

- Department of Neurosurgery, Iran University of Medical Sciences, Rasoul Akram Hospital, Tehran, Iran.
- Department of Neurosurgery, Iran University of Medical Sciences, Rasoul Akram Hospital, Tehran, Iran.
Correspondence Address:
Seyed Mohammad Reza Mohajeri, Department of Neurosurgery, Iran University of Medical Sciences, Rasoul Akram Hospital, Tehran, Iran.
DOI:10.25259/SNI_462_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Arash Fattahi1, Abdoulhadi Daneshi1, seyed Mohammad Reza Mohajeri2. Posttraumatic C2-C3 spondyloptosis without focal neurological deficit, treated with anterior and posterior approaches: A case report. 06-Jul-2021;12:332
How to cite this URL: Arash Fattahi1, Abdoulhadi Daneshi1, seyed Mohammad Reza Mohajeri2. Posttraumatic C2-C3 spondyloptosis without focal neurological deficit, treated with anterior and posterior approaches: A case report. 06-Jul-2021;12:332. Available from: https://surgicalneurologyint.com/surgicalint-articles/10946/
Date of Submission
09-May-2021
Date of Acceptance
13-Jun-2021
Date of Web Publication
06-Jul-2021
Abstract
Background: Cervical spondyloptosis is usually caused by trauma, and correlated with significant neurological deficits that can include quadriplegia, respiratory disorders, vertebral artery injury, and death.
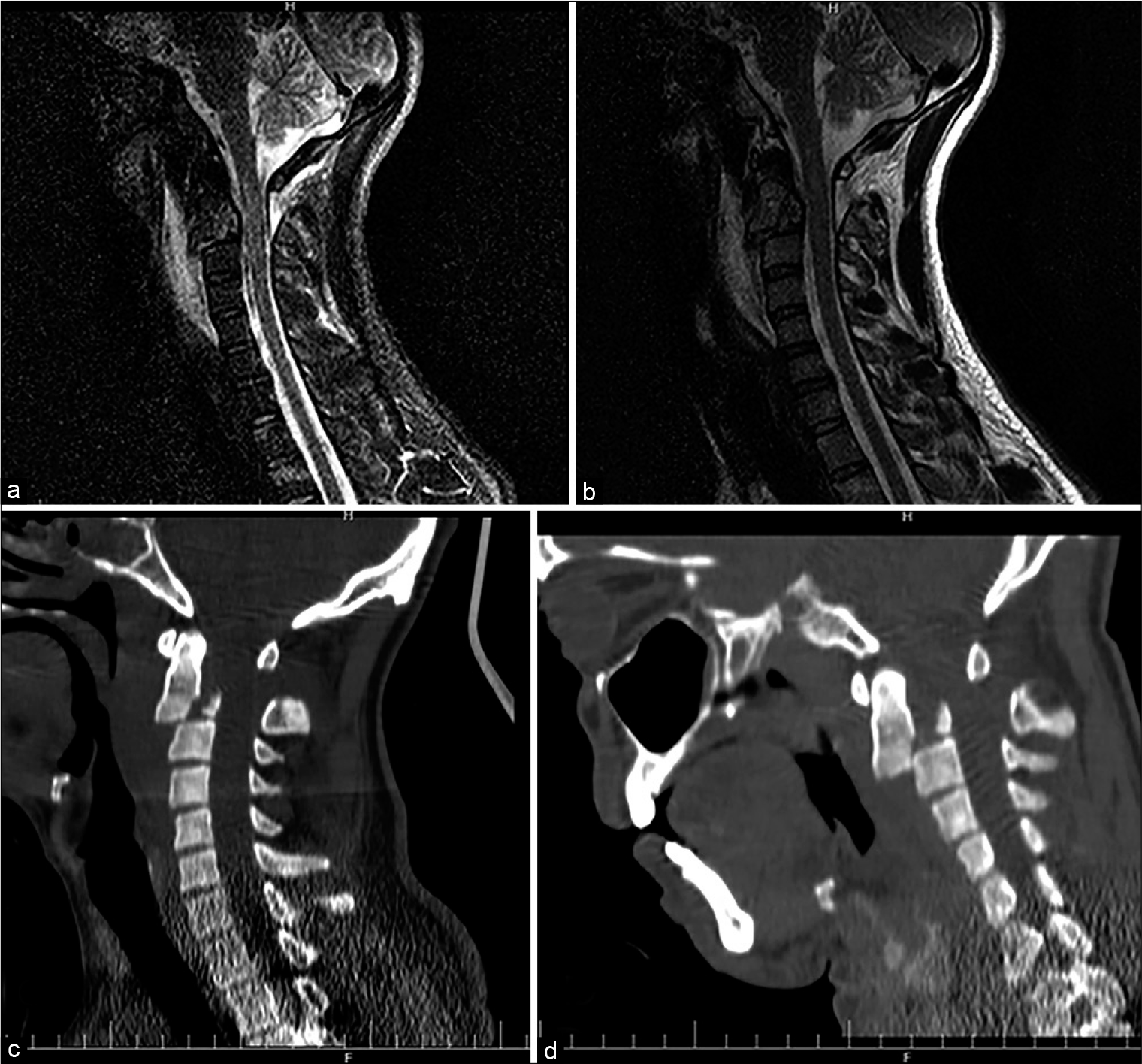
Case Description: A 34-year-old male presented with C2-C3 spondylolisthesis after a fall from a tree. Although he had no neurological deficits, CT and X-ray studies confirmed C2-C3 a spondyloptosis. He was treated with emergent anterior and posterior cervical reduction, decompression, and fixation, remaining neurologically intact in the postoperative period.
Conclusion: Patients with C2-C3 spondyloptosis documented on X-ray/CT studies should be considered for circumferential decompression/fusion to preserve neurological function.
Keywords: Cervical fusion, Cervical spondyloptosis, Hangman’s fracture, Trauma
INTRODUCTION
Cervical spondyloptosis is the most severe type of spondylolisthesis and is[
CASE STUDY
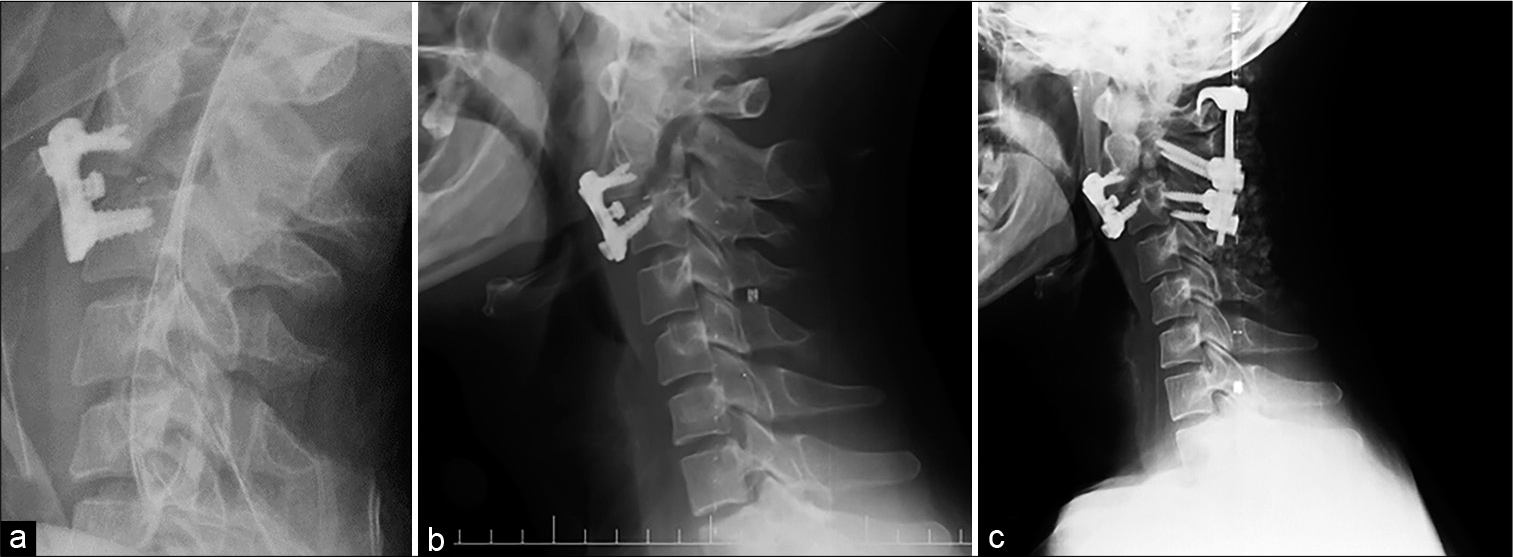
A 34-year-old male fell from a tree 3 m high. When transferred, he was neurologically intact. The cervical CT scan demonstrated traumatic C2-C3 spondylolisthesis with bilateral C2 pars interarticularis fractures (i.e. A hangman’s fracture). The patient underwent Gardner-Wells traction (i.e. 7.5 kg). However, when this failed to provide realignment, he first underwent an anterior fusion Consisting of C2-C3 discectomy, partial C2 and C3 corpectomy with cage/plate placement [
Three weeks later, due to increased anterior displacement, a secondary posterior fusion was performed warranting. C1-C3 fusion with bilateral C1 hooks, C2 trans-pars screws, and C3 lateral mass screws and rods. Four months later, the patient went on to fuse without any neurological deficit [
DISCUSSION
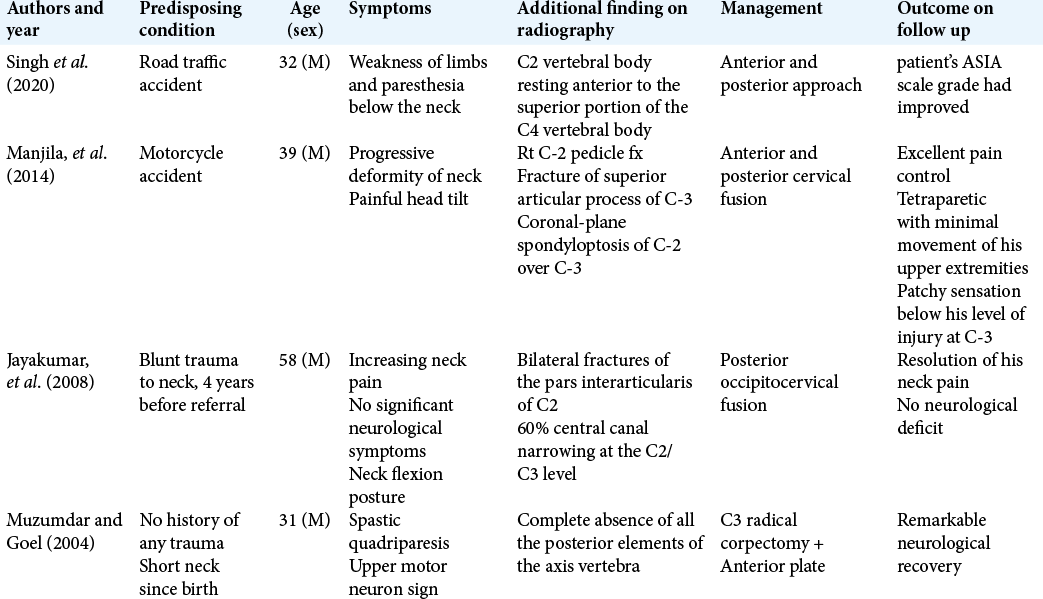
We identified four other cases of spondyloptosis at the C2-C3 level. These were attributed to; new trauma (1 case), old trauma (1 case), absence of all C2 vertebral posterior elements, (1 case), and a motor vehicle accident (1 case) [
Although Gardner-Wells traction should be acutely utilized to prevent further subluxation and increased neurological injury, circumferential surgical decompression/stabilization is the “gold standard.”
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akay KM, Ersahin Y, Tabur E. Cervical spondyloptosis: A case report. Minim Invasive Neurosurg. 2002. 45: 169-72
2. Jayakumar P, Choi D, Casey A. Late presentation of a Type III axis fracture with spondyloptosis. Ann R Coll Surg Engl. 2008. 90: W1-3
3. Manjila S, Chowdhry SA, Bambakidis NC, Hart DJ. Traumatic, high-cervical, coronal-plane spondyloptosis with unilateral vertebral artery occlusion: Treatment using a prophylactic arterial bypass graft, open reduction, and instrumented segmental fusion: Case report. J Neurosurg Spine. 2014. 20: 183-90
4. Muzumdar DP, Goel A. C2 over C3 spondyloptosis in a case with absent posterior elements. Report of an unusual case and analysis of treatment options. J Clin Neurosci. 2004. 11: 675-7
5. Singh PK, Agrawal M, Sawarkar D, Kumar A, Verma S, Doddamani R. Management of neglected complex hangman’s fracture by reforming the C2 pedicle: New innovative technique of motion preservation at the C1-2 joint in 2 cases. J Neurosurg Spine. 2020. 32: 1-8

