

- Department of Neurosurgery, Higashiyamato Hospital, Higashiyamato,
- Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fujieda, Japan.
Correspondence Address:
Sho Nakamura, Department of Neurosurgery, Higashiyamato Hospital, Higashiyamato, Japan.
DOI:10.25259/SNI_353_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sho Nakamura1, Toshiyuki Takahashi2, Manabu Minami2, Ryo Kanematsu2, Izumi Suda2, Junya Hanakita2, Shinya Tokunaga2, Shu Takeuchi2. Postoperative intractable leg pain caused by dislocation of drainage tube. 19-May-2023;14:177
How to cite this URL: Sho Nakamura1, Toshiyuki Takahashi2, Manabu Minami2, Ryo Kanematsu2, Izumi Suda2, Junya Hanakita2, Shinya Tokunaga2, Shu Takeuchi2. Postoperative intractable leg pain caused by dislocation of drainage tube. 19-May-2023;14:177. Available from: https://surgicalneurologyint.com/surgicalint-articles/12328/
Date of Submission
22-Apr-2023
Date of Acceptance
06-May-2023
Date of Web Publication
19-May-2023
Abstract
Background: A wide variety of conditions can cause recurrent postoperative lumbar radiculopathy.
Case Description: A 49-year-old female developed sudden recurrent postoperative right leg pain after a right-sided L5S1 microdiskectomy for a herniated disc. Emergent magnetic resonance and computed tomography studies demonstrated migration of the drainage tube into the right L5S1 lateral recess compromising the S1 nerve root. Following drain removal, the patient’s right reg pain immediately resolved.
Conclusion: Migration of a lumbar wound drain into the operated lateral recess following a lumbar diskectomy may result in acute, recurrent/intractable radicular pain that was readily resolved with drain removal.
Keywords: Drainage tube, Lumber disc herniation, Radiculopathy, Spine surgery
INTRODUCTION
Placement of a drain in a lumbar wound following a lumbar diskectomy is a common practice to prevent postoperative epidural hematomas (EDH).[
CASE DESCRIPTION
A 49-year-old female underwent a right L5S1 microdiskectomy for a lumber disc herniation. At surgery, a wound drain was placed [
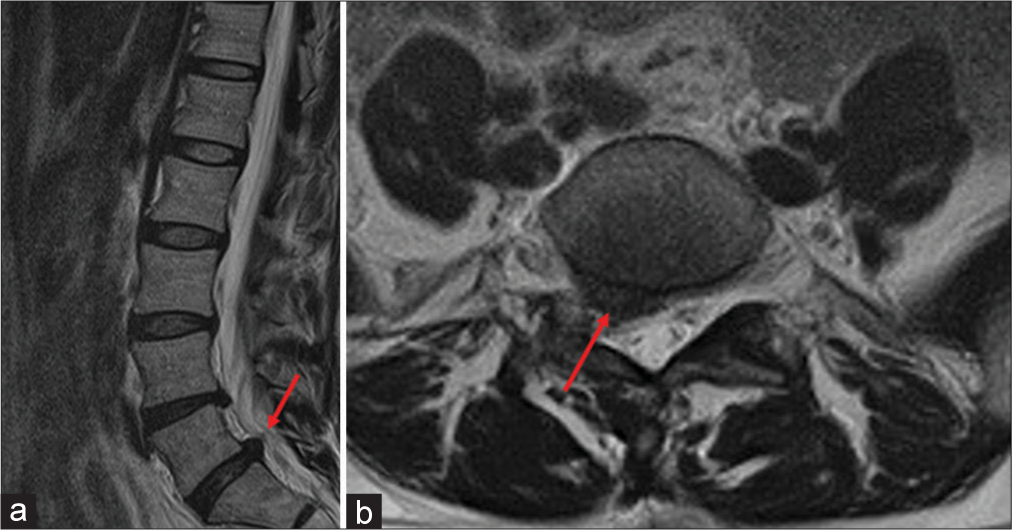

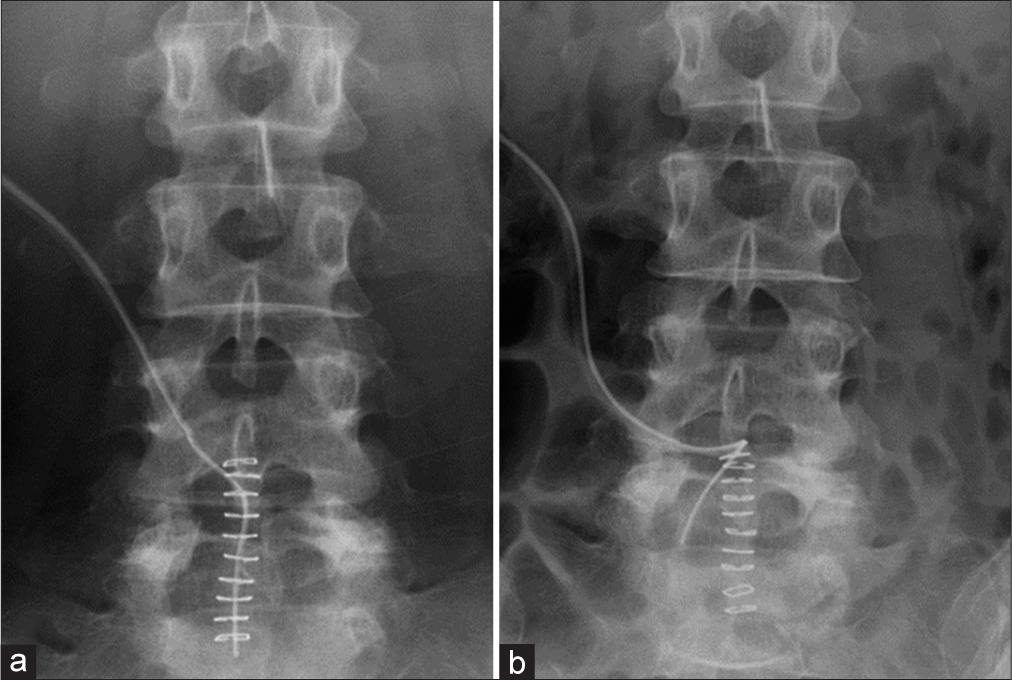
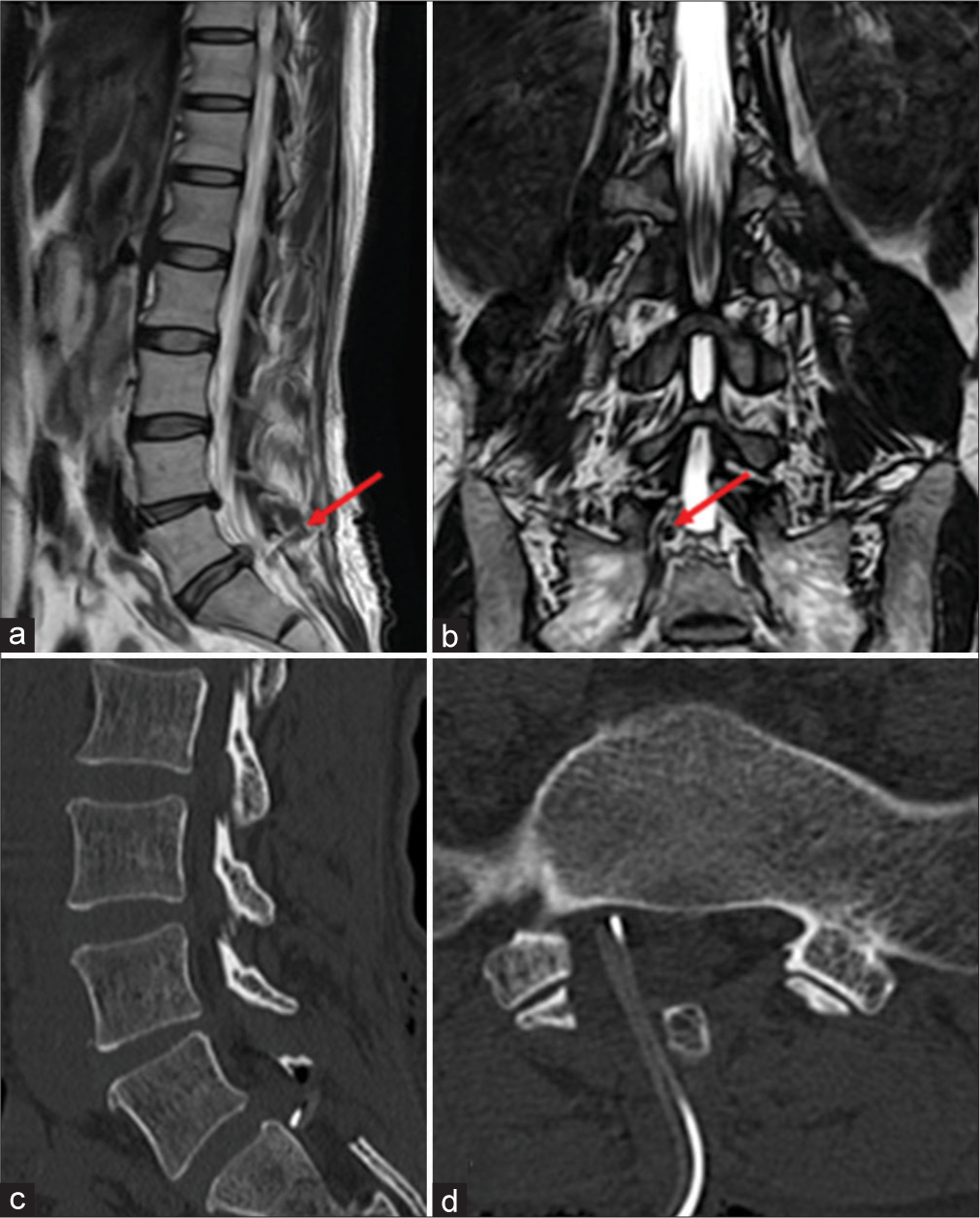
Figure 4:
(a and b) Postoperative magnetic resonance imaging. (a and b) T2-weighted image in sagittal section and constructive interference in steady state in coronal section showed spinal nerve root compression with drainage tube (red arrow). (c and d) Postoperative computed tomography (CT). (c and d) Drainage tube was migrated into the right L5S1 lateral recess on sagittal and axial CT images.
DISCUSSION
Recurrence of radicular pain after a lumber diskectomy is most commonly attributed to: Postoperative EDH contributing to cauda equina syndromes, cerebrospinal fluid leaks/fistulas (i.e., including root extrusion through durotomy sites or loculated cerebrospinal fluid compressing the cauda equina), or recurrent disc herniations.[
CONCLUSION
Following lumbar diskectomy, wound drains may rarely migrate into the operated lateral recesses causing symptomatic recurrent radiculopathy. In these instances, X-ray, MR, and CT confirmation of drain migration should prompt early drain removal to achieve rapid symptom resolution.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Glotzbecker MP, Bono CM, Wood KB, Harris MB. Postoperative spinal epidural hematoma: A systematic review. Spine (Phila Pa 1976). 2010. 35: E413-20
2. Heindel P, Tuchman A, Hsieh PC, Pham MH, D’Oro A, Patel NN. Reoperation rates after single-level lumbar discectomy. Spine (Phila Pa 1976). 2017. 42: E496-501
3. Mirzai H, Eminoglu M, Orguc S. Are drains useful for lumbar disc surgery? A prospective, randomized clinical study. J Spinal Disord Tech. 2006. 19: 171-7
4. Pavlou G, Bucur SD, van Hille PT. Entrapped spinal nerve roots in a pseudomeningocoele as a complication of previous spinal surgery. Acta Neurochir (Wien). 2006. 148: 215-9
5. Valente A, Nicodemo A, Bruno A, Massè A. Cerebrospinal fluid fistulas after iliosacral screw removal in post-traumatic pseudomeningocele. J Orthop Traumatol. 2012. 13: 111-4


Gabriel Jungberg
Posted June 1, 2023, 4:49 pm
I do not remember to leave a wound drain in more than 2000 lumbar microdiskectomy. Even if a patient develop a wound haematoma it will be limited to the small space of the approach and with a little possibility of nerve root compression. Now my standard is MISS diskectomy and still do not leave a wound drain.