

- Department of Neurosurgery, Lausanne University Hospital, Lausanne, Switzerland,
- Department of Clinical Neurosciences, Spine Unit, Lausanne University Hospital, Lausanne, Switzerland.
DOI:10.25259/SNI_22_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Alberto Vandenbulcke1, Giulia Cossu1, Juan Barges Coll2. Pharyngeal perforation: A rare complication of occipitocervical injury. 28-Jun-2021;12:308
How to cite this URL: Alberto Vandenbulcke1, Giulia Cossu1, Juan Barges Coll2. Pharyngeal perforation: A rare complication of occipitocervical injury. 28-Jun-2021;12:308. Available from: https://surgicalneurologyint.com/surgicalint-articles/10928/
Date of Submission
10-Jan-2021
Date of Acceptance
21-May-2021
Date of Web Publication
28-Jun-2021
Abstract
Background: Atlantoaxial dislocation is a rare injury following high-energy trauma. We report an undescribed complication of atlantoaxial dislocation.
Case Description: A 75-year-old man presented with atlantoaxial dislocation and Jefferson C1 fracture after a high-energy trauma. Occipitoaxial stabilizations were performed the day after. A nasopharyngeal fistula was identified at day 5 causing a persistent epistaxis.
Conclusion: Nasopharyngeal fistulization of C1 bony fragment is a rare complication of complex occipitocervical injury. Combined treatment with ENT surgeon should be considered.
Keywords: Atlantoaxial dislocation, Craniocervical junction, Craniocervical stabilization, Jefferson fracture, Rhinopharyngeal fistulizations
IMAGE REPORT
A 75-year-old man was the victim of a high-energy road accident. When emergency medical services arrived, he was in cardiac arrest (CA) and presented bilateral nonreactive mydriatic pupils. A rigid cervical collar was applied, and cardiopulmonary resuscitation (CPR) was initiated. CPR was discontinued after 12 min when spontaneous circulation returned. A Glasgow Coma Scale of 3 was described. The patient was intubated, fully sedated on site and airlifted to our emergency room.
When we performed the neurological evaluation, he presented with symmetric miotic nonreactive pupils and a preserved oculocardiac reflex and a polytrauma CT scan showed a Jefferson fracture of C1 with anterior atlantoaxial dislocation [
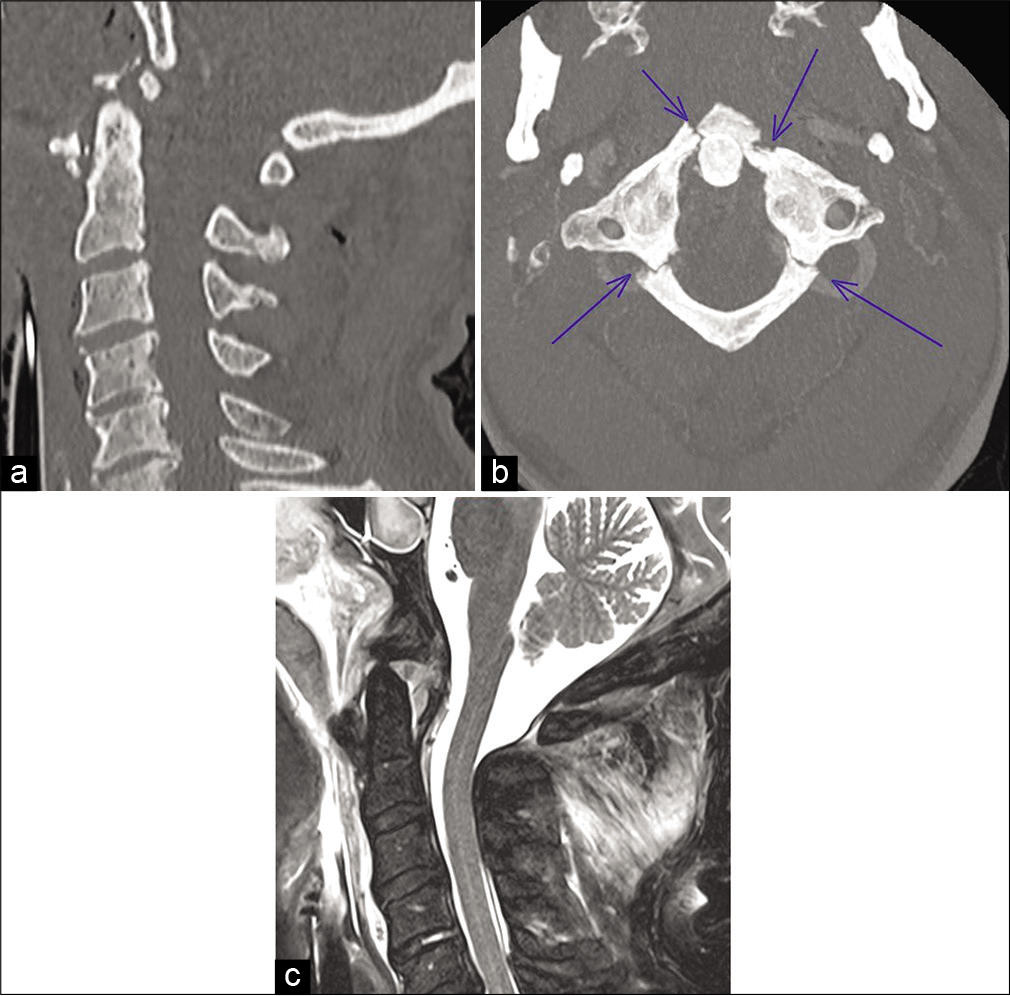
Figure 1:
(a) Sagittal bone CT sequence showing anterior dislocation of C2, with a basion density interval of 16 mm and multifragmented fracture of the anterior C1 arc. (b) Axial bone CT sequence showing a Jefferson fracture of C1: bilateral fracture of the anterior and posterior arcs pointed by the blue arrows. (c) Sagittal T2-weighted MRI sequence showing the anterior dislocation of C2 associated with prevertebral hematoma and suspicion of pharyngeal perforation from the anterior arc fragments.
A prevertebral hematoma from C2 to C5 was also present, with a suspicion of pharyngeal perforation from the anteriorly displaced C1 fragment [
Considering the fracture’s high instability, the absence of major cerebral lesions at cerebral MRI performed 4 h after the trauma and the presence of brainstem reflexes, occipitoaxial stabilization with an occipital plate, and C2 pars screws was performed the day after the trauma. A postoperative CT scan confirmed a correct placement of the pars screws with no major displacement of the C1 bony fragment [

On postoperative day 5, a second ENT evaluation was performed following an episode of massive epistaxis. A nasopharyngeal fistula of the thin mucosal layer identified preoperatively, with exposure of a bony fragment of C1 [

Occipitocervical bony and ligamentous lesions are rare fatal injuries following high-energy trauma.[
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Dickman C, Greene K, Sonntag V. Injuries involving the transverse atlantal ligament. Neurosurgery. 1996. 38: 44-50
2. Kandziora F, Scholz M, Pingel A, Schleicher P, Yildiz U, Kluger P. Treatment of atlas fractures: Recommendations of the spine section of the german society for orthopaedics and trauma (DGOU). Glob Spine J. 2018. 8: 5S-11S
3. Lee EJ, Jang JW, Choi SH, Rhim SC. Delayed pharyngeal extrusion of an anterior odontoid screw. Korean J Spine. 2012. 9: 289
4. Mendenhall SK, Sivaganesan A, Mistry A, Sivasubramaniam P, McGirt MJ, Devin CJ. Traumatic atlantooccipital dislocation: Comprehensive assessment of mortality, neurologic improvement, and patient-reported outcomes at a Level 1 trauma center over 15 years. Spine J. 2015. 15: 2385-95
5. Orlando ER, Caroli E, Ferrante L. Management of the cervical esophagus and hypofarinx perforations complicating anterior cervical spine surgery. Spine (Phila Pa 1976). 2003. 28: 290-5

