

- Department of Spine Surgery, Hospital Universitario Fundación Santa Fe de Bogotá, Bogotá, Colombia.
Correspondence Address:
Omar Marroquín Herrera, Department of Spine Surgery, Hospital Universitario Fundación Santa Fe de Bogotá, Bogotá, Colombia.
DOI:10.25259/SNI_817_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Fernando Alvarado Gomez, Omar Marroquín Herrera, Jorge L. Villán Gaona, Carlos A. Fuentes Reyes, Martha L. Caicedo Gutiérrez, Luis C. Morales Saenz. Pulmonary cement embolism following transpedicular screws placement for thoracolumbar fractures. 30-Sep-2021;12:495
How to cite this URL: Fernando Alvarado Gomez, Omar Marroquín Herrera, Jorge L. Villán Gaona, Carlos A. Fuentes Reyes, Martha L. Caicedo Gutiérrez, Luis C. Morales Saenz. Pulmonary cement embolism following transpedicular screws placement for thoracolumbar fractures. 30-Sep-2021;12:495. Available from: https://surgicalneurologyint.com/surgicalint-articles/11132/
Date of Submission
15-Aug-2021
Date of Acceptance
25-Aug-2021
Date of Web Publication
30-Sep-2021
Abstract
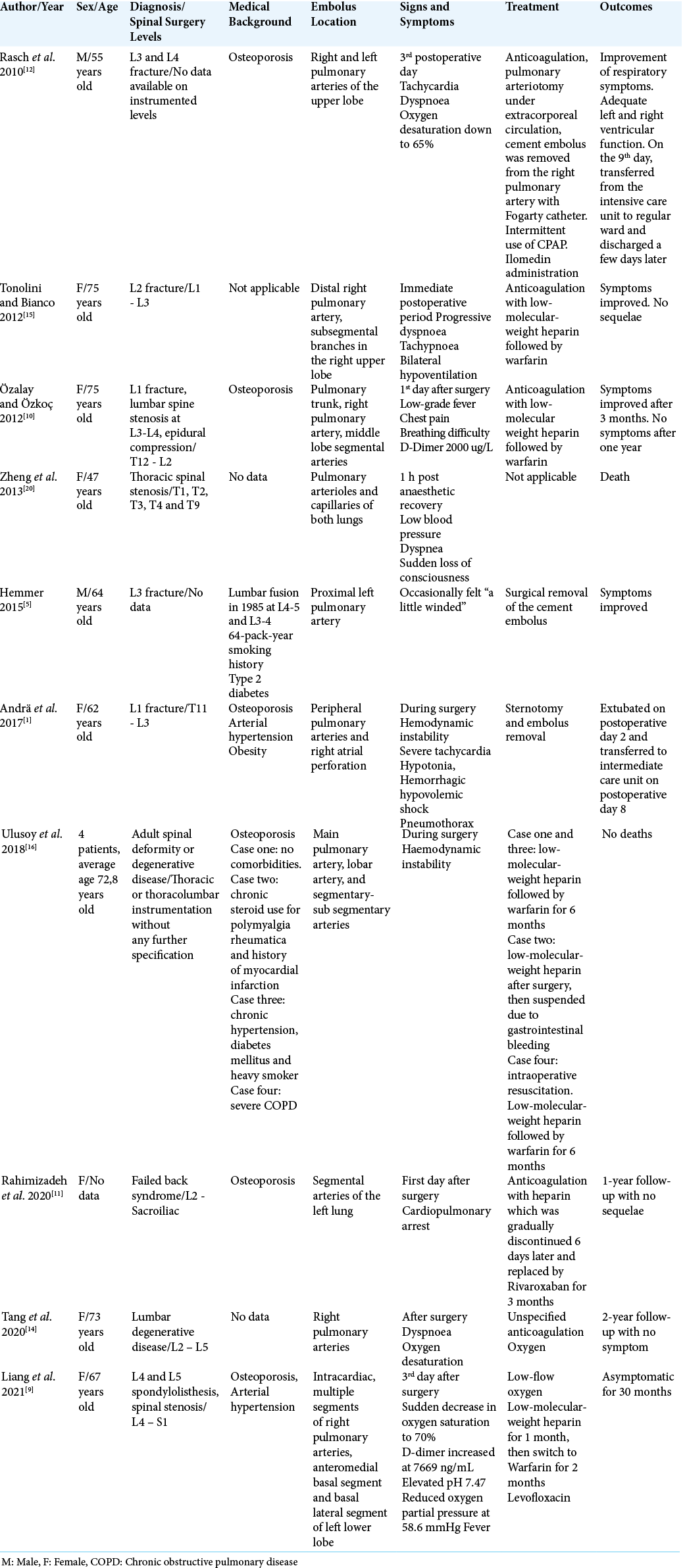
Background: Symptomatic pulmonary cement embolism in patients undergoing thoracic transpedicular fenestrated screw placement is rare. Here, we have added a 64-year-old female undergoing transpedicular screw placement for a T11 fracture who developed a pulmonary cement embolism intraoperatively and add this case to 13 others identified in the literature.
Case Description: A 64-year-old female presented with a type “C”, ASIA “E” T11 fracture. The thoracolumbar pedicle screw fixation was supplemented with bone cement due to her underlying severe osteoporosis. During the fluoroscopy-guided supplementation with bone cement, a leak through the paravertebral venous system was noted. Thirty minutes later, the patient acutely developed extreme respiratory failure and required mechanical ventilation for the next 2 days. The diagnosis of pulmonary embolism due to bone cement was confirmed on a contrast computed tomography study of the chest.
Conclusion: Symptomatic pulmonary cement embolization supplementing transpedicular screws placement for osteoporotic bone is rare. Here, we present a 64-year-old female who during transpedicular fixation of a T11 fracture developed an acute pulmonary embolism from the bone cement resulting in the need for 2 days of postoperative artificial ventilation.
Keywords: Fenestrated transpedicular screws, Polymethylmethacrylate, Pulmonary embolism, Thoracolumbar fracture
INTRODUCTION
Polymethylmethacrylate (PMMA) bone cement improves immediate stability and increases pullout resistance from 173% to 244% for patients with osteoporosis undergoing thoracic fracture transpedicular fixation.[
Potential locations of bone cement leakage include perivertebral, disc intracanalicular, foraminal, local perivertebral venous system cement leakage, and critically, as in this case, leakage to the central vascular system with migration to the cardiac or pulmonary system with risk of pulmonary embolism (2.1–26%).[
The presence of pulmonary embolism correlates with instrumentation of >7 levels.[
CASE REPORT
A 64-year-old female with osteoporosis, presented with a non-penetrating T11 traumatic spinal injury as a result of falling backwards downstairs. The computed tomography (CT) scan showed a T11, AO spine C classification, without a neurological deficit, ASIA – E [
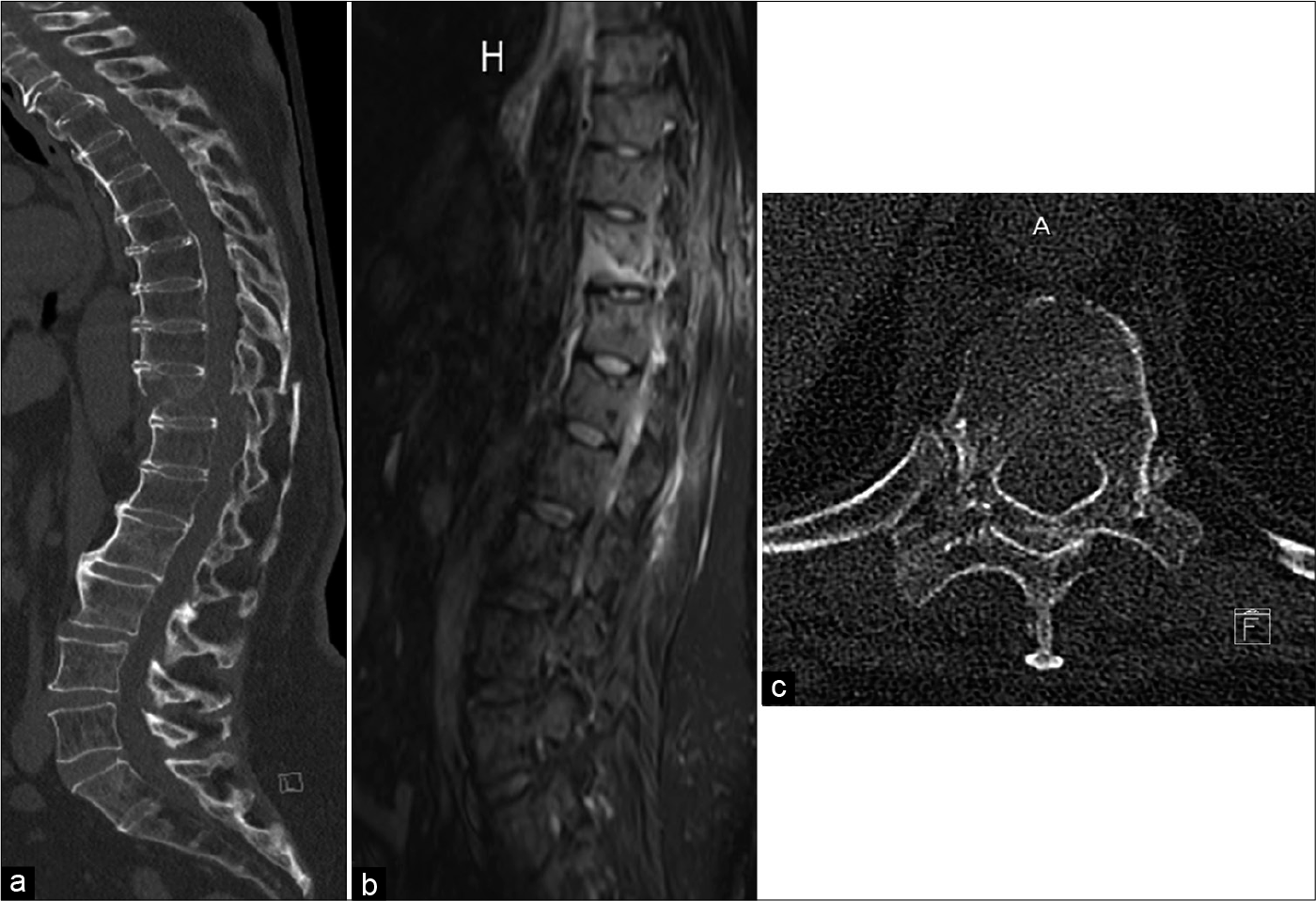
Figure 1:
(a) Computed tomography, sagittal view, transverse fracture of T11, subluxation of the vertebral body. (b) T2-weighted magnetic resonance imaging, sagittal view, injury of the posterior ligament complex. (c) Computed axial tomography, axial view, double image of vertebral laminae due to subluxation.
Surgery
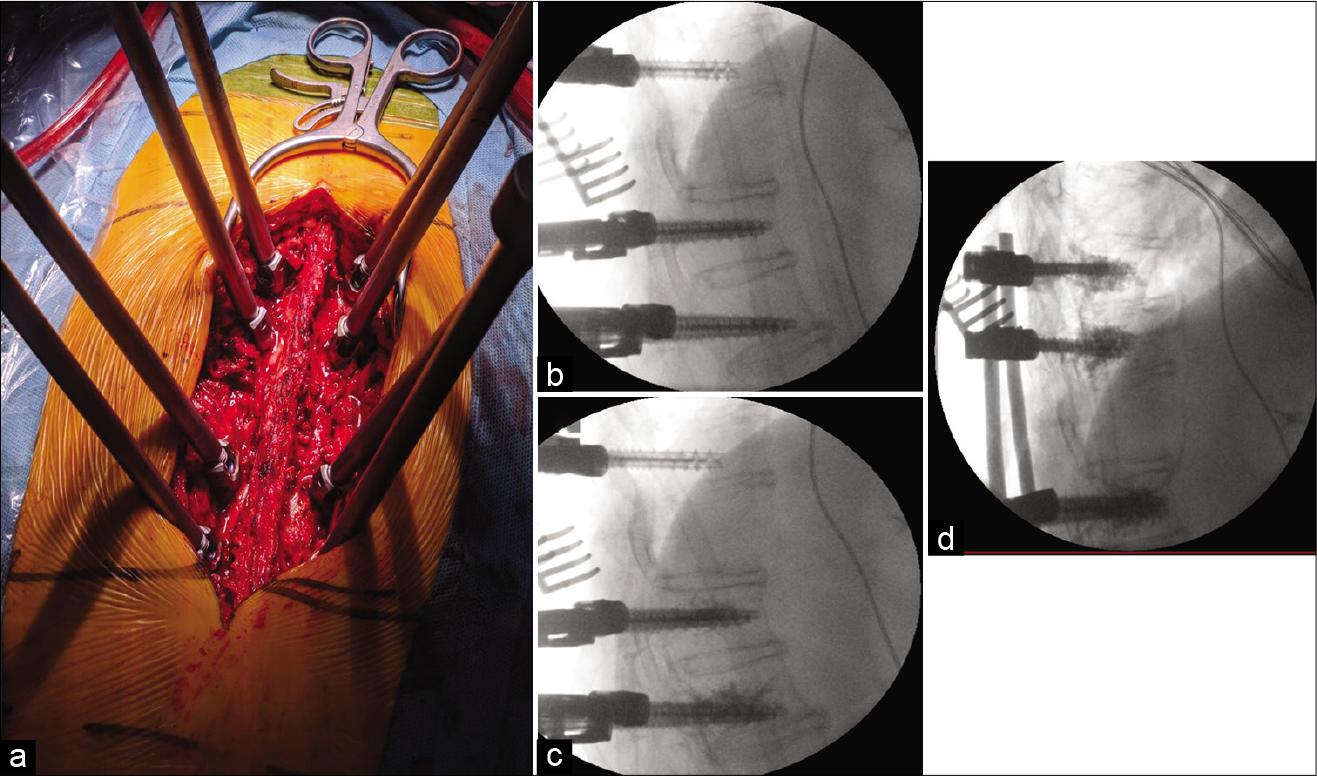
Three days later, she underwent a T11 hemilaminectomy to remove an epidural hematoma with T9 - T10 (5.5 mm × 40 mm screws) to T12 - L1 (6.5 mm × 45 mm screws) transpedicular instrumented fusion. Vertebral body augmentation with 1.5 mL of PMMA bone cement per transpedicular screw (distally fenestrated) was performed due to her underlying osteoporosis. When the fourth screw was placed, fluoroscopy showed leakage of PMMA cement into the paravertebral system [
The CT angiogram of the chest documented a cement pulmonary embolism [
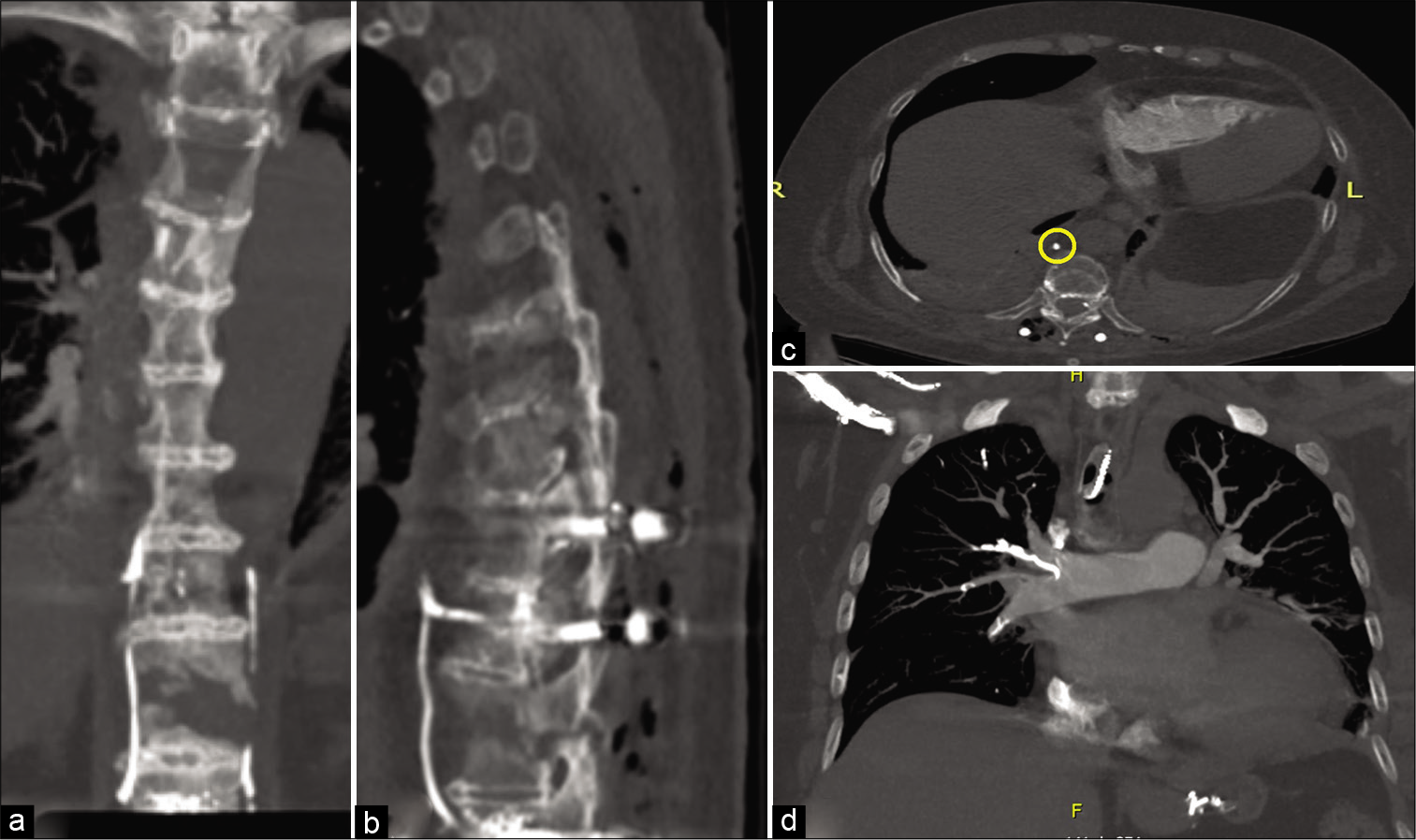
Figure 3:
Computed axial tomography Angiography, (a-c) Coronal, sagittal, and axial view (yellow circle), respectively where high density material is observed in the paravertebral venous system, is suggestive of cement embolus. (d) Presence of the high density material occupying the lumen of the subsegmental arterial vessels, in the apicoposterior segment of both upper lobes, anterior segment of the right upper lobe, lingula lobe, middle lobe, posterior and medial basal, segment of the right lower lobe.
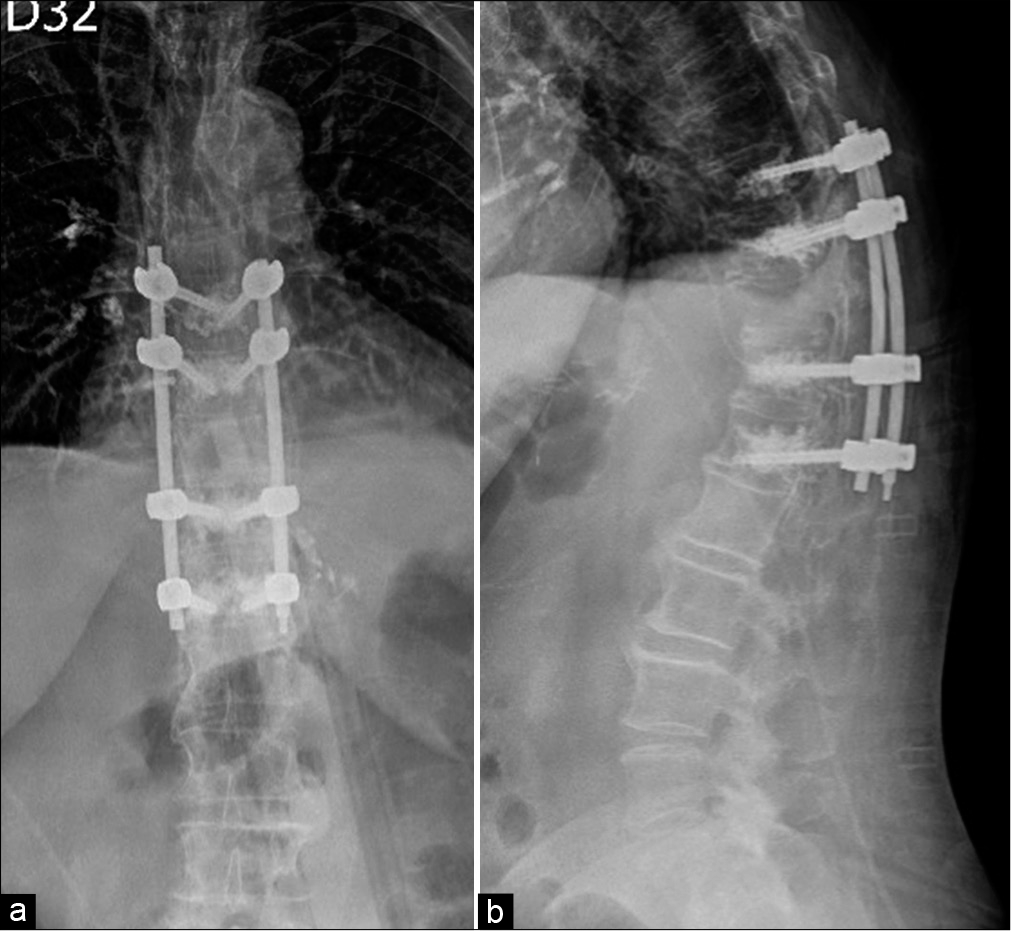
Figure 4:
Follow-up at 1 week after surgery. Instrumentation with transpedicular screws at T9, T10, T12 and L1 with polymethylmethacrylate augmentation. (a) Anteroposterior view, radiopaque image in right lung associated with cement emboli. (b) sagittal view radiopaque image which is correlated with cement leakage through the paravertebral venous system.
DISCUSSION
Symptomatic pulmonary embolism due to bone cement utilized to perform transpedicular screw fixation is rare, occurring in 1.4% of isolated cases.[
CONCLUSION
PMMA cementation continues to be a used in osteoporotic patients to increase pull-out resistance when placing transpedicular screws for thoracolumbar fractures/ fusions. Although cement leakage resulting in symptomatic pulmonary embolization following cemented PMMA transpedicular screw fixation is rare, it should be aggressively diagnosed and medically managed in every patient individually by an interdisciplinary team.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Andrä M, Baumer H, Mittergradnegger F, Laschitz M, Petek T, Wandschneider W. Life-threatening cardiac perforation after posterior spondylodesis. Ann Thorac Surg. 2017. 104: e355-7
2. Bopparaju S, Varon J, Surani S. Pulmonary embolism with vertebral augmentation procedures. Case Rep Pulmonol. 2013. 2013: 785307
3. Choe DH, Marom EM, Ahrar K, Truong MT, Madewell JE. Pulmonary embolism of polymethyl methacrylate during percutaneous vertebroplasty and kyphoplasty. AJR Am J Roentgenol. 2004. 183: 1097-102
4. Girardo M, Rava A, Fusini F, Gargiulo G, Coniglio A, Cinnella P. Different pedicle osteosynthesis for thoracolumbar vertebral fractures in elderly patients. Eur Spine J. 2018. 27: 198-205
5. Hemmer C. Abnormal chest X-ray and computed tomography post-lumbar fusion. J Nurse Pract. 2015. 11: 276-8
6. Ignacio JMF, Ignacio SD. Pulmonary bone cement embolism following pedicle screw instrumentation with bone cement augmentation for a burst fracture of l1 in a non-osteoporotic spine. Acta Med Philipp. 2013. 47: 76-9
7. Kerry G, Ruedinger C, Steiner HH. Cement embolism into the venous system after pedicle screw fixation: Case report, literature review, and prevention tips. Orthop Rev (Pavia). 2013. 5: 24
8. Krueger A, Bliemel C, Zettl R, Ruchholtz S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: A systematic review of the literature. Eur Spine J. 2009. 18: 1257-65
9. Liang TZ, Zhu HP, Gao B, Peng Y, Gao WJ. Intracardiac, pulmonary cement embolism in a 67-year-old female after cement-augmented pedicle screw instrumentation: A case report and review of literature. World J Clin Cases. 2021. 9: 3120-9
10. Özalay M, Özkoç G. Pulmonary cement embolism after segmental polymethyl methacrylate-augmented pedicle screw fixation. J Turk Spinal Surg. 2012. 23: 233-40
11. Rahimizadeh A, Hassani V, Soufiani H, Rahimizadeh A, Karimi M, Asgari N. Symptomatic pulmonary cement embolism after pedicle screw polymethylmethacrylate cement augmentation: A case report and review. Surg Neurol Int. 2020. 11: 1-4
12. Rasch A, Sindermann J, Scheld HH, Hoffmeier A. Pulmonary palacos embolism: A case report. Thorac Cardiovasc Surg. 2010. 58: 437-9
13. Röllinghoff M, Siewe J, Eysel P, Delank KS. Pulmonary cement embolism after augmentation of pedicle screws with bone cement. Acta Orthop Belg. 2010. 76: 269-73
14. Tang YC, Guo HZ, Guo DG, Luo PJ, Li YX, Mo GY. Effect and potential risks of using multilevel cement-augmented pedicle screw fixation in osteoporotic spine with lumbar degenerative disease. BMC Musculoskelet Disord. 2020. 21: 274
15. Tonolini M, Bianco R. Pulmonary cement embolism after pedicle screw vertebral stabilization. J Emerg Trauma Shock. 2012. 5: 272-3
16. Ulusoy OL, Kahraman S, Karalok I, Kaya E, Enercan M, Sever C. Pulmonary cement embolism following cement-augmented fenestrated pedicle screw fixation in adult spinal deformity patients with severe osteoporosis (analysis of 2978 fenestrated screws). Eur Spine J. 2018. 27: 2348-56
17. Venmans A, Lohle PN, van Rooij WJ, Verhaar HJ, Mali WP. Frequency and outcome of pulmonary polymethylmethacrylate embolism during percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2008. 29: 1983-5
18. Wang LJ, Yang HL, Shi YX, Jiang WM, Chen L. Pulmonary cement embolism associated with percutaneous vertebroplasty or kyphoplasty: A systematic review. Orthop Surg. 2012. 4: 182-9
19. Yazu M, Kin A, Kosaka R, Kinoshita M, Abe M. Efficacy of novel-concept pedicle screw fixation augmented with calcium phosphate cement in the osteoporotic spine. J Orthop Sci. 2005. 10: 56-61
20. Zheng N, Liang M, Zhang HD, Zhu SH, Yang TT, Zhuo L. Fatal extensive bone cement embolism: Histological findings confirmed by Fourier transform infrared spectroscopy. Forensic Sci Int. 2013. 229: e23-5

