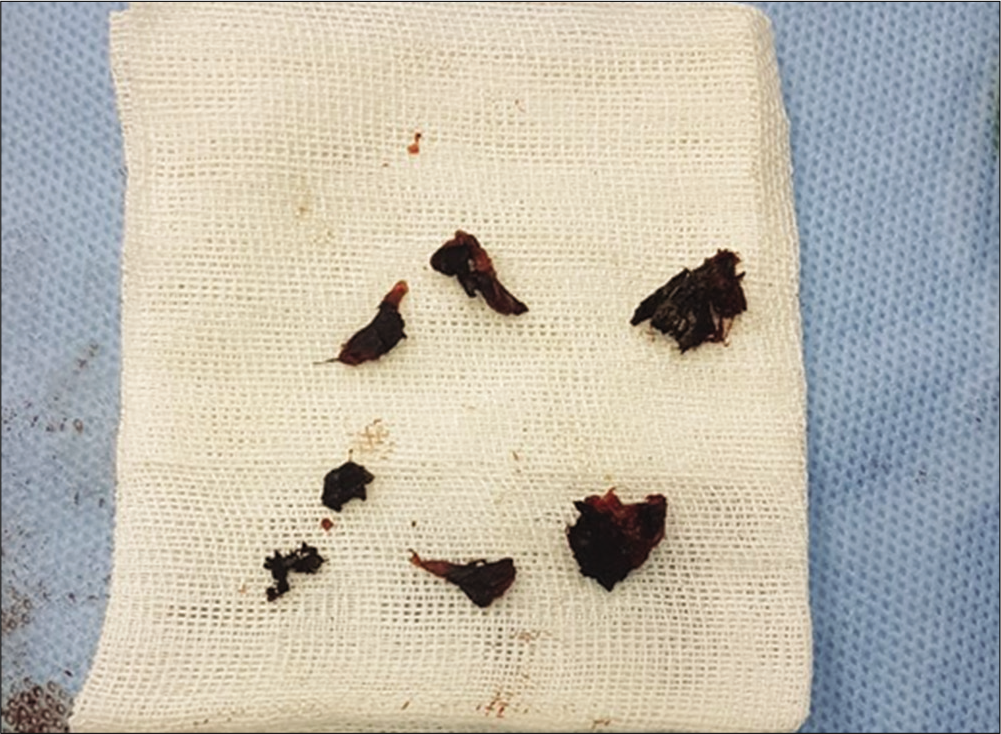
Case Description: A 28-year-old male presented with 1 year of low back pain. The lumbar magnetic resonance imaging showed an extruded disc at the L4-L5 level accompanied extensive disc space narrowing and osteophyte formation. At surgery, the interspinous ligaments, facet joints, and disc herniation were black. In addition, the postoperative re-examination revealed a black discoloration of the nasal and ear cartilage. Finally, the diagnosis of AKU was confirmed when the urine specimen was positive for HGA.
Conclusion: Rarely, younger patients with AKU who develop excess black deposits of HGA in connective tissues (i.e., ochronosis) may present with lumbar disc herniations and spondylosis.
Keywords: Alkaptonuria, Disc herniation, Low back pain, Radiculopathy
INTRODUCTION
Alkaptonuria (AKU) is a rare autosomal recessive inheritance disorder attributed to dysfunction of the third enzyme in tyrosine degradation (i.e., homogentisic acid [HGA] dioxygenase).[
CASE REPORT
A 28-year-old-male presented with 1 year of low back pain and a left foot drop (3/5 level). The lumbar magnetic resonance (MR) imaging revealed a disk extrusion at the L4-L5 level, disk space narrowing, and osteophyte formation out of proportion to the patient’s young age [
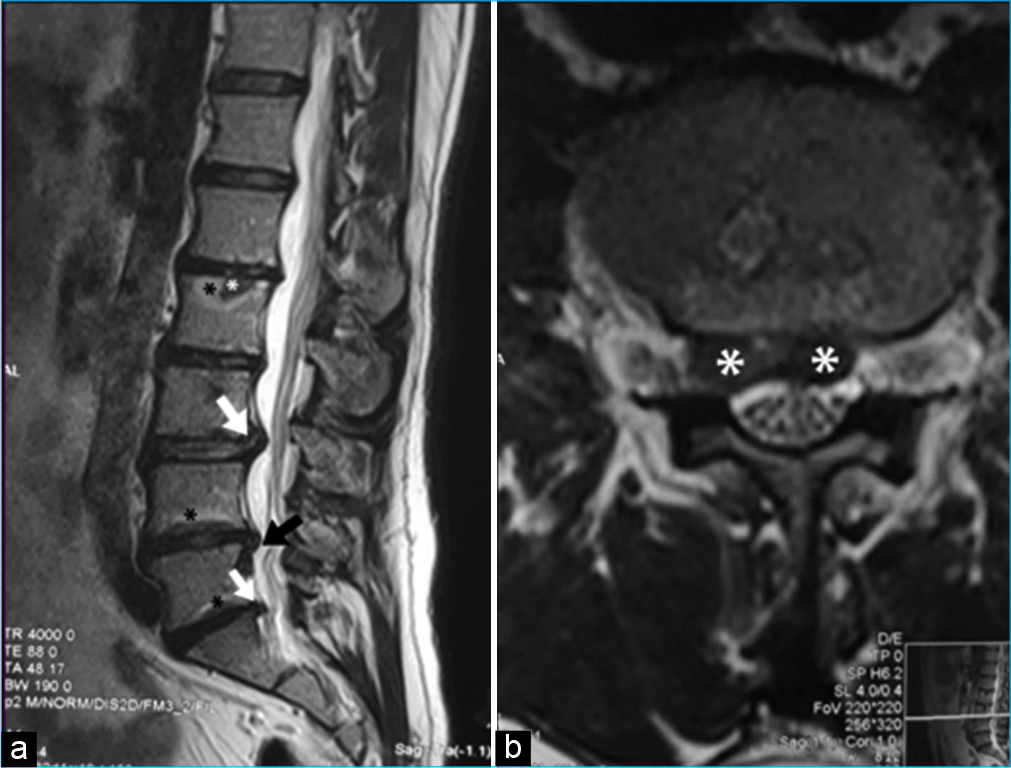
Figure 1:
Lumbar magnetic resonance imaging images in a 28-year-old patient in the sagittal (a) and axial (b) planes show disk protrusions (white arrows), disk extrusion (black arrow in a and asterisk in b), Schmorl’s node (white asterisk in a), and Modic degenerative changes at vertebral end plates (black asterisks in a).

DISCUSSION
AKU is a hereditary autosomal recessive metabolic disorder that occurs due to the failure to metabolize HGA (i.e., HGA oxidase deficiency). The excess of HGA is excreted in the urine, sweat, and deposits in the tissues; this is responsible for the formation of gray pigmentation termed ochronosis.[
Radiographic findings of AKU
Plain X-ray, computed tomography, and MR scans of the spine (i.e., especially the lumbar spine) typically document osteoporosis, calcification of the interspinous ligament, decreased disk space height, and disk calcification.[
Surgery for AKU
The diagnosis of AKU, although rare, is usually confirmed during discectomy as the ligaments, facet joints, and disc are typically black.[
CONCLUSION
Early diagnosis of patients with AKU may reveal a black discoloration involving multiple tissues.[
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
References
1. Choudhury R, Rajamani S, Rajshekhar V. A case of ochronosis: MRI of the lumbar spine. Neuroradiology. 2000. 42: 905-7
2. Elsas LJ, Longo N, Rosenberg LE, Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin JB, Kasper DL, Hauser SL, Longo DL.editors. Inherited disorders of amino acid metabolism and storage. Harrison’s Principles of Internal Medicine. New York: McGraw-Hill; 1998. p. 2194-203
3. Farzannia A, Shokouhi G, Hadidchi S. Alkaptonuria and lumbar disc herniation: Report of three cases. J Neurosurg. 2003. 98: 87-9
4. Feild JR, Higley GB, DeSaussure R. Ochronosis with ruptured lumbar disc: Case report. J Neurosurg. 1963. 20: 348-51
5. Fernández-Cañón JM, Granadino B, De Bernabé DB, Renedo M, Fernández-Ruiz E, Peñalva MA. The molecular basis of alkaptonuria. Nat Genet. 1996. 14: 19-24
6. Gürkanlar D, Daneyemez M, Solmaz I, Temiz C. Ochronosis and lumbar disc herniation. Acta Neurochirurg. 2006. 148: 891-4
7. Kahveci R, Ergungor MF, Gunaydin A, Temiz A. Alkaptonuric patient presenting with “black” disc: A case report. Acta Orthop Traumatol Turcica. 2013. 47: 134-8
8. La Du BN, Zannoni VG, Laster L, Seegmiller J. The nature of the defect in tyrosine metabolism in alcaptonuria. J Biol Chem. 1958. 230: 251-60
9. Laskar F, Sargison K. Ochronotic arthropathy: A review with four case reports. J Bone Joint Surg Br. 1970. 52: 653-66

