

- Department of Neurosurgery (Retired), University of California, Davis, Sacramento, California, United States.
DOI:10.25259/SNI-185-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Harry S. Goldsmith. Potential improvement of survival statistics for glioblastoma multiforme (WHO IV). 28-Jun-2019;10:123
How to cite this URL: Harry S. Goldsmith. Potential improvement of survival statistics for glioblastoma multiforme (WHO IV). 28-Jun-2019;10:123. Available from: http://surgicalneurologyint.com/surgicalint-articles/9435/
Date of Submission
10-Mar-2019
Date of Acceptance
11-May-2019
Date of Web Publication
28-Jun-2019
Abstract
The present-day treatment of a glioblastoma multiforme IV (glioblast) is by surgery, radiation, and chemotherapy. Unfortunately, the current treatment has not significantly improved the survival statistics of this tumor. There are now two relatively new surgical procedures that may improve the survival statistics of this malignancy. One of these procedures is the intraoperative use of the drug 5-aminovolumic acid (ALA), which fluoresces a red color in malignant brain tissue that is not observed in normal brain tissue. This allows a neurosurgeon to distinguish brain tissue infiltrated by malignant cells, thus allowing a more complete resection of the tumor. Another procedure that has the potential to improve the survival statistics of glioblasts is the use of the omentum. Direct placement of the omentum on a brain infiltrated by malignant cells would allow omental blood vessels, known to be completely clear of endothelial cells, to penetrate directly into the underlying brain. The blood flow through omental blood vessels could be expected to carry chemotherapeutic agents throughout the involved brain, thereby totally bypassing the blood–brain barrier. Combining a tumor resection using 5-ALA and placing the omentum on the brain may prove instrumental in improving the survival statistics of patients suffering from a glioblast.
Keywords: 5-Aminovolumic acid, Glioblastoma multiforme IV, Omentum
A glioblastoma multiforme IV is one of the most devastating tumors that occur in humans. Despite the current treatment of a glioblast by surgical excision, radiation therapy, and chemotherapy, it is estimated that patients with this condition will live only 1–2 years following the diagnosis and treatment with standard therapy. The National Brain Tumor Society stated that the survival statistic for a glioblast is 5.2%. The American Brain Tumor Association reported that 13,309 glioblast cases occurred in 2017, and the American Cancer Society has reported that in the 55–64-year-old age group, the age that most glioblasts occur, only 5% of this group would be alive at 5 years. The survival of these patients has improved only slightly since the time of Harvey Cushing’s surgical career (1899–1933). The question this raises is whether there can be a significant improvement at this time.
THERAPEUTIC STATUS
Neurosurgery
A glioblast is a highly malignant tumor with cells that can spread throughout the brain. The current forms of treatment include surgical removal of the primary tumor followed by postsurgical radiation and the subsequent administration of chemotherapy. The present-day neurosurgical treatment of a glioblast involves removing the maximum amount of malignant tumor tissue without involving critical areas of the brain that if resected would result in a serious postoperative neurological defect.
Radiation
Following surgical excision of a glioblast in which complete or incomplete removal of the tumor has been performed; the malignant tumor bed and surrounding brain areas receive conventional radiation therapy often in 30 treatments of radiation in a cumulative dosage of 60 gy. Additional radiation may be applied to other areas of the brain by directing multiple beams of radiation to specific brain locations; however, there is the possibility that additional radiation can be harmful to brain tissue. Furthermore, it does not appear that increased radiation therapy for a glioblast will have a significant influence on future survival statistics for this tumor.
Chemotherapy
If there is to be improvement in the poor statistics associated with a glioblast, it seems likely that chemotherapy will be a major factor in the treatment. The chemotherapeutic agents needed for effective destruction of malignant tumor cells will require easy access into brain tissue over an indefinite period of time.
The ultimate question is can the present-day treatment of a glioblast by surgery, radiation therapy, and chemotherapy be improved? There appears to be a possibility that this can be accomplished.
An Interventional proposal
The initial procedure over the years for the treatment of a glioblast has been the surgical removal of the primary tumor and as much as possible of infiltrating malignant tissue surrounding the primary tumor. Success of this procedure has been limited by tumor tissue present in, or adjacent to, a critical brain area, a problem that has remained unresolved.
A recent article suggested that “there does not presently appear to be surgical techniques that would increase patients’ survival rates following the excision of a primary glioblastoma WHO IV.”[
THERAPEUTIC SOLUTION
5-Aminovolumic acid (ALA)
One of the new procedures that have the potential to improve the progression-free period that follows the initial resection of glioblast is the intraoperative utilization of the drug 5-ALA. This drug was first described in 1983 and was approved for glioblast treatment by the FDA on July 3, 2017. Recently, the first 5-ALA fluorescence-guided brain tumor surgery symposium was held in the USA at the Mount Sinai Hospital in New York City on November 20, 2018.[
5-ALA, when administered 3 h before surgery for a glioblast, results in the fluorescence of malignant tissue within the brain. At the time of surgery, the drug causes a distinct red coloration in malignant brain tissue predominantly around the area of the primary tumor. The distinct red coloration loses its intensity at the site of a primary malignant tumor with the fluorescent red coloration decreasing to pink at the margin of the lesion. Fluorescence-guided surgery enables neurosurgeons to distinguish tissue infiltrated by malignant cells from normal brain tissue. The red and pink coloration of malignant tumor at the margin of a tumor resection allows for a more complete resection of malignant brain tissue. The visual distinction observed between normal and malignant tissue at the time of surgery can result in the surgical removal of a greater amount of malignant brain tissue than was previously possible. Fluorescence-guided surgery has made this achievable.
The amount of 5-ALA that is necessary for fluorescence has been proposed at a dosage level of 5, 10, and 20 mg/kg. The optimal dosage of the drug is presently being investigated by various studies which undoubtedly will be significant.
Omentum
A second new neurosurgical procedure that may improve the survival statistics of a glioblast is the use of the omentum. It has been shown over the past several decades that when an intact vascularized omental pedicle is placed directly on the brain of animals[
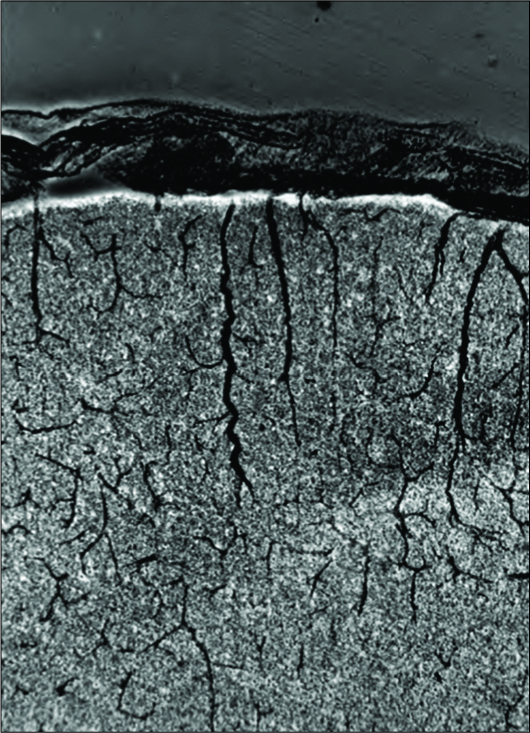
Figure 1:
India Ink given intravenously shows the dye in the omentum located on a monkey brain. Note the omental blood vessels delivering blood and India Ink into the depth of the underlying brain. It is expected that chemotherapeutic agents will also have the ability, when present in omental capillary blood flow, to deliver drugs to malignant cells distant from a primary glioma. Blood brain barrier vessels will not be necessary in the process.
Omental blood flow studies have shown that placing the omentum on the brain of humans allows for increased blood flow throughout the entire brain.[
CONCLUSION
Due to the BBB that limits the entrance of possible effective chemotherapeutic agents into the brain infiltrated by glioblast cells, there has been no appreciable improvement in the survival statistics of this tumor since the endeavor of Harvey Cushing over a century ago. Fluorescent-guided surgery now aides in identifying undetected malignant brain tissue that previously was not observed, an achievement that was impossible before the introduction of 5-ALA. The combination of 5-ALA and the placement of the omentum on the brain harboring glioblast cells may have the potential to improve the survival statistics of this tumor.
The ongoing surgical evaluation of 5-ALA combined with the use of the omentum in the treatment of a glioblast would appear to justify the undertaking of clinical trials pertaining to 5-ALA and the omentum in the possibility that these two factors may improve the future survival statistics of patients with a glioblastoma multiforme WHO IV.
References
1. Goldsmith HS. Blood brain barrier effect eliminated by omentum for the treatment of glioblastoma multiforme (WHO IV). EC Neurol. 2018. 10: 928-32
2. Goldsmith HS. Lack of atherosclerosis in omental arteries. Lancet. 1990. 335: 409-
3. Goldsmith HS, Duckett S, Chen WF. Prevention of cerebral infarction in the dog by intact omentum. Am J Surg. 1975. 130: 317-26
4. Goldsmith HS, Duckett S, Chen WF. Prevention of cerebral infarction in the monkey by omental transposition to the brain. Stroke. 1978. 147: 503-6
5. Goldsmith HS. Traumatic brain injury: Possible effect of omentum. J Syst Integr Neurosci. 2017. 3: 4-
6. Goldsmith HS, Bacciu P, Cossu M, Pau A, Rodriguez G, Rosadini G. Regional cerebral blood flow after omental transposition to the ischaemic brain in man. A five year follow-up study. Acta Neurochir (Wien). 1990. 106: 145-52
7. Goldsmith HS. A new approach to the treatment of alzheimer’s disease: The need for a controlled study. J Alzheimers Dis. 2011. 25: 209-12
8. Goldsmith HS. Benefit of omental blood flow in alzheimer’s disease: Effect on deteriorating neurons. J Alzheimers Dis. 2014. 42: S277-80
9. Goldsmith HS. Alzheimer disease can be treated: Why the delay?. Surg Neurol Int. 2017. 8: 133-8
10. Goldsmith HS. Omentum transposition for treatment of alzheimer’s disease in China. Chin Neurosurg. 2016. 2: 1-3
11. Goldsmith HS. Omental transplantation for stroke and TIA’s. J Neurosurg. 1987. 66: 152-3
12. Goldsmith HS. The evolution of omentum transposition: From lymphedema to spinal cord, stroke and alzheimer’s disease. Neurol Res. 2004. 26: 586-93
13. Goldsmith HS, Sax DS. Omental transposition for cerebral infarction: A 13-year follow-up study. Surg Neurol. 1999. 51: 342-5
14. Goldsmith HS, Saunders RL, Reeves AG, Allen CD, Milne J. Omental transposition to brain of stroke patients. Stroke. 1979. 10: 471-2
15. Goldsmith HS. Omental transposition for alzheimer’s disease. Neurol Res. 1996. 18: 103-8
16. Pardridge WM. The blood-brain barrier: Bottleneck in brain drug development. NeuroRx. 2005. 2: 3-14
17. Stummer W, Stocker S, Wagner S, Stepp H, Fritsch C, Goetz C. Intraoperative detection of malignant gliomas by 5-aminolevulinic acid-induced porphyrin fluorescence. Neurosurgery. 1998. 42: 518-25
18. Stummer W, Novotny A, Stepp H, Goetz C, Bise K, Reulen HJ. Fluorescence-guided resection of glioblastoma multiforme by using 5-aminolevulinic acid-induced porphyrins: A prospective study in 52 consecutive patients. J Neurosurg. 2000. 93: 1003-13
19. Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006. 7: 392-401
20. Stummer W, Reulen HJ, Meinel T, Pichlmeier U, Schumacher W, Tonn JC. Extent of resection and survival in glioblastoma multiforme: Identification of and adjustment for bias. Neurosurgery. 2008. 62: 564-76
21. Stummer W, Tonn JC, Mehdorn HM, Nestler U, Franz K, Goetz C. Counterbalancing risks and gains from extended resections in malignant glioma surgery: A supplemental analysis from the randomized 5-aminolevulinic acid glioma resection study. Clinical article. J Neurosurg. 2011. 114: 613-23
22. Stummer W, Tonn JC, Goetz C, Ullrich W, Stepp H, Bink A. 5-aminolevulinic acid-derived tumor fluorescence: The diagnostic accuracy of visible fluorescence qualities as corroborated by spectrometry and histology and postoperative imaging. Neurosurgery. 2014. 74: 310-9
23. Stummer W, Rodrigues F, Schucht P, Preuss M, Wiewrodt D, Nestler U. Predicting the “usefulness” of 5-ALA-derived tumor fluorescence for fluorescence-guided resections in pediatric brain tumors: A European survey. Acta Neurochir. 2014. 156: 2315-24

