

- Department of Neurosurgery, Louisiana State University Health Sciences Center Shreveport, LA, USA
- Department of Biometry, Louisiana State University Health Sciences Center Shreveport, LA, USA
Correspondence Address:
R. Menger
Department of Neurosurgery, Louisiana State University Health Sciences Center Shreveport, LA, USA
DOI:10.4103/2152-7806.156632
Copyright: © 2015 Menger R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Menger R, Connor D, Hefner M, Caldito G, Nanda A. Pseudomeningocele formation following chiari decompression: 19-year retrospective review of predisposing and prognostic factors. Surg Neurol Int 07-May-2015;6:70
How to cite this URL: Menger R, Connor D, Hefner M, Caldito G, Nanda A. Pseudomeningocele formation following chiari decompression: 19-year retrospective review of predisposing and prognostic factors. Surg Neurol Int 07-May-2015;6:70. Available from: http://surgicalneurologyint.com/surgicalint_articles/pseudomeningocele-formation-following-chiari-decompression/
Abstract
Background:Pseudomeningocele is a known operative complication of Chiari decompression with significant morbidity.
Methods:A retrospective analysis of 150 consecutive patients from November 1991 to June 2011 was conducted. Symptomatic pseudomeningocele was defined clinically; to meet definition it must have required operative intervention. Variables evaluated included sex, age, use of graft, and use of operative sealant. The Chi-square, Fisher test, and the two-sample t-test were used as appropriate to determine significance. Multiple logistic regression was used to determine independent risk factors for complication.
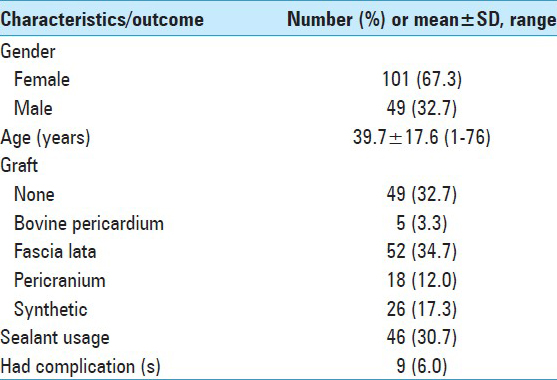
Results:A total of 67.3% of patients were female, with average age being 39.7 years. A total of 67.3% of patients had a graft placed with the most common being fascia lata. Only nine patients (6%) presented with pseudomeningocele. Factors observed to be significantly associated with pseudomeningocele development were age and use of sealant. Age and sealant use were also independent risk factors for complication. Adjusted for the significant effect of age, odds for complication among patients with sealant usage were 6.67 times those for patients without sealant. Adjusted for the significance of sealant usage, there is a 6% increase in odds for complication for every year increase in patient's age.
Conclusions:A statistically significant relationship exists between age and sealant use and the risk of developing a postoperative pseudomeningocele. Emphasis and attention must be placed on meticulous closure technique. This information can aide in preoperative planning and patient selection.
Keywords: Arnold-Chiari malformation, operative complications, operative sealant, pseudomeningocele
INTRODUCTION
Chiari malformations represent a broad group of craniovertebral anomalies in which patients may present in a spectrum of different clinical scenarios.[
The most clinically volatile complication of Chiari decompression is the pseudomeningocele.[
Primary closure techniques vary significantly from center to center and can involve many possible permutations of auto- or allograft and sealant.[
The current investigation reviews the long-term trends in complications following Chiari decompression at a large, academic teaching hospital.
MATERIALS AND METHODS
Review Protocol was approved by the Institutional Review Board. A retrospective analysis of patient charts, operative records, and radiology reports was performed upon consecutive patients undergoing operative intervention for Chiari malformation at our institution from April 1991 to June 2011. This was performed using the historical database available for all surgical patients created by the Department of Neurosurgery. Patient characteristics collected and recorded included age, sex, race, diagnosis, surgical treatment, including use of graft or operative sealant, date of admission, and imaging characteristics.
The information was extracted by the same chart reviewer using an electronic database as well as the electronic chart system. Inclusion criteria included patients undergoing a first time decompression via sub-occipital craniectomy for Chiari malformation. Furthermore, this was limited to type I Chiari malformations as linked with the admission or surgical diagnosis. Focus was on pseudomeningocele that was both symptomatic and operative. Again, this implies that the pseudomeningocele had to be identified clinically and radiographically; it also had to result in an operative intervention. Other complications were not considered in the aim of this study.
Data on 150 patients were analyzed to determine factors significantly associated with complication. The Chi-square or Fisher test was used to determine significant categorical factors, and the two-sample t-test was used to determine association of age with complications. Multiple logistic regression was used to determine independent risk factors for complication.
Operative procedure
Surgical goals for Chiari decompression include decompression of the inferior cerebellum, enlargement of the posterior fossa, and the establishment of CSF flow.[
RESULTS
A total of 150 patient met inclusion criteria. Demographic information, operative variables, and incidence of complications are included in [
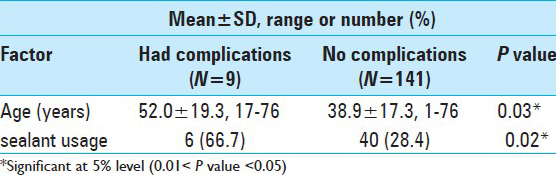
Only nine patients (6.0%) experienced an operative pseudomeningocele. The factors observed to be significantly associated with having an operative pseudomeningocele were age and utilization of operative sealant during closure. Comparisons between patients with and without complications are shown in [
Following multiple logistic regression analysis, age and usage of operative sealant were determined to be independent risk factors for complication [

DISCUSSION
The pathophysiology of Chiari malformation, as well as the most appropriate management of its myriad symptoms has vexed physicians for centuries. Among the first documented observations were made by Realdo Colombo in 1572, when he described the syndrome of atlas assimilation.[
Incidence of operative pseudomeningocele
From the beginning of operative intervention for Chiari malformation, surgical morbidity has been high. Contemporary rates have significantly diminished from historical rates as high as 100%. Overall, the 6% rate of symptomatic, operative pseudomeningocele demonstrated in this series compares favorably with published rates. In 2012, Klekamp et al. reported a 5.9% rate of CSF fistula in 371 consecutive decompressions with duraplasty,[
Patient age
Increasing patient age was found to be significantly associated with increasing rates of complication. Intuitively, age is seen as risk factor for developing a pseudomeningocele, as it has been well established as a predictor of operative morbidity and mortality in multiple series.[
Operative sealant
Additionally, the use of any sealant, without respect to type, increased the chances of operative pseudomeningocele in this series. It is likely surgeons are more likely to use sealant in the face of a possible complicated closure. Than et al. performed a direct comparison between fibrin-based and polyethylene glycol (PEG) sealant augmented dural closure in 100 consecutive posterior fossa surgeries and found a significantly higher rate of incisional CSF leak in the former group.[
Graft selection
While the current series did not find any correlation or statistically significant difference in outcome based upon the selection of dural graft, the literature is replete with case series purporting the superiority of autologous, synthetic, or xenographic materials.[
In a retrospective review of their pediatric experience, Attenello et al. published a radiographic and clinical outcome comparison between autologous pericranial and an “antiadhesive” ePTFE dural substitute graft.[
Most recently, in 2013, Williams et al. published a prospective, randomized comparison of sutureless synthetic duraplasty with a watertight closure with bovine pericardium grafting, without the use of operative sealant in either case.[
The preponderance of contradictory data regarding choice of dural graft and its effect on postoperative complications seems to suggest that the factors likely responsible for poor outcomes are more surgeon and technique-driven. The creation of a watertight duraplasty and proper, layered closure of the operative incision probably contribute significantly to the overall outcome more so than the specific choice of material for implantation. Of course the corollary of this argument also holds true: no amount of technological advancement will even overcome the effects of a nonmeticulous surgical closure.
Limitations
This investigation is limited by several factors inherent to its retrospective design. Information regarding specific operative technique not listed in the operative note was unavailable. This included but was not limited to type or technique of stitch used, level of training for surgeon closing the wound, and the reason regarding the type of graft used. Specific information regarding the opening of the arachnoid membrane, a known risk factor for pseudeomeningocele formation, in duroplasty cases was also not available. The decision-making process regarding when to use sealant was also unavailable. While standard operating technique at our facility would dictate a Valsalva maneuver following completion of the duraplasty, if these results were not noted in the operative report, they were unavailable for analysis. This includes whether or not the dura was fully opened. Additionally, data regarding the selection of graft material selection was not available in 49 patients. As a result, we were unable to accurately compare this variable over the 20-year study period. The effect of graft selection on outcome following posterior fossa decompression needs to be further evaluated and investigated in future study.
Furthermore, this study defined a complication as a symptomatic and operative pseudomeningocele. Size, presence of a transcutaneous fistula, or attending's treatment algorithm for pseudomeningocele treatment was not available. While this complication has been shown to significantly reduce the immediate efficacy of decompression and diminish overall improvement in health at one year, the data presented here does not capture the incidence and outcome of symptomatic pseudomeningoceles treated conservatively with either placement of a lumbar drain or needle decompression followed by a tight head wrap.[
CONCLUSION
This investigation is the first to establish a statistically significant relationship between the risk of developing of a postoperative pseudomeningocele following posterior fossa decompression and increasing patient age as well as use of operative sealant. This data can aide surgeons in risk stratification and preoperative planning prior to performing these procedures. Focus is on operative technique. We believe that these results emphasize the importance, not only of meticulous attention to detail when performing the duraplasty, but also flexibility in technique allowing for alternate choices in dural substitute or operative sealant as the individual case may dictate.
The modern era of Chiari surgery was ushered in by Bernard Williams, the first neurosurgeon to intensively deal with the pathology of Chiari I malformation.
At the end of his prematurely interrupted life, he wrote an editorial advocating for leaving the dura open at the end of Chiari decompressions.[
In his opinion, leaving behind an iatrogenic pseudomeningocele was more acceptable than dealing with the mass effect of a pseudomeningocele caused by the ball valve mechanisms of an imperfectly closed duraplasty.
This article caused a schism in the Chiari surgical technique, which still endures today, between the American lore of closing the dura with a duraplasty and the British tradition of deference to the parting words of Mr. Williams.
In the following years, Ulrich Batzdorf M.D., Arnold Menezes M.D., and Thomas Milhorat M.D., demonstrated that through repetition, improvement, and impeccable technique, the incidence of pseudomeningocele could be contained to values below 5%.[
Years later, the pseudomeningocele is still the defining complication in the field of Chiari surgery.[
Pseudomeningoceles can negatively affect the patient via a number of different mechanisms: (i) mass effect on the duraplasty and the dural contents; (ii) aseptic meningitis; (iii) negative effects on cerebrospinal fluid (CSF) flow and pressure; and (iv) transcutaneous fistulas (with consequent bacterial meningitis).
Patients with a history of large postoperative pseudomeningoceles are often the recipients of subsequent ventriculo-peritoneal shunts, in the face of elevated CSF pressures.
The real overall incidence of pseudomeningoceles is probably underestimated, since many Neurosurgeons spring to corrective surgical action only in the case of transcutaneous CSF fistulae. Moreover, a number of Neurosurgeons tend to “accept” the chronic presence of nonexpanding pseudomeningoceles, as a part of the normal spectrum of postoperative surgical results.
The concepts of “failed Chiari surgery” and of “posterior fossa revision” are quite recent and have gained traction thanks to the birth of Centers dedicated to the diagnosis and management of Chiari I malformation. Persistent pseudomeningoceles are increasingly recognized as one of the causes for “failed Chiari surgery” in quite a large number of patients.
Running locked, running unlocked, and interrupted stitching configurations have been used in Chiari surgery, with similar results in the best of hands. Flawless execution is the only determining factor for successfully avoiding pseudomeningoceles, in the face of different needles and stitching materials used.
The dura of Chiari patients has several unique, challenging features. It is extremely thin over the cerebellar hemispheres (at the very top of the Y-shaped dural incision), because of the combined effects of a small posterior fossa and a pulsatile, crowded cerebellum. It is also very adherent to the periosteum at the level of the foramen magnum. Dural rents or shredding of the outer dural layer during the craniectomy can increase the chance of a postoperative pseudomeningocele.
The mismatch between a thin, fragile dura and a stiff, thick duraplasty (i.e., bovine pericardium, GoreTex) can create undue tension at the dural edge of the durarraphy, with leaking stitch-holes.
Watertight closure is to be tested with Valsalva maneuvers. As a rule, one or two Valsalva maneuvers are not enough. Attention should be paid to the air–fluid level (often visible through the thinned and transparent dura), being sure that the entire height of the durarraphy is below such level, to guarantee reliable Valsalva testing. We routinely fill the subdural space with 20–40 cc of injectable saline before passing the last dural stitch, to improve the odds.
Dural sealants have been engineered to prevent pseudomeningoceles.[
In the posterior fossa, gravity tends to bring the CSF through the dural stitching (and not away from it like in the supratentorial compartment).
Dural sealants cannot and should not be regarded as a magical remedy or a compensation to less than meticulous dural suturing.
Extradural techniques of Chiari decompression have been advocated to try to avoid pseudomeningoceles altogether.[
Our preoccupation is that the new generations of Residents, tempted by the availability of sealants and extradural techniques, could end up becoming less proficient in the fine art of a watertight dural closure of the posterior fossa.
Dr. Liu and his colleagues have recently combined a subpial tonsillar resection along with a primary durarraphy (i.e., without a duraplasty). Using a variant of this technique, we were able to perform more than 250 cases without a single instance of pseudomeningocele, exploiting the finding that the Chiari dura is at its thickest along the midline.
ACKNOWLEDGMENTS/DISCLOSURE
Dr. Anil Nanda is Professor and Chairman, Department of Neurosurgery at LSU Health Sciences Center in Shreveport, LA.
Neither Dr. Nanda nor any of the authors of this investigation has received anything of value from or owns stock in a commercial company or institution related directly or indirectly to the subject of this article.
A significant portion of this work was presented as an oral presentation at the Multidisciplinary Oral Presentations Section of the Original Science Program at the 2012 Congress of Neurological Surgeons Annual Meeting, October 6-10, in Chicago, Illinois.
Commentary
- Department of Neurosurgery, North Shore University Hospital at Manhasset, NY, USA. E-mail:
pbolognese@nspc.com
References
1. Abla AA, Link T, Fusco D, Wilson DA, Sonntag VK. Comparison of dural grafts in Chiari decompression surgery: Review of the literature. J Craniovertebral Junction Spine. 2010. 1: 29-37
2. Ackermann JF. über die Kretinen, eine besondere Menschenabart in den Alpen. ed, Gotha. 1790. p.
3. Attenello FJ, McGirt MJ, Garcés-Ambrossi GL, Chaichana KL, Carson B, Jallo GI. Suboccipital decompression for Chiari I malformation: Outcome comparison of duraplasty with expanded polytetrafluoroethylene dural substitute versus pericranial autograft. Childs Nerv Syst. 2009. 25: 183-90
4. Barkovich AJ, Wippold FJ, Sherman JL, Citrin CM. Significance of cerebellar tonsillar position on MR. AJNR Am J Neuroradiol. 1986. 7: 795-9
5. Bejjani GK. Definition of the adult Chiari malformation: A brief historical overview. Neurosurg Focus. 2011. 11: E1-
6. Chaichana KL, Pendleton C, Jackson C, Martinez-Gutierrez JC, Diaz-Stransky A, Aguayo J. Deep venous thrombosis and pulmonary embolisms in adult patients undergoing craniotomy for brain tumors. Neurol Res. 2013. 35: 206-11
7. Chauvet D, Tran V, Mutlu G, George B, Allain JM. Study of dural suture watertightness: An in vitro comparison of different sealants. Acta Neurochir (Wien). 2011. 153: 2465-72
8. Chiari H. Concerning alterations in the cerebellum resulting from cerebral hydrocephalus. 1891. Pediatr Neurosci. 1987. 13: 3-8
9. Danish SF, Samdani A, Hanna A, Storm P, Sutton L. Experience with acellular human dura and bovine collagen matrix for duraplasty after posterior fossa decompression for Chiari malformations. J Neurosurg. 2006. 104: 16-20
10. Elia C, Schoenfeld C, Bayer O, Ewald C, Reinhart K, Sakr Y. The impact of age on outcome after major surgical procedures. J Crit Care. 2013. 28: 413-20
11. Foreman P, Safavi-Abbasi S, Talley MC, Boeckman L, Mapstone TB. Perioperative outcomes and complications associated with allogeneic duraplasty for the management of Chiari malformations Type I in 48 pediatric patients. J Neurosurg Pediatr. 2012. 10: 142-9
12. Guo F, Wang M, Long J, Wang H, Sun H, Yang B. Surgical management of Chiari malformation: Analysis of 128 cases. Pediatr Neurosurg. 2007. 43: 375-81
13. Hoffman CE, Souweidane MM. Cerebrospinal fluid-related complications with autologous duraplasty and arachnoid sparing in type I Chiari malformation. Neurosurgery. 2008. 62: 156-60
14. Ito K, Horiuchi T, Oyanagi K, Nomiyama T, Hongo K. Comparative study of fibrin and chemical synthetic sealant on dural regeneration and brain damage. J Neurosurg Spine. 2013. 19: 736-43
15. Klekamp J. Surgical treatment of Chiari I malformation--analysis of intraoperative findings, complications, and outcome for 371 foramen magnum decompressions. Neurosurgery. 2012. 71: 365-80
16. Lam FC, Penumaka A, Chen CC, Fischer EG, Kasper EM. Fibrin sealant augmentation with autologous pericranium for duraplasty after suboccipital decompression in Chiari 1 patients: A case series. Surg Neurol Int. 2013. 4: 6-
17. Levy WJ, Mason L, Hahn JF. Chiari malformation presenting in adults: A surgical experience in 127 cases. Neurosurgery. 1983. 12: 377-90
18. Litvack ZN, West GA, Delashaw JB, Burchiel KJ, Anderson VC. Dural augmentation: part I-evaluation of collagen matrix allografts for dural defect after craniotomy. Neurosurgery. 2009. 65: 890-7
19. Parízek J, Mĕricka P, Husek Z. Detailed evaluation of 2959 allogeneic and xenogeneic dense connective tissue grafts (fascia lata, pericardium, and dura mater) used in the course of 20 years for duraplasty in neurosurgery. Acta Neurochir (Wien). 1997. 139: 827-38
20. Malliti M, Page P, Gury C, Chomette E, Nataf F, Roux FX. Comparison of deep wound infection rates using a synthetic dural substitute (neuro-patch) or pericranium graft for dural closure: A clinical review of 1 year. Neurosurgery. 2004. 54: 599-603
21. Markunas CA, Tubbs RS, Moftakhar R, Ashley-Koch AE, Gregory SG, Oakes WJ. Clinical, radiological, and genetic similarities between patients with Chiari Type I and Type 0 malformations. J Neurosurg Pediatr. 2012. 9: 372-8
22. Milhorat TH, Bolognese PA, Nishikawa M, McDonnell NB, Francomano CA. Syndrome of occipitoatlantoaxial hypermobility, cranial settling, and chiari malformation type I in patients with hereditary disorders of connective tissue. J Neurosurg Spine. 2007. 7: 601-9
23. Mutchnick IS, Janjua RM, Moeller K, Moriarty TM. Decompression of Chiari malformation with and without duraplasty: Morbidity versus recurrence. J Neurosurg Pediatr. 2010. 5: 474-8
24. Park TS, Hoffman HJ, Hendrick EB, Humphreys RP. Experience with surgical decompression of the Arnold-Chiari malformation in young infants with myelomeningocele. Neurosurgery. 1983. 13: 147-52
25. Parker SL, Godil SS, Zuckerman SL, Mendenhall SK, Tulipan NB, McGirt MJ. Effect of symptomatic pseudomeningocele on improvement in pain, disability, and quality of life following suboccipital decompression for adult Chiari malformation Type I. J Neurosurg. 2013. 119: 1159-65
26. Parker SL, Godil SS, Zuckerman SL, Mendenhall SK, Wells JA, Shau DN. Comprehensive assessment of 1-year outcomes and determination of minimum clinically important difference in pain, disability, and quality of life after suboccipital decompression for Chiari malformation I in adults. Neurosurgery. 2013. 73: 569-81
27. Parker SR, Harris P, Cummings TJ, George T, Fuchs H, Grant G. Complications following decompression of Chiari malformation Type I in children: Dural graft or sealant?. J Neurosurg Pediatr. 2011. 8: 177-83
28. Paul KS, Lye RH, Strang FA, Dutton J. Arnold-Chiari malformation. Review of 71 cases. J Neurosurg. 1983. 58: 183-7
29. Pearce JM. Arnold chiari, or “Cruveilhier cleland Chiari” malformation. J Neurol Neurosurg Psychiatry. 2000. 68: 13-
30. Weeks A, Fallah A, Rutka J, Rengachary RG.editors. Posterior Fossa and Brainstem Tumors in Children. Principles of Neurosurgery. Philadelphia: Elsevier; 2012. p. 169-85
31. Rosen DS, Wollman R, Frim DM. Recurrence of symptoms after Chiari decompression and duraplasty with nonautologous graft material. Pediatr Neurosurg. 2003. 38: 186-90
32. Santamarta D, Blázquez JA, Maillo A, Muñoz A, Caballero M, Morales F. Analysis of cerebrospinal fluid related complications (hydrocephalus, fistula, pseudomeningocele and infection) following surgery for posterior fossa tumors. Neurocir Astur Spain. 2003. 14: 117-26
33. Scheich M, Ginzkey C, Mlynski R. Postoperative Complications After Surgery for Vestibular Schwannoma via the MCF Approach. Laryngorhinootologie. 2013. 92: 823-7
34. Schijman E. History, anatomic forms, and pathogenesis of Chiari I malformations. Childs Nerv Syst. 2004. 20: 323-8
35. Siasios J, Kapsalaki EZ, Fountas KN. Surgical Management of Patients with Chiari I Malformation. Int J Pediatr 2012. 2012. p.
36. Stevens EA, Powers AK, Sweasey TA, Tatter SB, Ojemann RG. Simplified harvest of autologous pericranium for duraplasty in Chiari malformation Type I. Technical note. J Neurosurg Spine. 2009. 11: 80-3
37. Than KD, Baird CJ, Olivi A. Polyethylene glycol hydrogel dural sealant may reduce incisional cerebrospinal fluid leak after posterior fossa surgery. Neurosurgery. 2008. 63: ONS182-6
38. Tubbs RS, Beckman J, Naftel RP, Chern JJ, Wellons JC, Rozzelle CJ. Institutional experience with 500 cases of surgically treated pediatric Chiari malformation Type I. J Neurosurg Pediatr. 2011. 7: 248-56
39. Vanaclocha V, Saiz-Sapena N. Duraplasty with freeze-dried cadaveric dura versus occipital pericranium for Chiari type I malformation: Comparative study. Acta Neurochir (Wien). 1997. 139: 112-9
40. Wang MC, Shivakoti M, Sparapani RA, Guo C, Laud PW, Nattinger AB. Thirty-day readmissions after elective spine surgery for degenerative conditions among US Medicare beneficiaries. Spine J Off J North Am Spine Soc. 2012. 12: 902-11
41. Williams LE, Vannemreddy PS, Watson KS, Slavin KV. The need in dural graft suturing in Chiari I malformation decompression: A prospective, single-blind, randomized trial comparing sutured and sutureless duraplasty materials. Surg Neurol Int. 2013. 4: 26-
42. Batzdorf U, McArthur DL, Bentson JR. Surgical treatment of Chiari malformation with and without syringomyelia: Experience with 177 adult patients. J Neurosurg. 2013. 118: 232-42
43. Hoffman CE, Souweidane MM. Cerebrospinal fluid-related complications with autologous duraplasty and arachnoid sparing in type I Chiari malformation. Neurosurgery. 2008. 62: 156-60
44. Mutchnick IS, Janjua RM, Moeller K, Moriarty TM. Decompression of Chiari malformation with and without duraplasty: Morbidity versus recurrence. J Neurosurg Pediatr. 2010. 5: 474-8
45. Parker SR, Harris P, Cummings TJ, George T, Fuchs H, Grant G. Complications following decompression of Chiari malformation Type I in children: Dural graft or sealant?. J Neurosurg Pediatr. 2011. 8: 177-83
46. Williams B. A blast against grafts-on the closing and grafting of the posterior fossa dura. Br J Neurosurg. 1994. 8: 275-8
47. Williams LE, Vannemreddy PS, Watson KS, Slavin KV. The need in dural graft suturing in Chiari I malformation decompression: A prospective, single-blind, randomized trial comparing sutured and sutureless duraplasty materials. Surg Neurol Int. 2013. 4: 26-

