

- Neurosurgical Spine/Education, Department of NeuroScience, NYU Winthrop Hospital, Mineola, New York, USA
Correspondence Address:
Nancy E. Epstein
Neurosurgical Spine/Education, Department of NeuroScience, NYU Winthrop Hospital, Mineola, New York, USA
DOI:10.4103/sni.sni_177_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nancy E. Epstein, Renee D. Hollingsworth. Nursing review section of surgical neurology international: Part 1 lumbar disc disease. 07-Jul-2017;8:135
How to cite this URL: Nancy E. Epstein, Renee D. Hollingsworth. Nursing review section of surgical neurology international: Part 1 lumbar disc disease. 07-Jul-2017;8:135. Available from: http://surgicalneurologyint.com/surgicalint-articles/nursing-review-section-of-surgical-neurology-international-part-1-lumbar-disc-disease/
Date of Submission
08-May-2017
Date of Acceptance
11-May-2017
Date of Web Publication
07-Jul-2017
Abstract
Background:Patients with lumbar disc disease may present with low back pain, pain that radiates down into the lower extremity (radiculopathy), and leg pain that increases with ambulation (neurogenic claudication). Patients may first undergo diagnostic studies [(magnetic resonance imaging (MRI) and computed tomographic (CT) examinations] to determine whether there is any significant nerve root or thecal sac compression.
Methods:Increasingly, patients with low back pain with/without radiculopathy are being screened by nurses rather than by neurologists or neurosurgeons/orthopedists. Recognition of the basic neurological symptoms and signs of lumbar disc disease is critical to manage and triage these patients.
Results:The neurological examination includes evaluation of the straight leg raising test [straight leg raise (SLR)/Lasegue Maneuver], and assessment of: motor function [grade 0 (no motion) to 5 (normal motion)], reflexes [patellar and Achilles levels graded 0 (absent) to 4+ (clonus)], sensory loss (pin prick, light touch, position, and vibration), and cerebellar function (tandem gait, heel-shin, and finger-nose-finger). Learning to read MR and CT studies for disc herniations is critical. Nonsurgical discs include those that are minimally protruding or bulging. Alternatively, surgical disc herniations are extruded (ruptured through the annulus) or sequestrated (migrated beyond the disc space following rupture).
Conclusion:Familiarity with symptoms, neurological signs, and radiographic presentation for patients with lumbar disc disease is critical for nurses. Here we review the important factors nurses should know to better recognize/triage, and treat patients with lumbar disc disease.
Keywords: Bulging, extruded, far lateral disc, foraminal, laminectomy, laminotomy, lumbar discs, nonsurgical, nursing, sequestrated, surgical
INTRODUCTION
Nurses are increasingly seeing patients with low back pain and potential lumbar disc herniations in offices or hospital settings. They need to learn how to perform a neurological examination and correlate symptoms (complaints) with neurological findings (signs). Familiarity with the various radiographic studies including X-rays, magnetic resonance images (MRI), and computed tomographic (CT) studies is critical if nurses want to actively contribute to the care of these patients [Figures
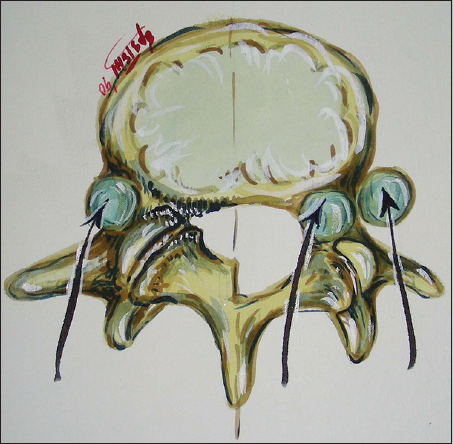
Figure 1
Illustration of location of lumbar discs. This illustration (Joseph A. Epstein M.D./Copyright Nancy E. Epstein M.D.) shows the different locations of lumbar discs; they may be located inside the spinal canal (centrally or laterally) or as shown blue), outside the spinal canal (e.g., proximal or distal foraminally (at the beginning or end of the foramen) and far laterally (beyond the facet joint

Figure 2
Axial MR of right L5-S1 lumbar disc (extruded). This axial T2 weighted MR image (T2 means the spinal fluid is white/hyperintense) demonstrated a right-sided L5-S1 disc herniation compressing the S1 nerve root. Note the additional marked anterorlateral compression of the dura/thecal sac containing the cauda equina


Figure 4
Axial noncontrast CT showing a massive extruded/sequestrated L5-S1 disc with right-sided inferior migration opposite S1. This axial noncontrast CT demonstrated massive right-sided extruded/sequestrated disc at the L5S1 level with marked right-sided inferior migration opposite the S1 pedicle. Note severe compromise of the thecal sac and obliteration of the S1 nerve root

Figure 5
Noncontrast CT of left lateral/foraminal/far lateral disc at the L3-L4 level. This non contrast CT scan demonstrates a left sided lateral/foraminal/far lateral disc herniation resulting in some anterolateral compression of the dural sac, but marked obliteration of the superiorly exiting L3 nerve root as well as compression of the inferior L4 nerve root. Here, the patient may require a full facetectomy [see
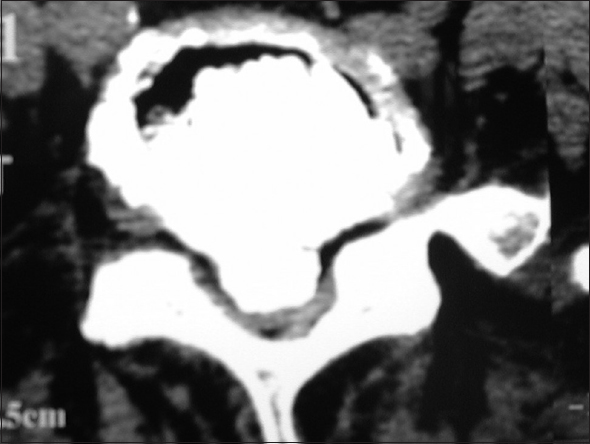
Figure 6
Noncontrast axial CT of massive central calcified disc/limbus fracture filling the spinal canal contributing to cauda equina compression. The axial noncontrast CT demonstrated calcification/ossification of a massive central disc herniation filling the spinal canal at the L4-L5 level. This is also called a limbus fracture. This patient presented with a cauda equina syndrome (paralysis) and required removal of this disc through a coronal hemilaminectomy [See Figures
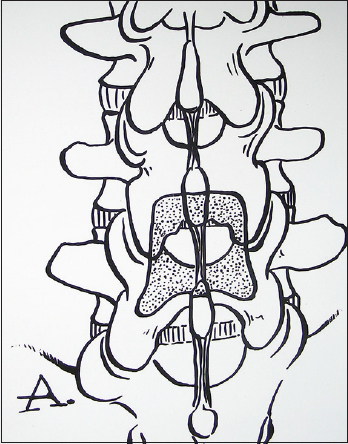
Figure 7
Illustration before removal of the L4-lamina above and L5-lamina below to perform a coronal hemilaminectomy. This illustration (Joseph A. Epstein M.D./Copyright Nancy E. Epstein M.D.) shows how much of the bone that will have to be removed to perform a coronal hemilaminectomy at the L4-L5 level. This involves removing half of the lamina above (L4) and half of the lamina below the L4-L5 disc space level
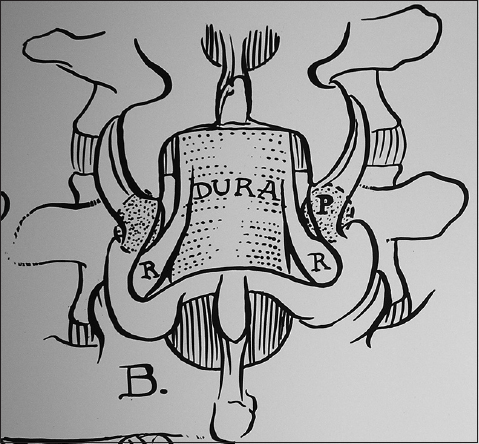
Figure 8
Coronal hemilaminectomy L4-L5 level (removal of half of L4 and half of L5 laminae). In this illustration (Joseph A. Epstein M.D./Copyright Nancy E. Epstein M.D.) half of the lower part of the L4 lamina and half of the upper part of the L5 laminae have been removed. This constitutes a coronal or partial laminectomy of both the L4 and L5 levels, potentially allowing access to a central disc herniation at that level. Note adequate visualization of both L5 roots (on either side) and the central thecal sac (nerve tissue in the middle)

Figure 9
Left-sided laminotomy at L4-L5 and right-sided hemilaminectomies at the L3-L4, L4-L5 and L5-S1 levels. This illustration (Joseph A. Epstein M.D./Copyright Nancy E. Epstein M.D.) demonstrates on the left, a laminotomy at the L4-L5 level (removal of half of the lamina of L4 above and half of L5 below). On the right-side, the lower part of L3 (laminotomy), but all the L4 and L5 laminae (hemilaminectomies) have been removed to decompress the L3-4, L4-L5, and L5-S1 levels
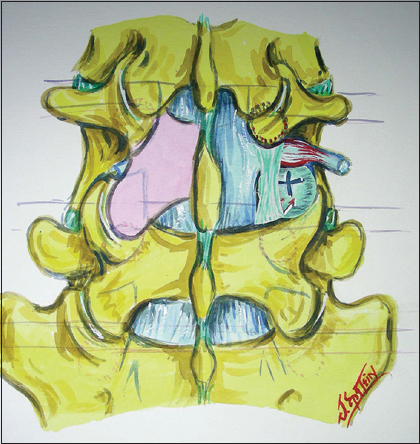
Figure 10
Unilateral inferior facetectomy vs. full facet removal during laminectomy. This figure (Joseph A. Epstein M.D./Copyright Nancy E. Epstein M.D.) illustrates a laminectomy at the L4 level (both sides). The left inferior articular facet (L4 lower facet on the left) has been removed, but the superior articular facet (connected to the L5 lamina) is still intact. On the right, the entire L4-L5 facet has been removed to allow for excision of a far lateral free disc fragment (seen way off to the side)
Symptoms of lumbar disc herniations
Symptoms are defined by patients’ complaints. These typically include pain, numbness/burning, tingling, and weakness in a specific nerve root distribution down a leg (radiculopathy). If the compression involves multiple nerves, then the deficit may be multifocal; this is often defined as cauda equina compromise.
NEUROLOGICAL SIGNS (EXAMINATION) FOR A LUMBAR DISC HERNIATION
How to perform a neurological exam for a lumbar disc herniation
First, one performed a straight leg raising test (e.g., with the patient seated, the leg is elevated to 90 degrees). This stretches/tethers the nerve over a disc and produces pain at a certain height. For example, severe pain would correlate with a positive straight leg raise (SLR) test at 10–20 degrees, moderate at 30–50 degrees, and mild at 60–80 degrees. Next the motor examination is assessed using a 6-point scale; 0 (no function/paralysis) -5 (normal). The motor exam includes (with the patient seated); assessment of: iliopsoas function (elevate the knee), quadriceps strength (straighten the leg out), dorsiflexion (pull the foot up), and plantar flexion (push the foot down—give me 90 miles an hour). The reflexes are assessed on a 5-point scale: 0 (absent) -4+ (clonus); additionally the Babinski response (stimulating the bottom of the foot) may indicate cord compression. The cerebellar exam includes evaluation of tandem gait (walking on a straight line with one foot in front of the other (test for inebriation)), and heel-shin (placing one foot over the knee and sliding it down the shin without wavering).
Magnetic resonance scans of lumbar disc herniations
MR scans best demonstrate soft tissue (e.g., like the chocolate side an M&M) [Figures
Computed tomographic scans
CT images best show the bone (e.g., the hard candy shell of the M&M). They will clearly demonstrate in a positive image the actual location of the bone itself, and other calcified/ossified tissues [Figures
TYPES OF DISCS
Bulging and protruding discs (nonsurgical lesions)
Nonsurgical degenerative changes of lumbar discs are frequently found on MR scans of the lumbar spine. These findings increase in frequency with age. Neither bulging nor protruding discs significantly compress nerve tissue.
Extruded and sequestrated lumbar discs
Disc herniations that go through the annulus of the disc (the surrounding capsule of the disc) may be surgical lesions. Extruded discs have ruptured through the annulus, but the fragment(s) are still in continuity with the disc space itself. Alternatively, the sequestrated disc has not only ruptured through the annulus, but the fragments have migrated away from the capsule, extending above, below, or to the side of the disc level.
Abnormal neurological exam that may correlate with a lumbar disc herniation
Neurological signs of significant surgical lumbar disc herniations may include positive femoral stretch tests (L2-L4) or SLR signs plus the following focal neurological deficits.
L1-L2 and L2-L3 discs (proximal lumbar disc herniations)
At the L1-L2 level, if the disc is off to one side, the patient may be unable to lift the knee (while seated; weakness of the iliopsoas), straighten the knee (quadriceps) have an absent knee jerk (patellar response), and have numbness in the thigh (L1, L2, L3 distributions). When the disc fills the spinal canal at this level, the patient may present with paralysis (cauda equina syndrome) involving sphincter (bowel/bladder) dysfunction (incontinence).
L3-L4 discs
The patient with a unilateral L3-L4 disc may demonstrate weakness elevating the thigh (iliopsoas) and straightening out the leg (quadriceps), a loss of the knee reflex (patellar response), and decreased pin appreciation in the L3-L4 distributions (anterior thigh; inside of the calf). If this is on both sides, and fills the canal, the patient may be paralyzed and exhibit a cauda equina syndrome with sphincter dysfunction.
L4-L5 discs
Unilateral disc herniations at the L4-L5 level may present as a foot drop: weakness of the extensor hallucis longus (L5 distribution), accompanied by a loss or decrease of the ankle reflex (Achilles response), and decrease in pin appreciation in the L5 distribution (outside of the calf and over the top of the foot).
L5-S1 discs
Disc herniations at the L5-S1 level on one side typically compress the S1 nerve root. Patients may demonstrate an inability to walk on the toes on that side (plantar flexor weakness, a loss of the ankle reflex (Achilles response), and decreased pin appreciation on the lateral aspect of the foot.
Lumbar decompressive procedures
There are different types of lumbar decompressive operations available for lumbar spine surgery [Figures
Coronal hemilaminectomy
A laminectomy involves removal of the bone on both sides to decompress the entire level. This may involve removal of a portion of the lamina above and below the disc space to be decompressed. For example, if the disc were bilateral (both sides) at the L4-L5 level, a coronal hemilaminotomy (removal of half lower part of the lamina L4 above and half of the L5 lamina below) would be removed.
Laminotomy
However, one can also just removed part of the lamina above and below one disc space to address a one-sided disc herniation. This is called a laminotomy. For example, if there were a disc herniation at the L4-L5 level on just one side, then the lower part of the L4 hemilamina above and the upper portion of the L5 lamina below would be removed. This can be repeated at any level.
Laminotomy on one side and multilevel hemilaminectomy on the other side
In some cases, patients may warrant a laminotomy (partial removal of the lamina above/below) at one interspace on one side, while there is multilevel stenosis requiring removal of the hemilaminae (half of the laminae) on the other side.
Laminectomy with different degrees of facet removal to address foraminal and far lateral discs
In cases where a patient has a lumbar disc herniation extending laterally, foraminally, or far laterally (way off to the side), more extensive facet resection (removal) may have to accompany the laminectomy. When the disc is located underneath the facet joint (foraminally), one may be able to access the disc by removing the inferior articular facet (seen on the left side of the diagram). However, if the disc is found far laterally, beyond the facet joint full facet removal may be warranted.
CONCLUSION
This is just a short introduction for nurses who want to become more familiar with the symptoms, signs, and radiographic (X-ray, MR, and CT) findings typical for lumbar disc herniations.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.

