

- Department of Surgery, Faculty of Medical, Universitas Kristen Indonesia, Jakarta, Indonesia.
DOI:10.25259/SNI_523_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Robert Sinurat. Occipitocervical fixation using Ransford loop for neglected posttraumatic odontoid fracture with atlantoaxial dislocation: A technical note. 15-Nov-2019;10:218
How to cite this URL: Robert Sinurat. Occipitocervical fixation using Ransford loop for neglected posttraumatic odontoid fracture with atlantoaxial dislocation: A technical note. 15-Nov-2019;10:218. Available from: http://surgicalneurologyint.com/surgicalint-articles/9752/
Date of Submission
19-Oct-2019
Date of Acceptance
23-Oct-2019
Date of Web Publication
15-Nov-2019
Abstract
Background: To relieve the onset of new clinical symptoms, it is important to recognize and treat previously neglected odontoid fractures. However, many hospitals in developing countries do not have the equipment or surgical expertise to adequately manage these lesions.
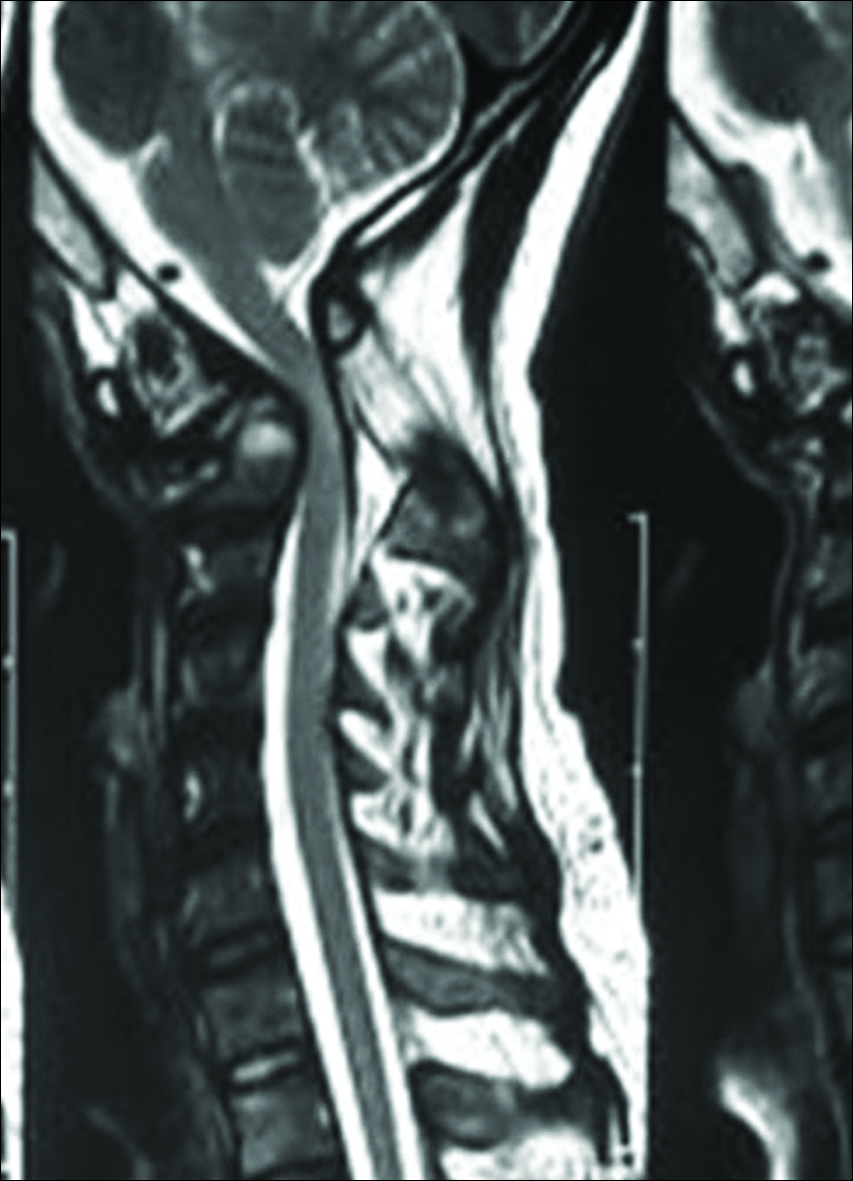
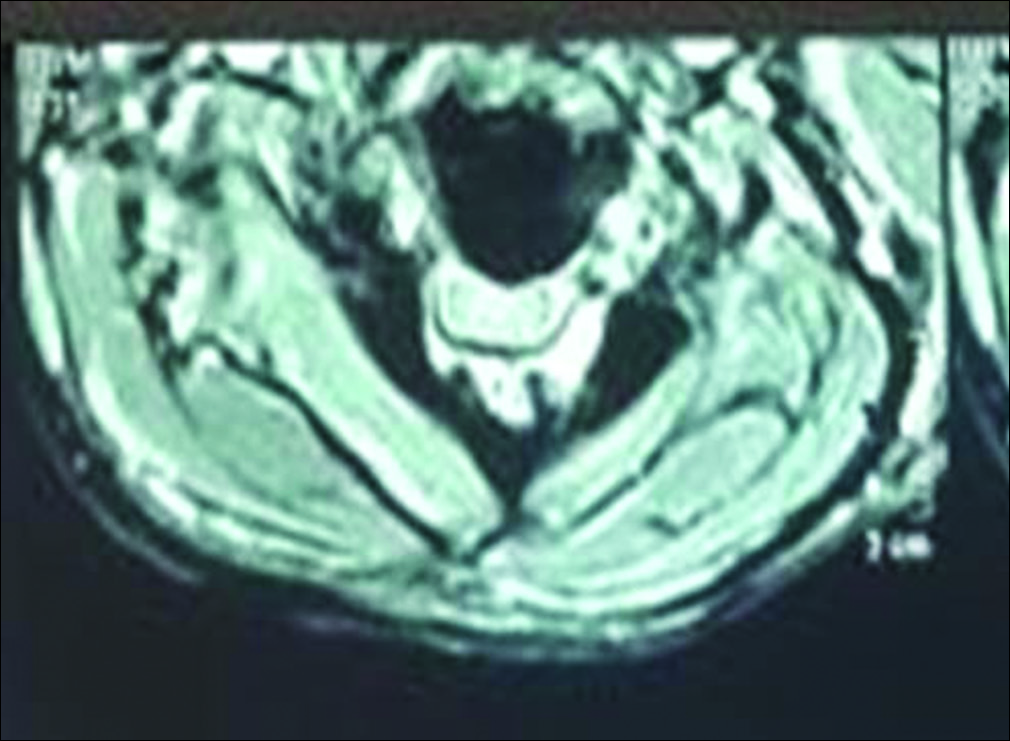
Case Description: A 31-year-old male presented with paresthesias/quadriparesis attributed to an accident sustained 6 months earlier. The cervical magnetic resonance image revealed atlantoaxial subluxation type 2. Following a laminectomy and occipitocervical fusion with a Ransford loop, the patient’s symptoms significantly improved.
Conclusion: Straight forward laminectomy and occipitocervical fusion with a Ransford loop may adequately treat selected cases of neglected atlantoaxial subluxation in a developing country.
Keywords: Atlantoaxial subluxation, Equipment, Stabilization
INTRODUCTION
About 10–20% of cervical fractures involve the odontoid. Type 2 odontoid fractures typically do not heal well without surgery.[
CASE REPORT
Six-month duration following a motorbike accident, a 31-year-old male presented with neck pain, paresthesias, quadriparesis, and bilateral ankle clonus. Upper extremity (3/5) and lower extremity strength (4/5) were compromised. The cervical magnetic resonance image showed atlantoaxial subluxation type 2©, with an increased atlantodens interval (ADI), a decreased posterior ADI, and an increased interspinous distance.[
Operative procedures
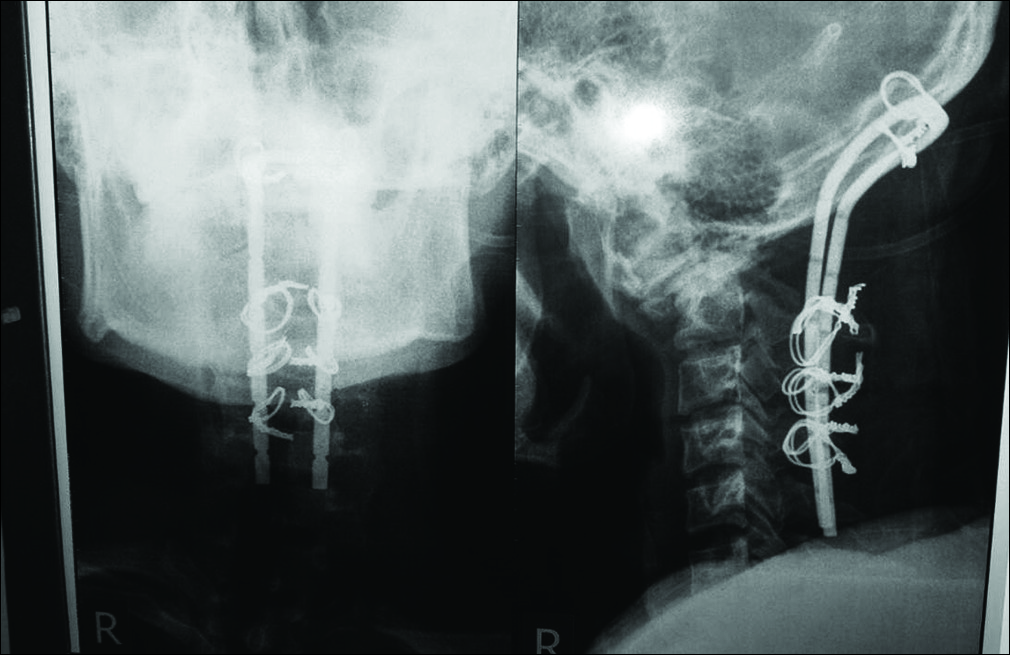
An incision was started from the occiput to C7. The posterior ring of C1 was drilled 1 cm lateral to the midline on both sides; additionally, a laminectomy was performed involving the upper part of the lamina of C2 bilaterally. Two small burr holes were placed in the occipital region; a Ransford loop affixed to the occipital bone using 1.5 mm wires. Similarly, the lamina of C2-C4 was fixed using 1.5 mm sublaminar wires. The patient was discharged on postoperative day 7 without any changes in his neurological status. The postoperative X-ray showed that the Ransford loop had remained in good position [
DISCUSSION
Poorly managed odontoid fractures are a common problem in underdeveloped countries due to many factors, for example, socioeconomic problems, overlooked diagnoses, and poor access to health care.[
CONCLUSION
Selected patients with neglected odontoid type 2 fractures with atlantoaxial dislocation type C can be managed utilizing a simple laminectomy decompression and occipitocervical stabilization using Ransford loops and wire.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aggarwal RA, Rathod AK, Chaudhary KS. Irreducible atlanto-axial dislocation in neglected odontoid fracture treated with single stage anterior release and posterior instrumented fusion. Asian Spine J. 2016. 10: 349-54
2. Evaniew N, Yarascavitch B, Madden K, Ghert M, Drew B, Bhandari M. Atlantoaxial instability in acute odontoid fractures is associated with nonunion and mortality. Spine J. 2015. 15: 910-7
3. Sengupta DK. Neglected spinal injuries. Clin Orthop Relat Res. 2005. 431: 93-103
4. Shetty A, Kini AR, Prabhu J. Odontoid fractures: A retrospective analysis of 53 cases. Indian J Orthop. 2009. 43: 352-60
5. Shetty A, Kumar A, Chacko A, Guthe S, Kini AR. Reduction techniques in the management of atlantoaxial subluxation. Indian J Orthop. 2013. 47: 333-9
6. Yang SY, Boniello AJ, Poorman CE, Chang AL, Wang S, Passias PG. A review of the diagnosis and treatment of atlantoaxial dislocations. Global Spine J. 2014. 4: 197-210

