

- Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, Old Rajinder Nagar, New Delhi, Delhi, India.
DOI:10.25259/SNI_61_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Manoj Kumar, Prem Bahadur Shahi, Nitin Adsul, Shankar Acharya, K. L. Kalra, R. S. Chahal. Progressive dysphagia and dysphonia secondary to DISH-related anterior cervical osteophytes: A case report. 18-Apr-2020;11:69
How to cite this URL: Manoj Kumar, Prem Bahadur Shahi, Nitin Adsul, Shankar Acharya, K. L. Kalra, R. S. Chahal. Progressive dysphagia and dysphonia secondary to DISH-related anterior cervical osteophytes: A case report. 18-Apr-2020;11:69. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9968
Date of Submission
14-Feb-2020
Date of Acceptance
19-Mar-2020
Date of Web Publication
18-Apr-2020
Abstract
Background: Dysphagia due to diffuse idiopathic skeletal hyperostosis (DISH)-related anterior cervical osteophytes is not uncommon. However, this rarely leads to dysphonia and/or dysphagia along with life- threatening airway obstruction requiring emergency tracheotomy.
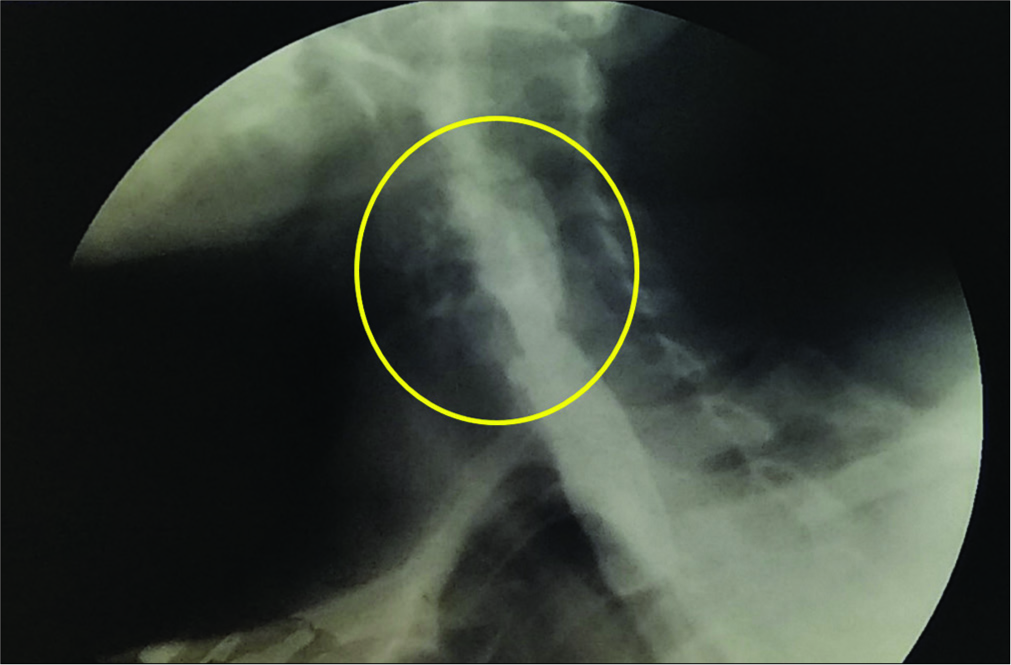
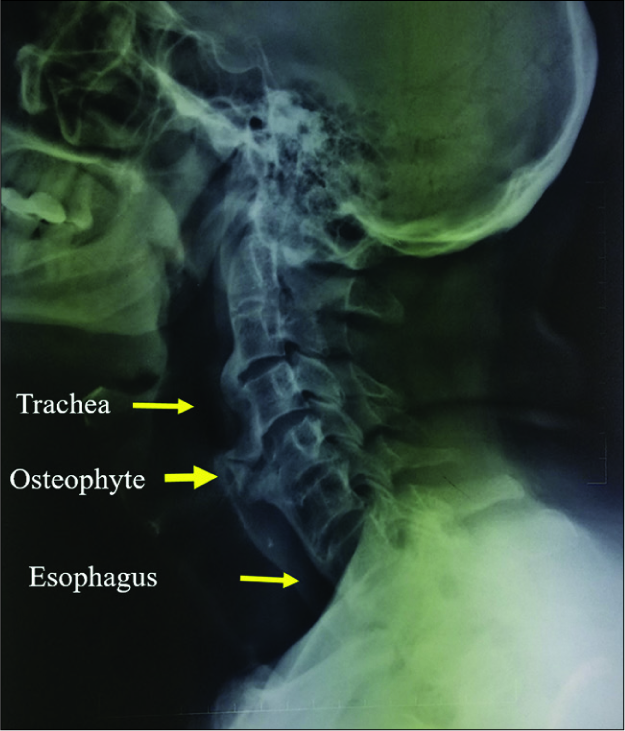
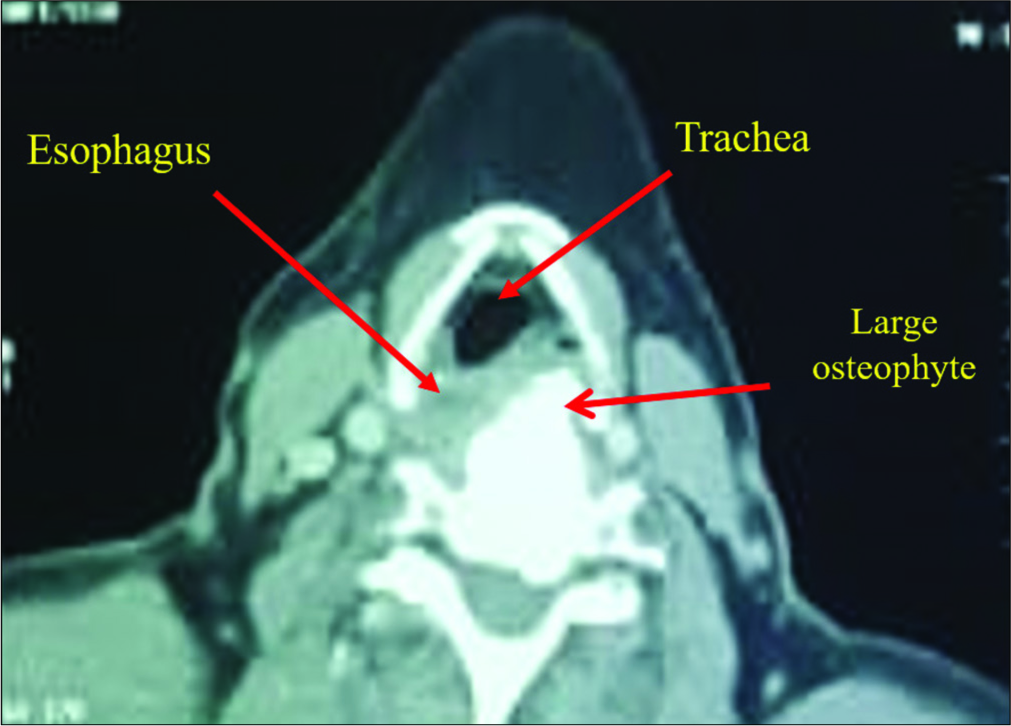
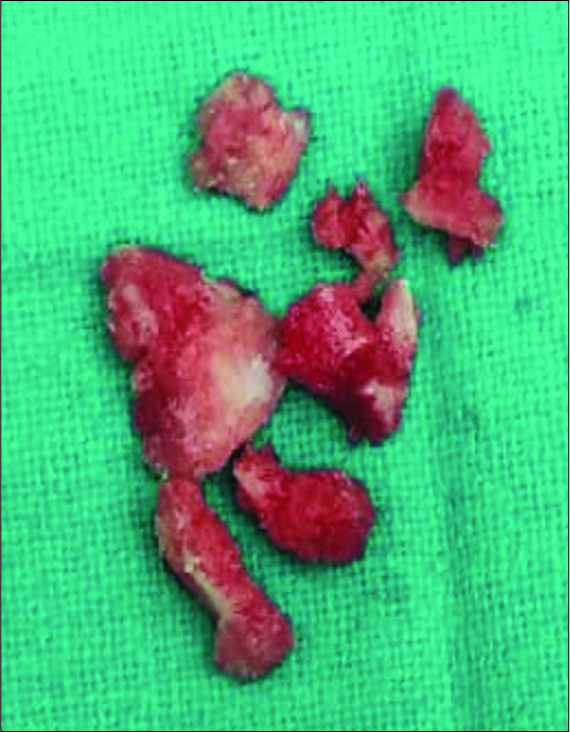
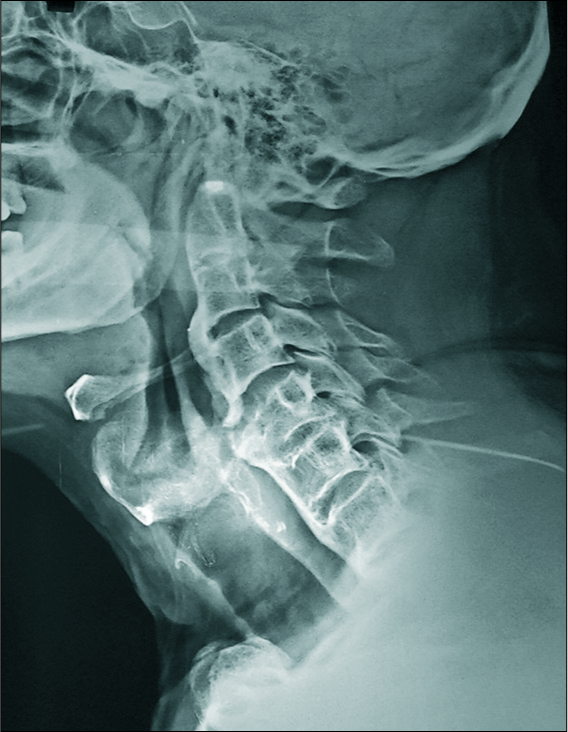
Case Description: A 56-year-old male presented with progressive dysphagia and dysphonia secondary to DISH-related anterior osteophytes at the C3–C4 and C4–C5 levels. The barium swallow, X-ray, magnetic resonance imaging, and computed tomography scans confirmed the presence of DISH. Utilizing an anterior cervical approach, a large beak-like osteophyte was successfully removed, while preserving the anterior annulus. After clinic-radiological improvement, the patient was discharged with a soft cervical collar and nonsteroidal anti-inflammatory drug (NSAID).
Conclusion: Large anterior osteophytes in Forestier disease/DISH may cause dysphagia and dysphonia. Direct anterior resection of these lesions yields excellent results as long as other etiologies for such symptoms have been ruled out.
Keywords: Anterior cervical osteophyte, Diffuse idiopathic skeletal hyperostosis, Dysphagia, Dysphonia
INTRODUCTION
Diffuse idiopathic skeletal hyperostosis also known as Forestier’s disease is a common degenerative enthesopathic disorder of unknown etiology. It is characterized by ossification of the longitudinal ligaments, especially the anterior longitudinal ligaments (ALL) in the spine.[
In this case, a 56-year-old male presented with a large symptomatic anterior osteophyte/DISH lesion at the C4–C5 level causing progressive dysphagia and dysphonia.
CASE REPORT
A 56-year-old male presented with the 1-year onset of progressive dysphagia and 8 months of dysphonia. Notably, his neurological examination was intact. The barium swallow showed a narrowed esophageal lumen at the C4–C5 level [
DISCUSSION
Dysphagia due to anterior cervical osteophytes is rare.[
Imaging of DISH to rule out other causes of dysphagia/ dysphonia
Besides preoperative images (e.g., X-ray, computed tomography, and magnetic resonance imaging), esophageal and laryngoscopic examinations combined with fluoroscopic barium swallowing tests are essential to both establish the diagnosis of DISH contributing to dysphagia/dysphonia and to provide a clear guide for treatment.
Surgery
Patients who fail conservative measures typically become surgical candidates. Surgery should consist of direct anterior removal of osteophytes/DISH, with preservation of the anterior annulus.[
Recurrence of DISH
Recurrence of cervical DISH is rare, but may develop slowly and progressively at the average rate of 1 mm/year. In addition, it may be associated with segmental instability at the index operated level.[
Role of nonsteroidal anti-inflammatory drugs (NSAIDs)
After total hip replacement, NSAIDs are typically utilized postoperatively to prevent the recurrence of DISH osteophytes. However, the utility of NSAIDs following cervical spine surgery for DISH is not as well understood. Ruetten et al. recommend the postoperative use of indomethacin 50 mg twice daily for 10 days with gastric protection, plus fractionated radiation with five doses of 2 Gray (4 days interval) if not contraindicated with patients over 55 years of age.
Postoperative bracing
The postoperative use of a soft cervical collar for 6 weeks combined with speech therapy was found to improve clinical outcomes in some patients undergoing anterior cervical DISH surgery. The role of bisphosphonate etidronate disodium in the prevention of ligament ossification/DISH in animal tests has not yet become standard in humans.[
CONCLUSION
Large cervical anterior osteophytes in Forestier disease (DISH) rarely cause dysphagia and dysphonia. Here, direct surgical resection of the anterior osteophytes/DISH produced an excellent result.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Forestier J, Rotes-Querol J. Senile ankylosing hyperostosis of the spine. Ann Rheum Dis. 1950. 9: 321-30
2. Lee DU, Ko HC, Son BC. Extensive heterotopic ossification following anterior cervical fusion in a patient with diffuse idiopathic skeletal hyperostosis. Nerve. 2018. 4: 12-5
3. Nicolas H, Voelker A, Jarvers JS, Gulow J, Heyde CE. Results after the surgical treatment of anterior cervical hyperostosis causing dysphagia. Eur Spine J. 2015. 24: 489-93
4. Psychogios G, Jering M, Zenk J. Cervical hyperostosis leading to dyspnea, aspiration and dysphagia: Strategies to improve patient management. Front Surg. 2018. 5: 33-
5. Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology. 1976. 119: 559-68
6. Ruetten S, Baraliakos X, Godolias G, Komp M. Surgical treatment of anterior cervical osteophytes causing dysphagia. J Orthop Surg (Hong Kong). 2019. 27: 2309499019837424-
7. Sardana H, Rai HI, Kumar A, Agrawal D, Kale S. Dysphagia, dysphonia and dyspnoe caused by ostrich beak-like anterior C1-C2 cervical osteophyte. Interdisciplinary Neurosurg. 2019. 16: 132-4
8. Yamamoto K, Imakiire A, Shishido T, Masaoka T. Effects of ethane-1-hydroxy-1,1-diphosphonate on ossification of the posterior longitudinal ligament in Zucker fatty rats. J Orthop Surg (Hong Kong). 2004. 12: 45-54

