

- Department of Neurosurgery, Rasool Akram Hospital, Tehran, Iran
Correspondence Address:
Morteza Taheri
Department of Neurosurgery, Rasool Akram Hospital, Tehran, Iran
DOI:10.4103/sni.sni_87_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Tabibkhooei A, Taheri M, Rohani S, Azimi A. Polyostotic craniofacial fibrous dysplasia with bizarre radiologic finding: Mandible, anterior skull base, frontal, temporal, parietal, and occipital bones involvement. Surg Neurol Int 01-Aug-2017;8:160
How to cite this URL: Tabibkhooei A, Taheri M, Rohani S, Azimi A. Polyostotic craniofacial fibrous dysplasia with bizarre radiologic finding: Mandible, anterior skull base, frontal, temporal, parietal, and occipital bones involvement. Surg Neurol Int 01-Aug-2017;8:160. Available from: http://surgicalneurologyint.com/surgicalint-articles/polyostotic-craniofacial-fibrous-dysplasia-with-bizarre-radiologic-finding-mandible-anterior-skull-base-frontal-temporal-parietal-and-occipital-bones-involvement/
Date of Submission
24-Feb-2017
Date of Acceptance
27-May-2017
Date of Web Publication
01-Aug-2017
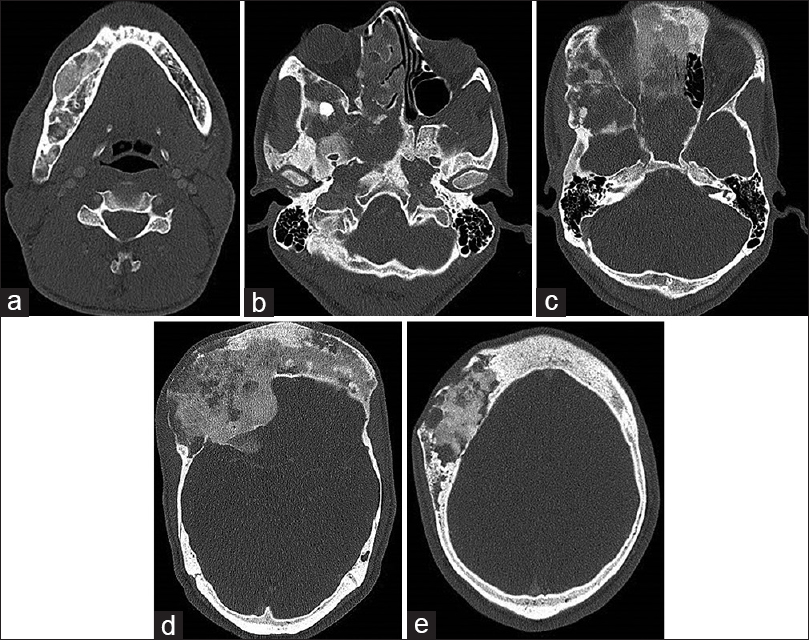
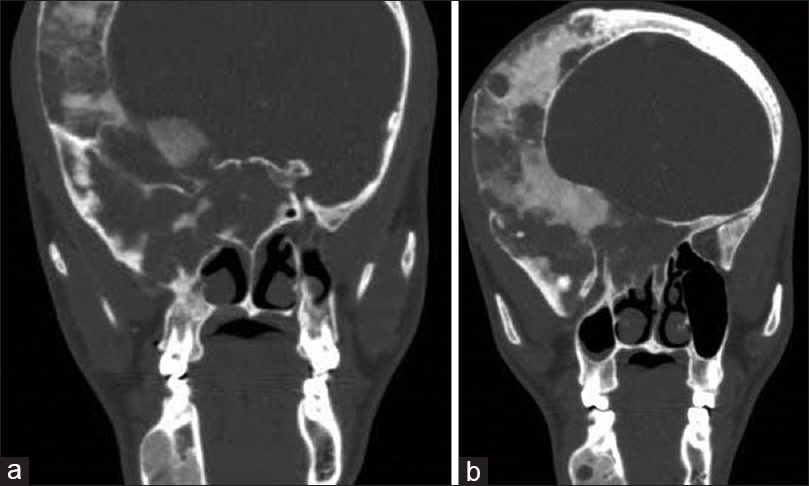
A 30-year-old man presented with progressive blurred vision and cosmetic facial problems within 2 years ago. Neurological examination demonstrated impaired visual acuity and constricted visual field associated with both forehead and right side craniofacial deformity in the general examination. The craniofacial computed tomography (CT) scan showed expansion and thickening in right mandible, anterior skull base (including sphenoid, orbital roof, and ethmoidal bones), clival part of the occipital bone, right temporal, frontal, and parietal bones and also left frontal bone [Figures
DISCUSSION
Fibrous dysplasia (FD) is an uncommon benign disorder with unknown etiology, although variety causative factors explained. It divides into two primary types. First, monostotic type involves one bone and the second, polyostotic type that involves more than one bone.[
Clinically FD result to pain, deformity, fracture, and nerve entrapments,[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bowers CA, Taussky P, Couldwell WT. Surgical treatment of craniofacial fibrous dysplasia in adults. Neurosurg Rev. 2014. 37: 47-53
2. Guruprasad Y, Prabhakar C. Craniofacial polyostotic fibrous dysplasia. Contemp Clin Dent. 2010. 1: 177-9
3. Júnior SV, Andrade EC, Didoni ALS, Jorge JC, Filho SN, Yoshimoto FR. Displasia fibrosa do osso temporal: Relato de caso e revisão da literatura. Braz J Otorhinolaryngol. 2004. 70: 828-31
4. Mrabet D, Rekik S, Sahli H, Ben Amor M, Meddeb N, Sellami S. An extensive hemimelic polyostotic fibrous dysplasia: A case report. Rheumatol Int. 2012. 32: 1075-8
5. Swain SK, Sahu MC. An extensive Fibrous dysplasia of anterior skull base area of a 12-year-old boy – A case report. Pediatria Polska. 2016. 91: 636-9

